Article Text

Statistics from Altmetric.com
Introduction
Gender dysphoria (GD), or gender identity disorder, is defined as persistent distress stemming from the incongruence between one’s assigned sex at birth and gender identity.1 GD has traditionally been introduced as a rare condition predominant in assigned males at birth (AMABs).2 However, recent studies have shown an upward trend in assigned females at birth (AFABs) with a dramatic reversal of the AMAB:AFAB ratio.3–5 The actual AMAB:AFAB ratio varies by age group and study population.4–6 Questions have been raised concerning the increasing number of youth who seek professional care for GD, especially adolescent AFABs.7
Current GD studies are significantly limited by small sample sizes, short follow-up periods, or out-of-date data sets. In this study, we analysed data from multiple healthcare organisations between 2017 and 2021. Our aims were to uniquely illustrate an updated epidemiological trend by providing an estimated prevalence of GD and explore how sex assigned at birth and age influence GD.
Methods
Data and study design
We conducted a retrospective review of the TriNetX database Research Network in April 2022. This database provides access to de-identified electronic medical records. Available data include diagnoses, procedures, medications, laboratory values and genomic information from approximately 66 million patients from 49 healthcare organisations. Data sources included inpatients and outpatients from hospitals, primary care and speciality clinics. Most data were obtained from large academic medical institutions and their affiliated facilities. Approximately 80% of the patients were in the United States of America (USA). The Carilion Clinic Institutional Review Board designated the study as non-human subject research (NHSR) due to the de-identification of patient information inherent in TriNetX.
Sampling
Study subjects were defined as patients aged 4–65 with a diagnosis of gender identity disorder (International Statistical Classification of Diseases, ICD-10: F64). Patients with GD were compared with all patients aged 4–65 in the database. We applied all the available ICD-10 codes, visit codes, current procedural terminology (CPT) codes, collection of standardised codes that represent medical procedures, supplies, products and service (HCPCS) codes as well as medication codes to identify patient population size in the database in each survey year.8 We obtained patient information from 30 April 2017 to 30 April 2022, including assigned sex at birth and age per year. Each survey year was defined as the year following 30 April. For example, the survey year 2017 indicated 30 April 2017 to 30 April 2018.
Statistical analyses
We used TriNetX analytics, the built-in analytic tool of the TriNetX database, to analyse the characteristics of subjects by applying Fisher’s exact test for categorical variables and t-test for continuous variables. We compared baseline characteristics, including age, sex, ethnicity and race, for patients diagnosed with GD and all the other patients available in the database. Statistical significance was set as p-value<0.05. Age trends in GD prevalence by survey year (2017–2021) and sex were calculated independently (figure 1A,B). Differential time trends in GD diagnosis between sex and age at GD diagnosis were tested by two-way interactions of sex and age at GD diagnosis in binary logistic regression for the whole population. Logistic regression analysis was conducted using STATA 17 (College Station, TX).

{kind=link}
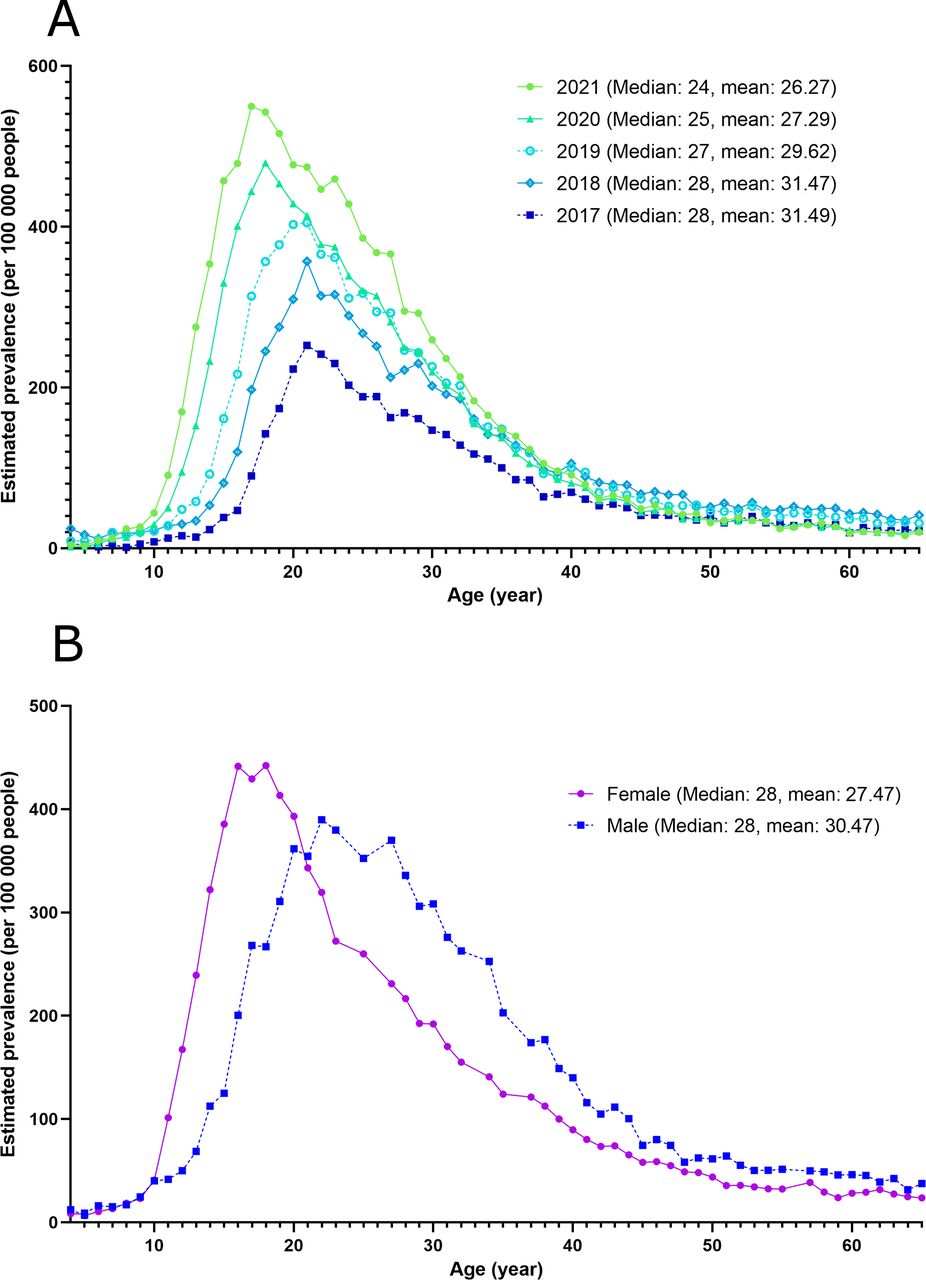
(A) Estimated prevalence, mean age and median age of gender dysphoria by survey year. (B) Estimated prevalence, mean age and median age of gender dysphoria by sex assigned at birth.
Results
Of the approximately 42 million patients identified as the study population, 66 078 were identified with GD (overall estimated prevalence 0.001 5). The mean age of patients with GD was 26; the mean age of the study population was 34. Patients with GD were more likely to be AFAB (57.6% vs 54.6%, p<0.001), non-Hispanic or Latino (71.2% vs 54.2%, p<0.001) and white (72.8% vs 57.6%, p<0.001). The baseline characteristics of subjects are presented in table 1.
Baseline characteristics: demographic data of patients with gender dysphoria and study population.
The estimated prevalence of GD diagnosis increased significantly from 2017 to 2021 (figure 1A). The mean (standard error (SE)) age at GD diagnosis decreased from 31.49 (0.105) in 2017 to 26.27 (0.063) in 2021 (p<0.001). Stratifying the population by assigned sex at birth, the highest prevalence of GD diagnosis among AFABs was at age 19 whereas for AMABs was at age 23 (figure 1B). The mean age at GD diagnosis across all survey years was 27.47 (0.046) in AFABs and 30.47 (0.055) in AMABs (p<0.001). The logistic regression analysis resulted in a significant interaction between assigned sex at birth and age at diagnosis, indicating that the association between age at diagnosis and GD diagnosis varied by the sex assigned at birth. The increasing trend of GD diagnosis among AFABs was significantly more rapid than that in AMABs before the age of 22 (odds ratio (OR): 1.61; 95% confidence interval (CI): 1.58 to 1.65; p<0.001). After the age of 22, the number of AMABs with GD diagnosis exceeded their AFAB counterparts (OR: 1.50; 95% CI: 1.48 to 1.52; p<0.001).
Discussion
Our study estimated a GD prevalence of 155 per 100 000 individuals. Multiple studies describe the reversed ratio in sex assigned at birth.3 Our study showed an increasing trend in AMAB:AFAB of 5:6 in 2017 to 5:7 in 2021, while the pooled ratio during 2017–2021 was 10:13. Most of the change was due to the skew in the number of AFAB adolescents and young adults. This finding is consistent with a recent nationwide Swedish study.9 We found that the estimated prevalence of GD in AFABs sharply increased at the age of 11, peaked at 17–19, and then decreased below AMABs at 22. The estimated prevalence of GD in AMABs started to increase at the age of 13, peaked at 23, and then gradually decreased.
The time of physical and hormonal change during puberty might explain the different patterns of GD development by sex. Youth with GD tend to seek medical attention when puberty begins. AFABs enter puberty at a mean age of 10–11 and, on average, achieve growth and menarche at 13; AMABs enter puberty about 18 months later than AFABs with a slower growth spurt.2 10 The time of puberty onset is consistent with the time when GD patient numbers start to increase. The quick decline after age 18 in the AFAB population diagnosed with GD might result from a decrease in seeking medical intervention. AFABs who start hormones as adults are associated with increased discontinuation rates.11 Thereby, adult AFABs with GD might drop out of our study because of treatment discontinuation.
The reversed gender ratio could be explained by environmental factors. Social movements and media encourage AFABs to embrace diversity and independence. Minority AFABs are more likely to want to express their identities. In contrast, AMABs have been less motivated to express their gender diversity, which may lead to delayed care for AMABs with GD. In addition, social attitudes at an early age are more favourable for girls with GD to reveal their identity. School-age gender non-congruent AFABs are more likely to be accepted by peers, even categorised as the leader of their class.12 By comparison, gender non-congruent AMABs are more likely to face bullying and rejection, which suggests effeminate characteristics are less tolerable in AMABs than masculine characteristics in their GD AFAB counterparts.12 13
A previous study hypothesised that the increasing GD in AFAB adolescents was a consequence of peer influence and mental vulnerability.7 Subsequently, the persistence of GD diagnosis was questioned along with the concern of later regret. Persistent rates of GD were known to be 2%–30% in AMABs and 12%–50% in AFABs.6 However, GD diagnosis in patients receiving gender-affirming intervention did not change significantly over time.14 Our study only showed the pattern of prevalence in different sex and age groups. Further investigation is warranted to determine the persistence of GD diagnosis. Notably, changing identity over time should not be pathologised considering the gender-fluid nature in certain populations.15 That is to say, GD is not a permanent diagnosis.
Increased availability of speciality gender clinics might generally explain the increasing number of patients with GD.16 The decreasing mean age of GD diagnosis suggests an increasing gender non-congruent youth population. The phenomenon might be related to increased accessibility of gender care as well as a gender-minority-friendly social context. Gender identity development heavily leans on social processes, including exploration and experimentation with external feedback.17 There is now increasing acceptance of gender-neutral pronouns and gender-non-congruent chosen names. Gender minority youth are no longer receiving consistent toxic feedback regarding their identity. Additionally, digital platforms such as video games provide a ‘transitional playground’ that allows youth to explore their identity with more freedom and less worry compared with traditional social situations.18 The concept of gender is a cultural construct rather than a genetic fact. The decreased mean age of GD suggests less oppression of gender minority youth and increased awareness of gender diversity. A survey-based study reported 600/100 000 youths under the age of 21 identified themselves as transgender.19 This number is much higher than the estimated prevalence we observed. Previous research and our results demonstrate the need for expanded and accessible gender clinic services.
Limitations
In our study, we assumed gender dysphoria in the Diagnostic and Statistical Manual (DSM) to be equivalent to gender identity disorder as classified in the ICD system, which might be confusing. Gender identity disorder is the old term for gender dysphoria in the DSM-IV, with minor differences in diagnostic criteria.1 We considered the two diagnoses to be the same because only the DSM-5 and DSM-5-TR were available during our study period while there was no change in the ICD system. We applied ICD code F64 (gender identity disorder), which includes the controversial diagnosis of dual-role transvestism (F64.1) and other gender identity disorders (F64.8) which may not meet the full criteria for GD. However, even by applying a broader code with the hope to cover all potential patients with GD, we still could not estimate the GD prevalence since clinical-based studies usually include limited portions of gender non-congruent individuals.20 GD prevalence is highly variable geographically.18 Lacking precise geographic data is another limitation of this study. Despite the fact that 80% of TriNetX data are from the USA, the other 20% are scattered internationally among many countries. We were also not able to analyse the study subjects by race or ethnicity. An additional limitation is the possible sex assigned at birth misclassification in the TriNetX database. It was unclear if patients’ gender in the electronic healthcare records (EMR) represented their sex assigned at birth or their identified gender. Since sex assigned at birth carries a higher weight biologically when it comes to medical decisions, we believe most EMR systems still register patients with their sex assigned at birth. Thereby the effect of misclassification is minimal. Due to the limitations listed above, we only emphasise the temporary change as a trend in sex assigned at birth and age.
Conclusion
Our study demonstrated a climbing prevalence of GD, especially in AFABs. While further studies are warranted to determine the persistence of the diagnosis, we encourage youth to explore their gender identity with a non-biased stance, educate the public on gender diversity, and call upon clinicians to provide timely assessment for children and youth with GD concerns.
Data availability statement
Research data supporting this publication are available from the TriNetX Research Network located at https://trinetx.com/
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but is exempted by the IRB board at Carilion Clinic.
Acknowledgments
We thank Dr Robert L. Trestman for his full support in academic work as the chair of the Department of Psychiatry and Behavioral Medicine at Carilion Clinic and Virginia Tech Carilion School of Medicine. We also thank Carilion Health Analytics Research Team for introducing the TriNetX database, providing consultation services and sharing their experience and knowledge.
References
Ching-Fang Sun is a psychiatry resident physician at Virginia-Tech Carilion School of Medicine (VTCSOM), USA (2021-2024). She is an active member of the American Psychiatric Association and the American Psychoanalytic Student/Resident Associates. Dr. Sun's research interests include child and adolescent psychiatry, mood disorders, LGBTQ issues, psychotherapy, and public health. With expertise in big data analysis and epidemiology, she leads multiple public health projects with the aim of promoting health equality and reducing health disparities.

Supplementary materials
Press release
- Press_release -
Press release
- Press_release -
Footnotes
Twitter @ChingFangSun
Contributors C-FS designed the study and collected the data. C-FS and VM conceived and wrote the manuscript. HX and MSH analysed the data and supported the methodology writing. JHD, YL and ASK provided proofreading and revision for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.