Article Text

Abstract
Background To date, cognitive–behavioural therapy (CBT) trials have primarily focused on clinical recovery; however, personal recovery is actually the fundamental aspect of the recovery process. The aim of this study was to summarise and synthesise the existing evidence regarding the effectiveness of CBT for personal recovery in patients with schizophrenia.
Aim This study aimed to determine the effectiveness of CBT for personal recovery in patients with schizophrenia.
Methods A systematic search of the literature in PsycINFO, PubMed, Cochrane (CENTRAL), Embase and Web of Science (SCI) was conducted to identify randomised controlled trials reporting the impact of CBT interventions on personal recovery in patients with schizophrenia. The estimated effect sizes of the main study outcomes were calculated to estimate the magnitude of the treatment effects of CBT on personal recovery. We also evaluated the CBT’s effect size at the end-of-treatment and long-term (follow-up) changes in some aspects of personal recovery.
Results Twenty-five studies were included in the analysis. The effect of CBT on personal recovery was 2.27 (95% CI 0.10 to 4.45; I2=0%; p=0.04) at post-treatment and the long-term effect size was 2.62 (95% CI 0.51 to 4.47; I2=0%; p=0.02). During the post-treatment period, the pooled effect size of CBT was 0.01 (95% CI −0.12 to 0.15; I2=33.0%; p>0.05) for quality of life (QoL), 0.643 (95% CI 0.056 to 1.130; I2=30.8%; p<0.01) for psychological health-related QoL, −1.77 (95% CI −3.29 to −0.25; I2=40%; p=0.02) for hopelessness and 1.85 (95% CI 0.69 to 3.01; I2=41%; p<0.01) for self-esteem. We also summarised the effects of CBT on QoL (subscale scores not included in the evaluation of the pooled effect size), self-confidence and connectedness, and all results corresponded to positive effects. However, there was insufficient evidence regarding the long-term effects of CBT on personal recovery.
Conclusions CBT is an effective therapy with meaningful clinical effect sizes on personal recovery and some aspects of personal recovery of schizophrenia after treatment. However, the effect is relatively immediate and rapidly decreases as time progresses. Therefore, in the future, more studies should focus on the mechanism of CBT for personal recovery and the factors that influence the long-term effects of CBT.
Trial registration number CRD42018085643.
- cognitive–behavioural therapy
- schizophrenia
- personal recovery
- systematic review
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Schizophrenia, a severe mental illness, affects more than 21 million people worldwide.1 The persistent negative symptoms and cognitive impairment associated with schizophrenia have led to its classification among the top 25 leading causes of disability worldwide and the top 11 leading causes of reduced years lived with disability in 2013.2 The WHO’s Mental Health Action Plan 2013–2020 highlights the steps required to provide appropriate services for people with schizophrenia.3
Cognitive–behavioural therapy (CBT) is the primarily recommended psychological treatment for schizophrenia according to major guidelines.4 5 Abundant studies have proven that the effects of CBT on reducing positive symptoms,6 improving negative symptoms,7 conferring functional improvement,8 reducing the time of relapse9 and reducing suicidal ideation10 in patients with schizophrenia are significant. However, the remission of clinical symptoms does not meet the criterion for rehabilitation, and patient organisations have emphasised that recovery can occur even when psychotic symptoms are persistent.11 Recovery is an ongoing, complex and multidimensional process. According to different perspectives, schizophrenia recovery can be classified as clinical and personal.12 In the treatment of patients with schizophrenia, the primary goal traditionally is the clinical recovery. Clinical recovery includes remission of symptoms and functional improvement, which is the premise of other non-pharmacological treatments and rehabilitations. The relationship between the clinical and personal recovery is somewhat correlated, and both should be considered when monitoring the treatments and outcomes of patients with schizophrenia.13 The term ‘personal recovery’, which based on the perspective of individuals who have experienced mental illness,14 has been widely used in the literature to describe the patient-based definition of recovery.15 The most frequently cited patient-based definition is ‘the development of new meaning and purpose in one’s life as one grows beyond the catastrophic effects of mental illness.’16
Personal recovery varies from person to person, and it is difficult to define common characteristics. Different researchers also have their own definitions of personal recovery. Andresen et al 17 concluded that personal recovery included four key points: finding hope; re-establishing identity; finding meaning in life; and taking responsibility for recovery. Leamy et al 18 posited that the categories of personal recovery encompass connectedness, hope, identity, meaning and empowerment. Based on a cluster analysis of self-reported personal recovery-related variables, Rossi et al 19 identified resilience, self-esteem, coping strategies, stigma and personal strength. Furthermore, quality of life (QoL),20 21 taking control of one’s life,22 23 personal confidence and reliance on others24 have been found to be important components of personal recovery.
According to a review of the abundant literature on personal recovery, which have most consistently identified connectedness, hope and empowerment as relevant categories,13 and discussions by our research team, we decided to use the CHIME personal recovery model defined by Leamy et al 18: Connectedness–Hope–Identity–Meaning–Empowerment. In addition, this model is consistent with the context of recovery defined by the WHO.25 Based on the progress of pharmacological treatment of acute psychiatric symptoms of schizophrenia, QoL measurement has become an important indicator for evaluating clinical outcomes in patients with schizophrenia.26 Furthermore, QoL is one of the most commonly used outcome assessments. To better address the concept of personal recovery, we have also considered QoL in the assessment of personal recovery.
The concept of recovery is multidimensional; why, then, should personal recovery be the primary focus? Personal recovery pertains to patients’ ability to live a favourable, dignified and meaningful life. It is the core element of recovery from the patient perspective, and it is the ultimate aim of mental illness treatment. Moreover, some components of personal recovery, such as hope, are the foundations and preconditions of treatment and other outcomes.27 In addition, Jahn et al’s28 finding suggests that personal recovery is a protective factor against suicidal ideation in individuals with schizophrenia. However, existing knowledge about the role of CBT in personal recovery is highly limited, and the current meta-analyses focused only on clinical outcomes;29 30 therefore, the aim of this study was to determine the effectiveness of CBT for personal recovery in patients with schizophrenia. This research has been registered at PROSPERO (CRD: 42018085643), and the study protocol can be obtained via the following website: https://www.crd.york.ac.uk/PROSPERO/%23recordDetails.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement31 were followed in all steps of this research.
Search strategy
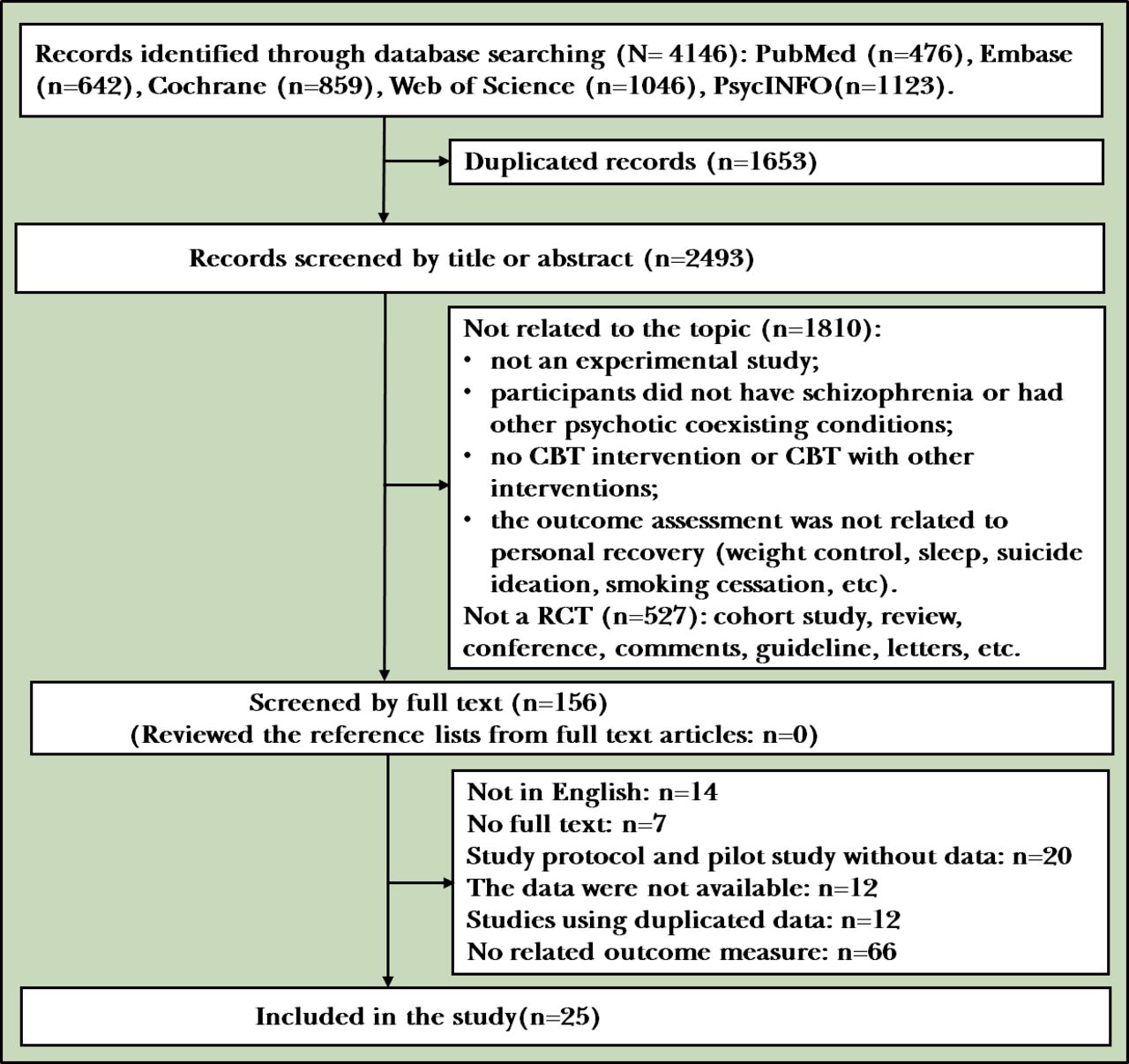
Five electronic databases, PsycINFO, PubMed, the Cochrane Library (CENTRAL), Embase and Web of Science (SCI),were searched for relevant papers published before 31 December 2018 with the following search terms: (‘psychosis’ OR ‘psychotic’ OR ‘schizophrenia’ OR ‘schizoaffective disorder’) AND (‘cognitive therapy’ OR ‘cognitive behavior* therapy’ OR ‘cognitive behaviour* therapy’ OR ‘CBT’) AND (‘random’ OR ‘randomized control trial’ OR ‘clinical trial’ OR ‘trial’). Manual searches were also performed by reviewing the reference lists of related papers. Two reviewers (WW and NC) independently screened the search results by reviewing titles and abstracts. The full texts of relevant articles screened in previous step were downloaded for further screening. If the same data were reported in more than one publication, only the paper with the more complete data set was included. Any disagreement was settled by discussion with the third author (ZY). (See the flow chart of the study, figure 1.)

The flowchart of search and study selection. CBT, cognitive–behavioural therapy; RCT, randomised controlled trial.
Inclusion and exclusion criteria
The definition of personal recovery in our study included six components: connectedness, hope,identity,meaning,empowerment; and QoL. Studies that fulfilled the following criteria were included: (1) randomised controlled trials; (2) publications with full texts written in English; (3) participants diagnosed with schizophrenia or schizophrenia spectrum disorder based on the International Classification of Diseases-Tenth Revision or Diagnostic and Statistical Manual of Mental Disorders-Fourth/Fifth Edition; (4) the use of a valid measure to assess personal recovery (CHIME and QoL); and (5) a psychological intervention of CBT or a CBT-modified programme, but not in combination with other psychological interventions.
The exclusion criteria were as follows: (1) no relevant data available for further analysis; (2) article types other than randomised controlled trials (RCT), such as comments, letters and reviews; and (3) other cognitive therapies, such as cognitive training, cognitive–behavioural social skills training, cognitive remediation therapy or cognitive enhancement therapy.
Data extraction
Data extraction was performed by two independent reviewers (WW and NC) who used a specific worksheet designed before the literature search to minimise errors in data extraction. Data extraction was conducted using the full-text versions of the RCTs. The data regarding basic characteristics and outcome measures, including study identity (first author, publication year and country); study design (randomisation, concealment of allocation, blinding); patients (number of study participants, mean age); intervention characteristics (treatment protocol, length of treatment, number of sessions and type of comparisons); and all relevant outcomes (types of outcome measures, instruments and follow-up periods) were extracted from all included studies.
Quality assessment
The quality of the RCTs enrolled in our study was assessed using the Cochrane Collaboration’s tool for determining the risk of bias in randomised trials.32 According to the Cochrane assessment tool, the relevant information was extracted from each study, and the study was rated as ‘high risk’, ‘low risk’ or ‘unclear risk’. Disagreements were resolved by consensus.
Statistical analysis
All the pooled effect size was performed by RevMan V.5.0. The I2 statistic was used to evaluate the heterogeneity of the studies. Sensitivity analysis and subgroup analysis were performed to deal with heterogeneity. Forest plots were also drawn to visualise the extent of heterogeneity across studies. Publication bias was evaluated using Egger’s test by Stata (V.14.2). Hedge’s g was used to determine the effect size of continuous outcomes. Considering the heterogeneity of the personal recovery outcome measures, we summarised the pooled results narratively with descriptive statistics and textual descriptions. A two-tailed p<0.05 was considered statistically significant. A power analysis to examine the reliability of the pooled result was performed with GPower V.3.1.
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was performed to assess confidence of evidence (CoE) for each comparison. CoE of outcomes was rated based on study design, risk of bias, inconsistency of results, indirectness of evidence, imprecision and publication bias. We used the GRADEpro Guideline Development Tool to assess the CoE of the critical outcomes.
Results
Study selection
A total of 4146 articles were retrieved from the electronic databases. After duplicates were discarded, 2493 remaining studies were screened. According to the inclusion and exclusion criteria, approximately 2337 records were removed after screening to determine whether the article titles and abstracts were relevant to the topic of the review. The full texts of the remaining 156 studies were reviewed. We manually searched by reviewing the reference lists from the full-text articles, and none of the references were related to the topic. Finally, 131 studies did not meet the inclusion criteria, leaving 25 studies for inclusion in this review. The details of the search process are shown in figure 1.
Study characteristics
All the participants included in the 25 studies33–57 were diagnosed with schizophrenia or schizoaffective disorders; the patients in seven studies were recruited from hospitals, and the patients in the other 18 studies were recruited from the community or mental health centres. The intervention treatment provided in most of the studies was CBT; 1 of the 25 studies44 used cognitive–behavioural oriented services (CBOS) as the intervention group’s treatment, but CBOS is still considered as CBT on the basis of its core theory and implementation. All the comparison groups received treatment as usual, support groups, standard care, standard treatment (ST), standard support, befriending, wait-listing or patient psychoeducation therapy, except in two studies37 53 that compared CBT versus CBT plus clozapine and CBT versus CBT plus thioridazine. Three studies53 54 57 reported directly the personal recovery using the Questionnaire about the Process of Recovery (QPR) scale, 11 studies33 35 37 40 43 50 51 53–56 reported QoL; 5 studies34 36 45–47 reported hope as an outcome of personal recovery; self-esteem, a core element of a better and more meaningful life for psychiatry patients, was measured in 11 studies34 39 41 42 45–49 52 57; 3 studies39 44 55 reported relationships with others as an outcome; and 1 study39 reported self-confidence as an outcome of personal recovery. No studies reported empowerment as an outcome. Twelve of the studies reported sufficient follow-up data to evaluate the long-term effect of CBT in schizophrenia (table 1).
Characteristics of the included studies
Quality of the studies
The risk of bias for each study is available in the online supplementary material 1. Eleven35 36 38 39 42 48 50 51 53–55 of the 25 studies were universally assessed as having a low risk of bias across all domains. Fifteen trials35 36 38 39 42 44 45 48 50 51 53–57 employed adequate methods of sequence generation, 10 trials31 33 34 37 40 43 46 47 49 52 were not clear. In addition, the risk of bias due to inadequate allocation concealment was unclear in seven trials,34 37 40 43 45 46 52 and four 33 41 47 49 trials did not include allocation concealment. Lack of blinding of the assessors led to a high risk of bias for some outcomes in four studies,41 42 44 47 and an unclear risk in four studies.33 37 43 52 A high risk of bias due to lack of participants or staff blinding was found in two studies33 47 and was unclear in three studies.37 43 52 There was a high risk of bias due to incomplete outcome data for two of the included trials;43 45 one trial44 did not report all outcomes.
Supplemental material
Main efficacy meta-analysis
Primary outcome
Three studies53 54 57 reported the effect of CBT for personal recovery measured by QPR. The random effects meta-analysis yielded a summary effect size of 2.27 (95% CI 0.10 to 4.45; I2=0%; p=0.04, power=0.61). Egger’s test indicated that there was no publication bias (p=0.96, 95% CI −18.14 to 17.96). The long-term effect of CBT was measured in these three studies and the pooled effect size was 2.62 (95% CI 0.51 to 4.47; I2=0%; p=0.02, power=0.13) (figure 2).

Forest plot of the effect of cognitive–behavioural therapy (CBT) on personal recovery.
Secondary outcomes
Effect size of QoL
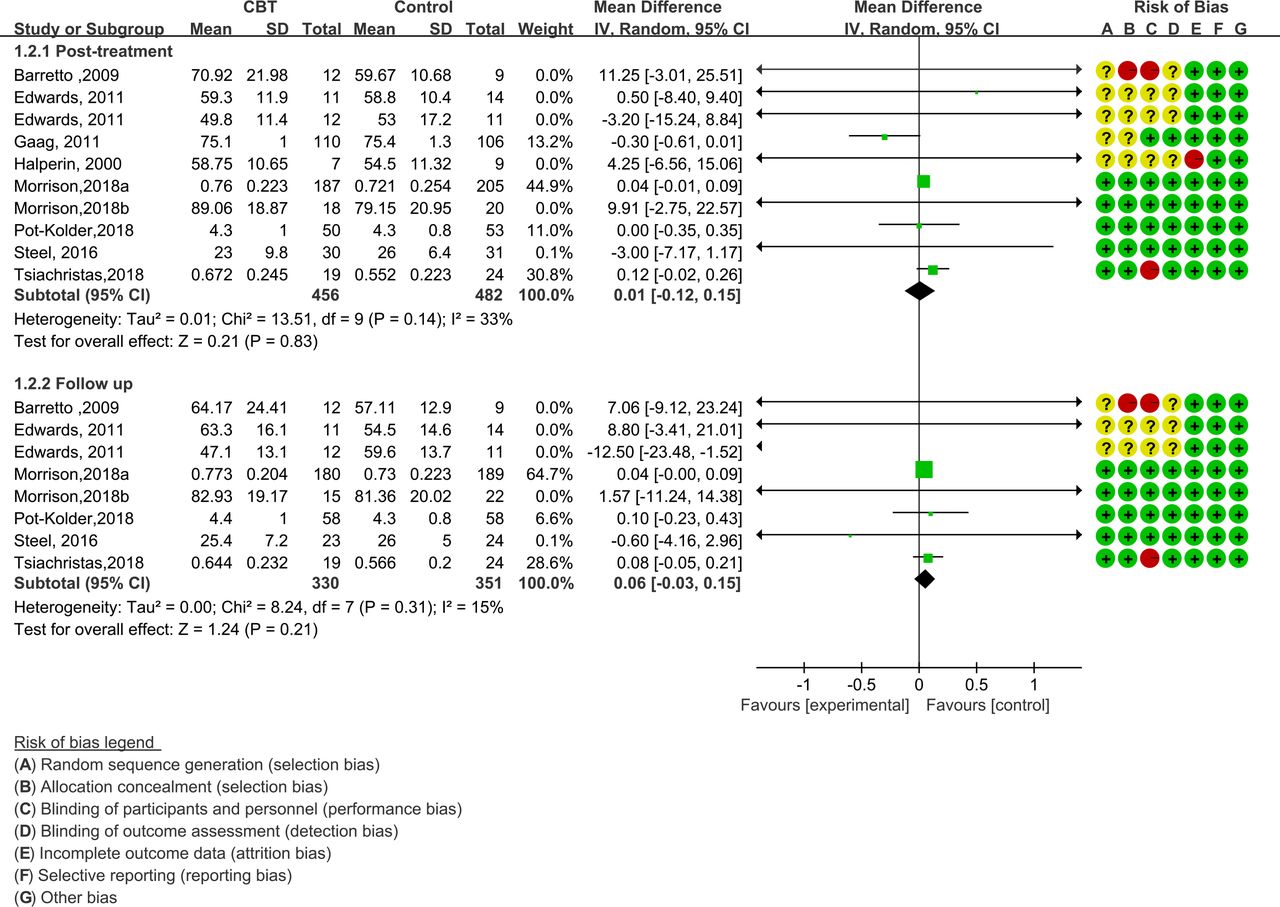
Nine studies33 37 40 43 51 53–56 reported QoL total scores based on questionnaires. The random effects meta-analysis yielded a summary effect size of 0.01 (95% CI −0.12 to 0.15; I2=33.0%; p>0.05) and a power analysis result of 0.97 (figure 2). Egger’s test indicated that there was no publication bias (p=0.54, 95% CI −1.40 to 2.48). The participants in three studies40 43 54 were recruited from hospitals, and the participants in six studies were recruited from outside the hospital. Both the inpatient and outpatient subgroups yielded a small and non-significant effect of schizophrenia on QoL (online supplementary material 1). Seven studies33 37 51 53–56 reported CBT follow-up for QoL in schizophrenia, and the pooled effect size was 0.06 (95% CI −0.03 to 0.15; I2=15%; p>0.05) with a small power of 0.19. The follow-up times differed among the studies (1 month;33 3 months;37 55 56 6 months and above51 53 54). We evaluated the effect sizes using Cohen’s d, and the pooled effect sizes were 0.36 (1 month), 0.08 (95% CI −0.31 to 0.47; I2=57.0%; p>0.05, power=0.87) (3 months) and 0.04 (95% CI −0.00 to 0.09; I2=0%; p=0.05, power=0.11) (6 months and above) respectively. After performing the sensitivity analyses, no substantial change in the new pooled effect size was observed.
Four studies35 38–40 reported the psychosocial well-being of the patients, as measured by the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS), a subscale of the Modular System for Quality of Life (MSQoL) scale and the WHO-QoL psychological well-being subscale. Because of the high heterogeneity (I2=91.0%, p<0.001), it was not appropriate to directly combine the effect sizes; thus, a descriptive analysis was performed. Two studies investigated psychological health with WEMWBS;38 39 the pooled effect size was 0.64 (95% CI 0.06 to 1.13; I2=30.8%; p<0.01) and the long-term effect size was 0.38 (95% CI 0.08 to 0.69; I2=0.00%; p<0.01). In a restrictive and high-quality RCT, Bechdolf et al 35 investigated the effect of CBT on patients’ psychosocial well-being using a subscale of the MSQoL. The results showed that the CBT programme improved the patients’ psychological health-related QoL with a small effect size (Cohen’s d=0.03). Moreover, the long-term effect of CBT was significant according to data collected 4 months after treatment and it had a moderate effect size (Cohen’s d=0.37). van der Gaag et al 40 used the WHO-QoL psychological well-being subscale to reflect the psychological health of patients with schizophrenia. The results showed that CBT significantly improved the patients’ QoL, with a large effect size at the end of treatment (Cohen’s d=1.41).
Shawyer et al 50 investigated QoL using two subscales from the Quality of Life Enjoyment and Satisfaction Questionnaire: Subjective Feelings and General Activities. In addition, the endpoint effect sizes of the two subscales corresponded to Cohen’s d values of 0.02 and 0.43, and the follow-up effect sizes were −0.48 and 0.14 respectively. The study also evaluated the life satisfaction and life enjoyment with special items, and the Cohen’s d values were 0.37 and 0.08 with long-term effect sizes of 0.20 and −0.19 respectively. Bechdolf et al 35 reported subjective QoL measured with the MSQoL-seven subscale scores at post-treatment and at a 6-month follow-up. The effect sizes of the seven subscales (endpoint, follow-up) were as follows: Physical Health (0.11, 0.21), Vitality (0.01, 0.36), Psychosocial QoL (0.03, 0.37), Affective QoL (0.17, 0.27), Material QoL (0.03, 0.12), Spare Time QoL (0.30, 0.32) and General QoL (0.07, 0.20). All changes in the effect sizes over time were positive.
Effect size of hope
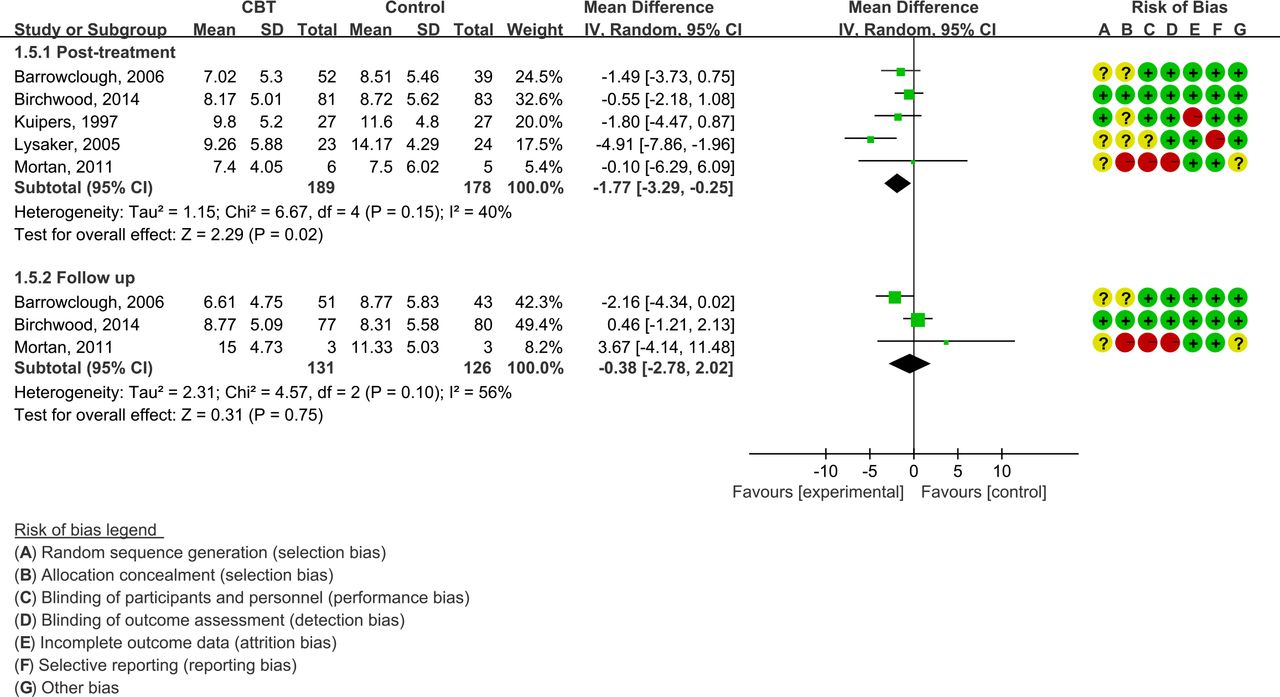
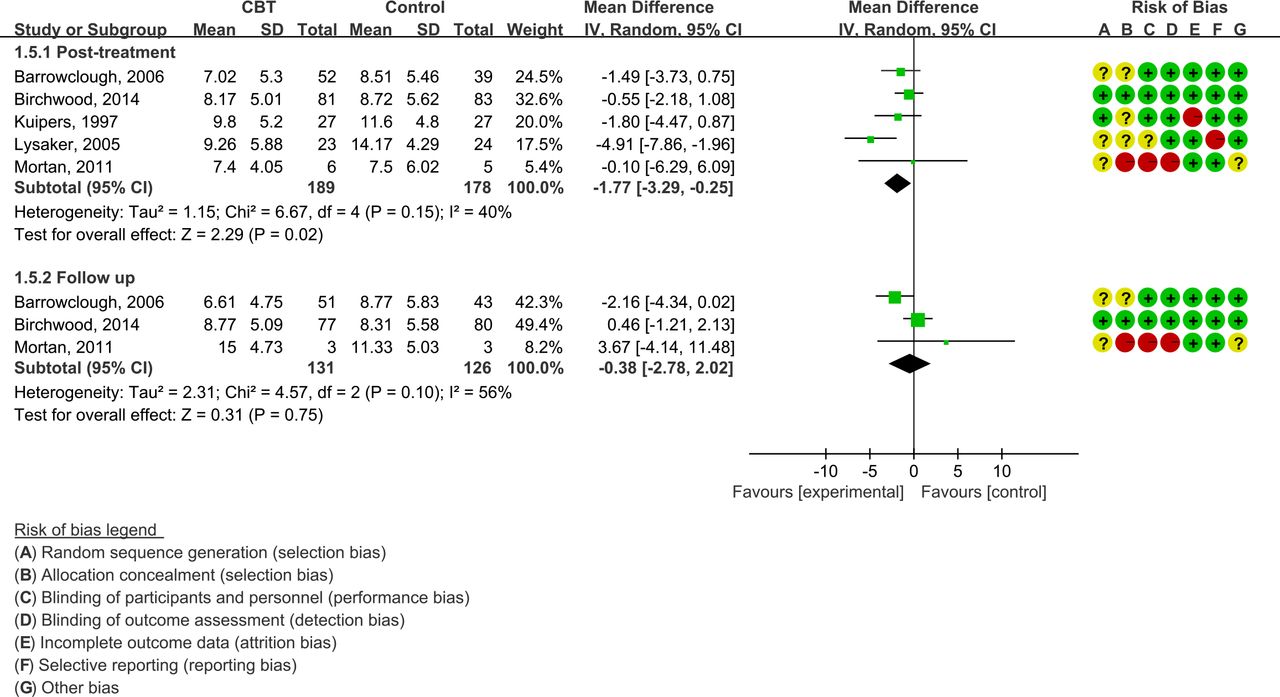
A total of five studies34 36 45–47 investigated the hopelessness levels of patients with schizophrenia using the Beck Hopelessness Scale (BHS), for which higher scores indicate lower hope levels. Egger’s test showed that no publication bias existed (p=0.72, 95% CI −5.65 to 7.23). The endpoint pooled effect size of the five studies was positive, with an effect size of −1.77 (95% CI −3.29 to -0.25; I2=40%; p=0.02, power=0.89) (figure 3). Regarding the long-term effect of CBT, three studies34 36 47 reported follow-up data for over 6 months after the treatment. The results showed that the effect of CBT on improving hope among patients with schizophrenia was uncertain (−0.38, 95% CI −2.78 to 2.02; I2=56%; p>0.05), and the three studies only yielded a power of 0.42. Sensitivity analyses were conducted and after eliminating the studies, no substantial change in the new pooled effect size was observed (figure 4).
Forest plot of the effect of cognitive–behavioural therapy (CBT) on quality of life (QoL).
Forest plot of the effect of cognitive–behavioural therapy (CBT) on hopelessness.
Effect size of identity (self-esteem and self-confidence)
A total of eleven studies34 39 41 42 45–49 52 57 reported self-esteem. The total sample size of these eleven studies was 584, and the pooled effect size was 1.85 (95% CI 0.69 to 3.01; I2=41%; p<0.01, power=0.98) (figure 5). The result of Egger’s test showed that there was no publication bias (p=0.20, 95% CI −3.92 to 0.94). For the long-term effect size of CBT, six34 39 42 47 48 57 of the ten studies completed a follow-up evaluation and the effect size was −1.21 (95% CI −2.45 to 0.04; I2=12%; p>0.05, power=0.37). Two39 57 of those studies reported results 1 month after the end of treatment, which showed an uncertain effect of CBT (3.61, 95% CI −13.89 to 21.11; I2=28%; p>0.05, power=0.11) and the statistical power was 0.11. For the other four studies, the follow-up time was over 6 months. Therefore, we combined the follow-up data from these four studies and it revealed a negative long-term effect, with an effect size of −1.23 (95% CI −2.52 to 0.06; I2=22%; p>0.05) and a power of 0.49.

Forest plot of the effect of cognitive–behavioural therapy (CBT) on self-esteem.
One study39 assessed the patients’ self-confidence using the Brief Core Schema Scales (BCSS). The BCSS is designed to assess negative and positive beliefs about oneself and others. The endpoint effect size of positive beliefs corresponded to Cohen’s d of 1.14, but the long-term effect size was only 0.20 at 1 month after treatment. The endpoint effect size of negative beliefs corresponded to Cohen’s d of 0.40, and the long-term effect size was 0.09.
Connectedness
The Social Comparison Scale is used to assess the patient’s relationship with others, and higher scores indicate a more positive view of oneself in relation to others.39 The effect sizes were 0.79 and 0.33 at the endpoint and follow-up respectively. Klingberg et al 44 investigated the effect on social connections of CBT in schizophrenia by the percentage of connections with relatives after CBT treatment, and the result showed significantly more improvement than deterioration regarding social contacts in the CBT group, with 15 of 61 patients exhibiting positive changes after CBT compared with 13 of 60 patients in the control group.
Figure 6 shows the trend of the effect of CBT on personal recovery over time from the end of treatment, visually showing the characteristics of CBT long-term effects. Summary of findings tables summarising CoE assessment based on the GRADE approach are shown in table 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The change in effect size over the follow-up period. Zero on the x-axis indicates the endpoint of treatment.
GRADE summary of evidence for the effects of CBT and personal recovery
Discussion
Main findings
There has recently been growing attention surrounding the effects of CBT on personal recovery in patients with schizophrenia. The present review examined the efficacy of CBT across 25 randomised clinical trials that included multiple outcomes of personal recovery over different periods of follow-up. Both the post-treatment and the follow-up effect of CBT on personal recovery measured by QPR were positive and significant, which means that CBT can indeed change the patient’s recovery process to some extent. However, due to the limited number of studies, the small sample size and low statistical power, the evidence is not sufficient. We also tested the effect of CBT on the specific components of personal recovery. At post-treatment and during the follow-up period, the effect of CBT on QoL in patients with schizophrenia was uncertain for both pooled groups and subgroups, with p values >0.05 and powers <80%. Thus, a conclusion cannot be drawn as to whether CBT is beneficial for patients’ QoL due to the limited number of studies, the small sample sizes and the fair quality of the included controlled trials. Additional sufficient and conclusive evidence is needed in the future.
However, for psychological well-being, which is an important component of QoL, the pooled endpoint effect size was significantly large (>0.6), although the long-term effect size decreased to a moderate level. The Subjective Feelings (how much of the time participants feel positive) and General Activities (degree of satisfaction with general activities of life) of patients also showed improvement at post-treatment but decreased at long-term follow-up times. Although this change in effect size with time is in contrary to the trend reported by Bechdolf et al,35 we still believe that CBT is a useful intervention for improving QoL other than psychological health-related QoL in patients with schizophrenia. However, the effect of CBT on QoL in schizophrenia and whether the long-term effect is better or worse than the endpoint should be explored in the future.
The effect of CBT on hope and self-esteem is obvious and positive at post-treatment; however, the long-term effect (over 6 months) is markedly decreased. The self-confidence and relationships of patients with schizophrenia improved little in the CBT group compared with the ST group, and the long-term effect of CBT was the same for hope and self-esteem. These data indicate that the effect of CBT on personal recovery is only sustained for a short time; as time progresses after treatment, the personal recovery of the patients reverts back to the original level. Most studies have only focused on the immediate effects of targeting cognitions about the self and have not tried to determine which specific intervention techniques may change the underlying mechanism.39 We believe that the personal recovery of patients should be a long-term effort, whether in or out of the hospital, and to maximise the effectiveness of CBT, more efforts should be dedicated to continuing CBT interventions at specific time points when its effects are decreased and to determining which factors influence its effects.
None of these studies reported the effect of CBT on meaning and empowerment in patients with schizophrenia. Empowerment includes participating in society in terms of access to employment, education and other valued resources; in terms of interpersonal characteristics, empowerment also means having control over one’s life and the recovery process or efforts to achieve greater control and self-efficacy. There are also some scales available for measuring empowerment, especially among patients with psychosis.58 Unfortunately, none of the studies included in our research used the empowerment scale as a measure of personal recovery. In the CHIME personal recovery model, meaning is not reported directly, and to the best of our knowledge, there is no specially designed scale for meaning measurement; however, the schizophrenia hope scale designed by Choe59 examines positive expectations for the future, confidence in life and the future, and meaning in life, which may help to reflect meaning as an aspect of personal recovery in patients with schizophrenia. Meaning and empowerment can reflect personal recovery to a large extent, and future studies should be designed to verify the effectiveness of CBT on these components of personal recovery. Moreover, such studies would support the implementation of instruments to measure personal recovery as an outcome.
In the present study, even when strict inclusion criteria were applied to minimise the heterogeneity of the meta-analysis, there was still moderate or even large heterogeneity in some of the outcome analyses. Because of the small number of studies in the high heterogeneity group, the sensitivity analyses and the subgroup analysis were unable to compensate for the heterogeneity; therefore, instead of reporting the results of the meta-analysis, we reported the data as descriptive statistics. Additionally, the outcomes in our study are the best defined main measures for personal recovery, despite the moderate heterogeneity of some analyses. The uniformity among estimates of the effect was remarkable given the unavoidable differences in interventions associated with the different individual personnel delivering the behavioural interventions. In addition, we found no statistical evidence of publication bias, therefore such factors are unlikely to have affected our estimates.
Some of the results were not statistically significant, with p values >0.05. However, the absence of statistical significance should never be interpreted as evidence that an effect is absent. We performed a power analysis to test the reliability of the negative result, and the statistical power was low or very low. According to the significance test ( ), the effect size (M) is the important factor that determines the p value, and the factors that control the power are the same as those that control the significance60 (Chapter 29). Therefore, additional higher power studies with restrictive designs and sufficient sample sizes are needed in the future to confirm the effectiveness of CBT on personal recovery in schizophrenia.
), the effect size (M) is the important factor that determines the p value, and the factors that control the power are the same as those that control the significance60 (Chapter 29). Therefore, additional higher power studies with restrictive designs and sufficient sample sizes are needed in the future to confirm the effectiveness of CBT on personal recovery in schizophrenia.
Limitations
There are several limitations of this review. First, some subgroup analyses were not performed due to the limited number of studies. We found that the frequency and number of CBT sessions varied among studies . We initially planned to perform a subgroup analysis according to session design to determine which CBT design corresponds to the best outcome; however, because of the limited number of studies, this subgroup analysis was inappropriate. Therefore, we did not perform this analysis, although this issue could be discussed in future studies aimed at other recovery outcomes. Second, we could not perform a meta-analysis of some outcomes, thus the findings of the effects of CBT are less conclusive and valid. Third, we could not consider all aspects of personal recovery due to the absence of various measures in primary studies. The hope level was represented by the BHS score, which may not be ideal as there is a special hope scale designed for patients with schizophrenia.59 Fourth, this review included randomised controlled trials but did not include other study methods/designs or studies that used mixed methods or qualitative exploratory approaches. This limits the comprehensiveness and depth of the understanding of the process, the perceived benefits and different clinical outcomes of CBT on the personal recovery of patients with schizophrenia. Lastly, the review only included experimental studies published in peer-reviewed journals using English language. This could limit the generalisability and validity of the findings of this review.
Implications
There is insufficient evidence regarding the significant positive long-term effects of CBT on personal recovery outcomes among people with schizophrenia, and more experimental trials with high power are needed in the future. In our study, the QoL and CHIME recovery models were combined to represent personal recovery. However, there are numerous specialised scales designed to measure personal recovery among patients with schizophrenia, and future studies should take these scales into consideration as personal recovery measurement tools.13 Other important questions for both research and clinical applications that must be investigated include how long the effect of CBT can be sustained and how to ensure that patients with schizophrenia receive the greatest benefit from CBT intervention in the long term.
Conclusion
Our review showed that CBT is a reasonably effective treatment for some aspects of personal recovery among patients with schizophrenia. Our findings revealed improvements in QoL, hope, self-esteem, self-confidence and social connections after CBT interventions; however, the effect was relatively immediate and rapidly decreased over time. Therefore, in the future, more studies should focus on the mechanism of CBT for personal recovery and the factors that influence the long-term effects of CBT.
Acknowledgments
We thank Lynne Hyman and Kimberly Yasutis, PhD, from American Journal Experts for editing a draft of this manuscript.
References
Weiliang Wang graduated from Xinxiang Medical University of Henan province in 2016. Since 2016, he has been working on successive postgraduate and doctoral programs for Ph.D degree in Harbin Medical University, School of nursing. His research team is currently investigating how to slow down and prevent schizophrenia disability and maintain its social function. In recent years, attention has been paid to the treatment, clinical outcomes and rehabilitation of patients with schizophrenia. They are very interested in the personal recovery of mental illness, the development of clinical assessment tools, and the trajectories of disease development and its relationship with clinical outcomes, brain function and event-related potential studies. His research interest includes mental illness and psychotherapy.

Footnotes
Contributors WW and ZY designed the study and contributed substantially to the design of the search strategy. WW and NC searched the literature and extracted the data. DL performed the analysis and interpreted the data. WW wrote the first draft of the manuscript and YZ critically reviewed the manuscript. All authors read and approved the final manuscript.
Funding This work was supported by the National Natural Science Foundation of China (Grant No: 71673070).
Disclaimer The sponsor had no role in the study design, writing of the manuscript, or decision to submit this or future manuscripts for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data generated or analysed during this study are included in this article.