Article Text

Abstract
Background One potential modifiable factor to improve the mental health of healthcare professionals (HCPs) during the pandemic is lifestyle.
Aims This study aimed to assess whether an improved lifestyle during the pandemic is associated with improved mental health symptoms and mental well-being in HCPs over time.
Methods This was a cohort study involving an online survey distributed at two separate time points during the pandemic (baseline (July–September 2020) and follow-up (December 2020–March 2021)) to HCPs working in primary or secondary care in the UK. Both surveys assessed for major depressive disorder (MDD) (Patient Health Questionnaire-9 (PHQ-9)), generalised anxiety disorder (GAD) (Generalised Anxiety Disorder-7 (GAD-7)), mental well-being (Short Warwick-Edinburgh Mental Well-being Score (SWEMWBS)) and self-reported lifestyle change (compared with the start of the pandemic) on multiple domains. Cumulative scores were calculated to estimate overall lifestyle change compared with that before the pandemic (at both baseline and follow-up). At each time point, separate logistic regression models were constructed to relate the lifestyle change score with the presence of MDD, GAD and low mental well-being. Linear regression models were also developed relating the change in lifestyle scores from baseline to follow-up to changes in PHQ-9, GAD-7 and SWEMWBS scores.
Results 613 HCPs completed both baseline assessment and follow-up assessment. Consistent significant cross-sectional associations between increased lifestyle change scores and a reduced risk of MDD, GAD and low mental well-being were observed at both baseline and follow-up. Over the study period, a whole unit increase in the change in novel scores (ie, improved overall lifestyle) over 4 months was inversely associated with changes in PHQ-9 (adjusted coefficient: −0.51, 95% confidence interval (CI): −0.73 to −0.30, p<0.001) and GAD-7 scores (adjusted coefficient: −0.32, 95% CI: −0.53 to −0.10, p=0.004) and positively associated with the change in SWEMWBS scores (adjusted coefficient: 0.37, 95% CI: 0.18 to 0.55, p<0.001).
Conclusions Improved lifestyle over time is associated with improved mental health and mental well-being in HCPs during the pandemic. Improving lifestyle could be a recommended intervention for HCPs to help mitigate the mental health impact during the current and future pandemics.
Trial registration number NCT04433260.
- COVID-19
- Mental Health
- Cohort Studies
- Longitudinal Studies
- Life Style
Data availability statement
Data are available upon reasonable request. Anonymised data, the data dictionary and survey materials are available from the corresponding author, AG, on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Promoting a healthy lifestyle amongst healthcare professionals (HCPs) was employed by a few but not all organisations to improve the mental and physical well-being of HCPs during the coronavirus disease 2019 (COVID-19) pandemic.
However, robust data are limited, regarding whether improvement in the lifestyle is indeed a protective strategy to mitigate adverse mental health impacts of the pandemic among HCPs.
WHAT THIS STUDY ADDS
We demonstrated that an improved overall lifestyle was associated with improved symptoms of depression, anxiety and mental well-being over a 4-month period in a cohort of HCPs during the COVID-19 pandemic.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Improved lifestyle (e.g. regular physical activity, regular healthy meals, reduced cigarette smoking and vaping, and reduced alcohol consumption) could be a viable intervention to mitigate the mental health impact of the current and future pandemics in HCPs.
Introduction
Healthcare professionals (HCPs) may be particularly vulnerable to the mental health impact of the coronavirus disease 2019 (COVID-19) pandemic.1 While the association is likely to be bidirectional, one potential modifiable factor to improve mental health in HCPs is the improved lifestyle,2–6 including physical activity, diet, smoking and alcohol intake.7 Due to the potential for developing chronic physical diseases and mental health issues, which could lead to work absences and reduced quality of patient care, there is an urgent need to understand the lifestyle impact of the pandemic and its association with mental health in HCPs.
The lifestyle impact of the pandemic on the general population is evident, particularly regarding lockdown measures.8–16 Recent research has also found that essential workers, primarily consisting of HCPs, had worsened lifestyle compared with non-essential workers during the pandemic,17 and worse lifestyle has been associated with worse mental health in HCPs and essential workers in several cross-sectional studies.3 5 6 18 19 Despite this, one study observed no association between problem drinking and mental health status in UK intensive care HCPs.20 Longitudinal studies assessing change in mental health associated with lifestyle over time in HCPs are lacking. As such, the possible value of lifestyle as a modifiable factor to improve mental health in HCPs remains unclear, since cross-sectional studies provide ‘snapshot’ associations. Moreover, any consistencies between studies could be due to assessing specific domains of lifestyle (e.g. problem drinking20), in contrast to overall lifestyle.
The COVID-19 Disease and Physical and Emotional Well-being of Health Care Professionals (CoPE-HCP) project aimed to examine how the pandemic impacts specific lifestyle domains in HCPs and to examine the association between overall lifestyle changes and mental health in HCPs at two points during the pandemic. Importantly, this study aimed to examine whether an improved lifestyle over a period during the pandemic is associated with improved mental health and well-being in HCPs. We hypothesised that there would be worsened lifestyles in HCPs as compared with the beginning of the pandemic and that these would be associated with adverse mental health status in HCPs at baseline and follow-up. Lastly, we hypothesised that an improved lifestyle would be associated with improved mental health symptoms and well-being over the same period. If proven, these findings will inform further strategies for the well-being of employees and the public in pandemics and other similar settings.
Methods
CoPE-HCP is a cohort study of HCPs (in the UK and internationally) and non-HCPs (academic and research staff of Queen Mary University of London and other universities in the UK who were not working directly or indirectly with patients confirmed or suspected of having COVID-19). Details of the study are noted elsewhere.21 Corresponding details are registered in ClinicalTrials.gov (NCT04433260).
Briefly, those who were included in the study were aged 18 or older and identified as HCP or non-healthcare academic staff or self-declared non-HCPs. This longitudinal study involved multiple online surveys. The baseline survey was conducted between July and September 2020. In the UK, this corresponded to the trough of the first wave of COVID-19. The baseline survey gathered information including age, gender, ethnicity, relationship status, educational attainment and current mental health and physical health diagnosis (a multiple-choice close-ended item). The baseline survey also assessed the perceived change (since the start of the pandemic) in lifestyle domains: physical activity, cigarette smoking, alcohol consumption, vaping and healthy eating (multiple-choice close-ended items), and included validated mental health screening tools assessing the presence of major depressive disorder (MDD) (Patient Health Questionnaire-9 (PHQ-9)), generalised anxiety disorder (GAD) (Generalised Anxiety Disorder-7 (GAD-7)) and well-being (Short Warwick-Edinburgh Mental Well-being Score (SWEMWBS)).
A follow-up survey was distributed approximately 4 months after baseline containing the same mental health screening tools and items assessing change in lifestyle (compared with the start of the pandemic).
For the purpose of these analyses, we included only HCPs from the UK who responded to both surveys. This would allow evaluation regarding whether an improved lifestyle over time during the pandemic is associated with improved mental health and well-being in HCPs.
Patient and public involvement
A multidisciplinary team of HCPs (including mental health experts, behavioural change experts and those involved with well-being support) was consulted, and feedback was sought on the survey design. The input was also received from the Barts Education Academy on the design and delivery of the surveys.
Statistical analysis
Statistical analysis was performed using Stata V.17.0. At each time point, we calculated the prevalence of the mental health and well-being parameters using the validated cut-off and the proportions showing improvement in the different aspects of lifestyle (physical activity, cigarette smoking, alcohol consumption, vaping and healthy eating).
To estimate the overall change in lifestyle separately at baseline and follow-up, we developed a novel score that considered each behaviour and estimated the score based on the following: a positive score was given for a healthier lifestyle change and a negative score was given for a worsening of lifestyle. For example, physical activity was coded as +1.0, –1.0 and 0, corresponding to increased activity, decreased activity and no change, since the beginning of the pandemic. Similarly, a scoring of −1.0, +1.0 and 0 was assigned for increased, decreased and no change, respectively, for cigarette smoking, alcohol consumption and vaping. Participants who reported never smoking/drinking/vaping were given a score of zero to indicate no change. Healthy eating was assigned 0 for never being a healthy eater and no change, +1.0 for being able to eat healthy meals, −0.5 for trying to but not always managing to eat a healthy diet and −1.0 for not managing to eat a healthy diet. ‘Prefer not to say’ was classed as missing.
Scores were aggregated to produce separate lifestyle change scores at baseline and follow-up. A score was also calculated to assess lifestyle change from baseline to follow-up by subtracting the baseline score from the follow-up score.
Validated cut-offs were used for the mental health assessments. A score of 10 or higher on the GAD-7 and PHQ-9 indicates the presence of GAD and MDD, respectively.22 23 A score of 18 or below on the SWEMWBS indicates low mental well-being.24
Separate logistic regression models were conducted to relate the novel lifestyle score to the presence of MDD, GAD and low mental well-being at baseline and follow-up. Each model was adjusted for age, gender, education, relationship status, number of people living in the household, and currently diagnosed mental health and physical health condition.
Finally, separate linear regression models were then conducted to examine whether improved lifestyle scores (from baseline to follow-up) are associated with improved scores on the respective mental health measures (PHQ-9, GAD-7 and SWEMWBS). These models were adjusted for age, gender identity, education, relationship status, number of people living in the household, as well as current mental health and physical health conditions. The models were then adjusted for the aforementioned variables and baseline PHQ-9, GAD-7 or SWEMWBS score.
To help interpret the regression outputs, further plots were developed based on separate linear regression models where tertiles of lifestyle score were calculated to predict the change in PHQ-9, GAD-7 and SWEMWBS scores. These separate plots were adjusted for baseline PHQ-9, GAD-7 and SWEMWBS, respectively.
Results
Demographic characteristics for cohort of HCPs (N=613)
A total of 613 HCPs with both baseline and follow-up data were included in the analysis (see figure 1 for flowchart). Online supplemental table 1 shows the baseline demographic characteristics of the sample. The median age group was 36–50 years. Most participants were of white ethnicity (80.9%) and self-identified as female gender (76.7%). Most HCPs were also married or living with a partner in the family (65.6%), and most lived with at least one other person in their household (84.7%). Lastly, the majority of HCPs had high educational attainment (86.8% had a bachelor’s degree, master’s degree or doctor of philosophy degree).
Supplemental material
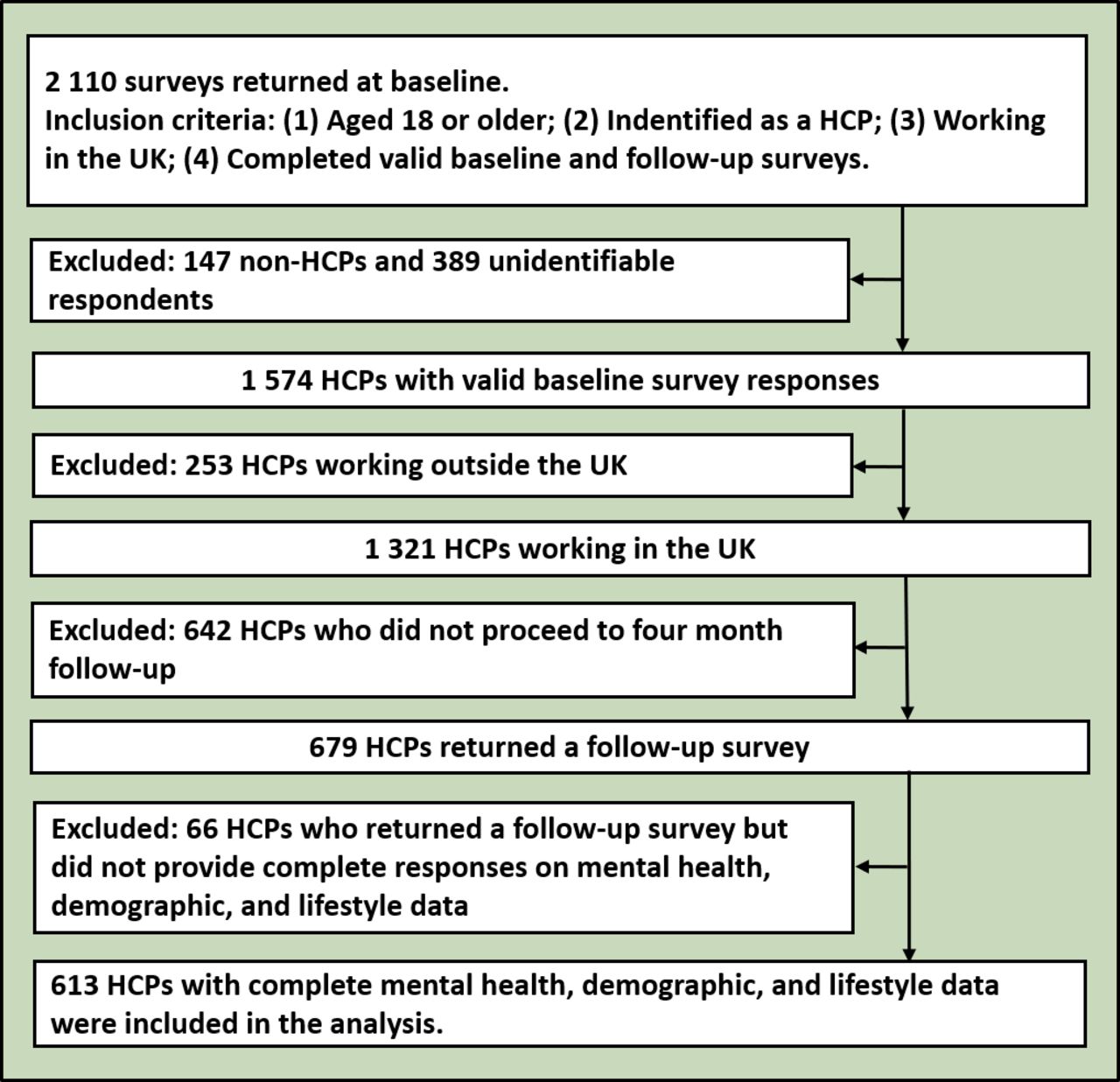
Flowchart for the final sample. HCP, healthcare professional; UK, United Kingdom.
Lifestyle change and prevalence of mental health outcomes in HCPs
At baseline, UK HCPs generally reported worsened health-risk behaviours compared with before the pandemic (table 1). A higher proportion became physically less active since the beginning of the pandemic (43.2% reported decreased activity vs 22.3% reported increased activity vs 32.6% reported no change), while the majority reported the same levels of alcohol consumption (35.4%). Most participants were never smokers (72.6%) and never vapers (94.9%). Out of those who consumed alcohol, relatively higher proportions reported consuming more (29.9%) rather than less (18.3%). In smokers and vapers, relatively more participants reported smoking more (4.9% smoking more vs 1.6% smoking less) and vaping more (1.5% vaping more vs 0.5% vaping less). At baseline, 23.2% of UK HCPs reported trying but not always managing to eat a healthy diet.
Change in health-risk behaviours (compared with before the pandemic), and prevalence of mental health outcomes at baseline and follow-up in UK HCPs (N=613)
At follow-up assessment (approximately 4 months later), a relatively larger proportion compared with baseline reported being physically less active (55.6% at follow-up vs 43.2% at baseline) as compared with the beginning of the pandemic. A larger proportion at follow-up (25.4% at follow-up vs 18.3% at baseline) reported drinking less compared with the beginning of the pandemic, and there was relatively little change in smoking or vaping status. The percentage of UK HCPs trying but not always managing to eat a healthy diet increased at follow-up (28.4% at follow-up vs 23.2% at baseline).
The mean total lifestyle scores in the 613 UK HCPs were −0.11 (range=−4 to 3) at baseline and −0.20 (range=−4 to 3) at follow-up (see online supplemental table 2), indicating that, at both baseline and follow-up, the overall lifestyle of UK HCPs worsened as compared with the beginning of the pandemic. The decreased mean score at follow-up indicated that lifestyle worsened over the 4-month period. Regarding mental health, the prevalences of all outcomes increased from baseline to follow-up (table 1).
Cross-sectional logistic regression models relating the novel lifestyle score to the presence of mental health and well-being at baseline and follow-up in UK HCPs
There were consistent associations between the novel lifestyle score and the presence of MDD, GAD and low mental well-being (SWEMWBS) (table 2).
A whole unit increase in total lifestyle score was associated with a 40% reduction in the risk of MDD at baseline (adjusted (adj.) OR: 0.60, 95% CI: 0.51 to 0.70, p<0.001) and a 24% reduction at follow-up (adj. OR: 0.76, 95% CI: 0.66 to 0.87, p<0.001), a 26% reduction in the risk of GAD at baseline (adj. OR: 0.74, 95% CI: 0.62 to 0.87, p<0.001) and a 17% reduction at follow-up (adj. OR: 0.83, 95% CI: 0.71 to 0.97, p=0.017), and a 36% reduction in the risk of low mental well-being at baseline (adj. OR: 0.64, 95% CI: 0.53 to 0.77, p<0.001) and a 31% reduction at follow-up (adj. OR: 0.69, 95% CI: 0.58 to 0.83, p<0.001) (table 2).
Separate cross-sectional logistic regression models relating the novel lifestyle score to mental health outcomes in UK HCPs at baseline and follow-up
Linear regression predicting the change in mental health scores with the change in lifestyle score from baseline to follow-up in UK HCPs
Separate linear regression models showed that a whole unit increase in lifestyle change was inversely associated with the change in PHQ-9 (adj. coefficient: −0.51, 95% CI: -0.73 to −0.30, p<0.001) and GAD-7 scores (adj. coefficient: −0.32, 95% CI: −0.53 to −0.10, p=0.004), and associated with increased SWEMWBS scores (adj. coefficient: 0.37, 95% CI: 0.18 to 0.55, p<0.001) over the 4-month period (table 3). Collectively, this demonstrated that improved lifestyle over time is associated with improved mental health symptoms and well-being during the same period.
Linear regression predicting the change in mental health scores with change in lifestyle from baseline to follow-up in UK HCPs (N=613)
When categorised into tertiles of lifestyle change score, significant trends were observed between tertile and change in PHQ-9, GAD-7 and SWEMWBS scores (figure 2) (adjusted for baseline PHQ-9, GAD-7 and SWEMWBS scores, respectively; for unadjusted plots, see online supplemental figure 1).
From baseline to follow-up, for PHQ-9, there was a significant reduction in the change of PHQ-9 scores in those in the highest tertile of lifestyle change (adj. coefficient: −1.69, 95% CI: −2.47 to −0.92, p<0.001) but not in the middle tertile, compared with participants in the lowest tertile. For GAD-7, there was a significant reduction in the change of GAD-7 scores in those in both the middle (adj. coefficient: −0.76, 95% CI: −1.52 to −0.00, p=0.049) and highest (adj. coefficient: −1.00, 95% CI: −1.76 to −0.24, p=0.010) tertile, compared with participants in the lowest tertile. For SWEMWBS, there was a significant increase in the change of SWEMWBS scores in those in the highest tertile (adj. coefficient: 0.89, 95% CI: 0.36 to 1.41, p=0.001) but not in the middle tertile, compared with participants in the lowest tertile.
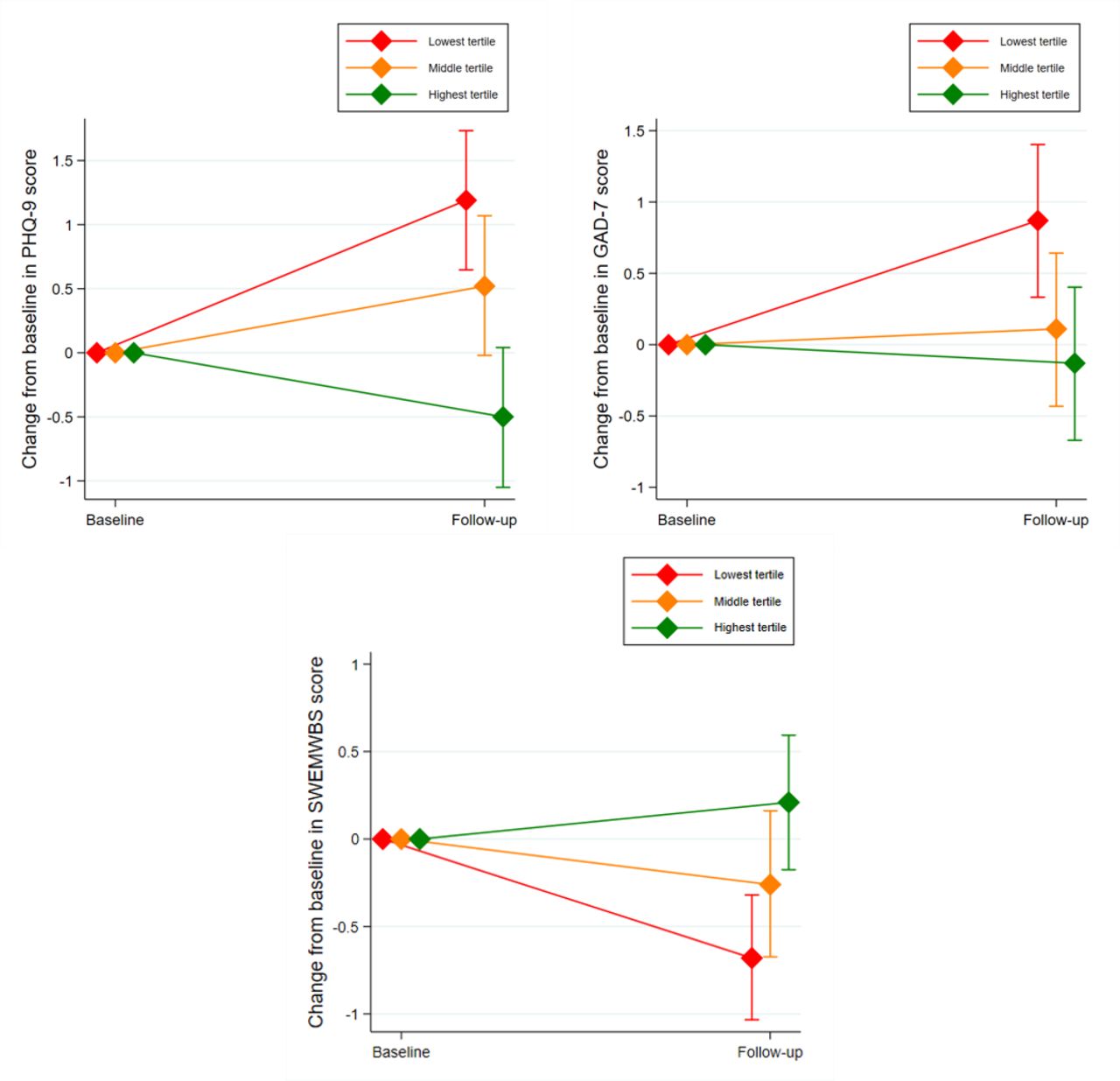
Plots illustrating the change in mean PHQ-9, GAD-7 and SWEMWBS scores from baseline to follow-up, by tertiles of lifestyle score change. Note: the lowest tertile includes lifestyle score changes lower than −0.5; the middle tertile includes scores from −0.5 to 0; and the highest tertile includes scores greater than 0. GAD-7, Generalised Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9; SWEMWBS, Short Warwick-Edinburgh Mental Well-being Score.
Discussion
Main findings
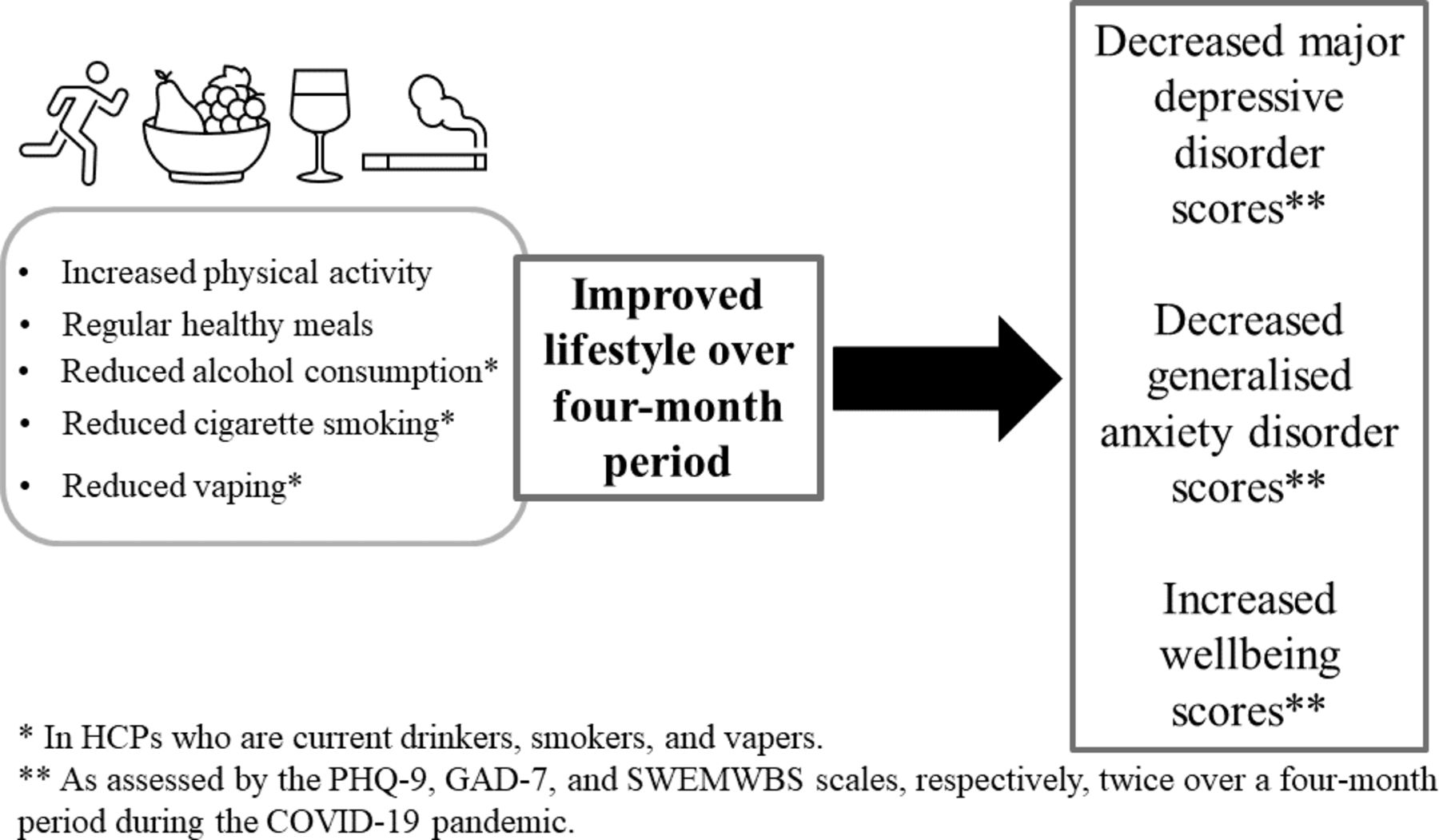
This cohort study indicated that the overall lifestyle in HCPs, consisting of changes to physical activity, cigarette smoking, alcohol consumption, vaping and healthy eating, had deteriorated compared with the beginning of the pandemic and worsened at follow-up. It is also concerning to note that the prevalence of mental health outcomes increased during this period. The study showed reliable associations between improved lifestyle and reduced risk of mental health issues in UK HCPs during the COVID-19 pandemic: a whole unit increase in lifestyle change was significantly associated with reductions in the odds of having depression, anxiety and low well-being at baseline and follow-up. More importantly, and to our knowledge for the first time, we demonstrated that improved lifestyle over the 4-month period is significantly associated with improved symptoms of validated depression, anxiety and well-being measures in HCPs during the COVID-19 pandemic (figure 3), regardless of their respective baseline mental health score. This is valuable evidence showing that lifestyle, as a modifiable factor, can improve mental health in UK HCPs and could be a recommended intervention, in addition to dedicated psychological support, during the current and future pandemics.

{kind=link}
{kind=link}
{kind=link}
Key study findings showing that improvements on the novel global lifestyle score over a 4-month period in HCPs is associated with improved depression, anxiety, and mental well-being scores over the same 4-month period. GAD-7, Generalised Anxiety Disorder-7; HCP, healthcare professional; PHQ-9, Patient Health Questionnaire-9; SWEMWBS, Short Warwick-Edinburgh Mental Well-being Score.
Our findings are consistent with previous work in the general population (and more so in HCPs) during the pandemic.17 In UK health and social care workers, substance use was found to increase and exercise was found to decrease approximately 6 months after baseline assessment during the pandemic.19 McFadden and colleagues also found that well-being was consistently associated with substance use and exercise at both time points. Elsewhere, Vietnamese HCPs whose smoking and alcohol consumption was unchanged or increased had significantly increased risk of having depression or anxiety, compared with HCPs whose smoking and alcohol consumption stopped, decreased or never consumed.5 Similar observations were made for physical activity and a healthy diet but in the reverse direction.5 Our study extends this work considerably by demonstrating associations between improved lifestyle and improved mental health and well-being scores over time.
There are several strengths to this study. First, we examined the associations between lifestyle and various domains of mental health, namely, depression, anxiety and a global indicator of well-being. The value of this is that we can differentiate the relevance of improved lifestyle to specific domains of mental health. Second, the inclusion of a relatively large sample size obtained at two separate points during the pandemic provides reliability in the observed associations. Finally, we obtained changes in mental health over a 4-month period, as opposed to snapshot associations.
Limitations
Despite these strengths, there are some limitations that must be acknowledged. First, most participants were white and female; therefore, our findings could be less applicable to those identifying as male and of other ethnicities. Second, we treated 'prefer not to say' lifestyle responses as missing, but this may underestimate the potential change in behaviours not disclosed by HCPs due to their occupation. Nevertheless, the number of responses for 'prefer not to say' are minimal relative to the sample size. Third, since we used a global score, the extent that improved mental health scores can be attributed to specific behaviours is uncertain and, unlike validated lifestyle measures such as the SMILE-C (The Short Multidimensional Inventory Lifestyle Evaluation during Confinement),25 we have not accounted for lifestyle domains such as sleep pattern and social support. We expect that either physical activity or alcohol consumption is driving the associations because these behaviours showed a greater number of participants reporting change compared with before the pandemic. Finally, since our lifestyle measures are self-reported, the perceptions of lifestyle change could be influenced by the adverse mental health brought on by the pandemic or otherwise.
Implications
By demonstrating robust evidence for the association between improved lifestyle and improved depression, anxiety and well-being symptoms over time, we can set the groundwork for a lifestyle-based intervention to help mitigate the mental health impact of the pandemic in HCPs.
It would be beneficial to understand the impact of specific lifestyle changes on different domains of mental health in HCPs stratified by their current lifestyle. For example, while increased physical activity (or sustained physical activity in those who are physically active) is likely to improve (or maintain) mental health in HCPs, there will be other lifestyle aspects relevant only to those individuals engaging in that specific lifestyle (e.g. an intervention focusing on reducing alcohol consumption may only be relevant to those who are heavy drinkers). Drawing on this, there are underlying groups that require further study. In this analysis, those who never drank alcohol and those who consume the same as before are categorised as ‘no change’. Moreover, we expect that those who drink less than before the pandemic could represent those who continue to be heavy drinkers.
It is also unclear what the relevance of different aspects of lifestyle change is to different domains of mental health. It would be valuable to understand whether improving diet, for example, is as effective as physical activity in mitigating anxiety, or whether improved diet is more relevant to domains such as depression. Future research implementing randomised controlled trials are required to test the efficacy of specified and tailored lifestyle-based interventions to different subgroups of HCPs. A randomised controlled trial will also determine the extent of a bidirectional relationship between lifestyle change and mental health. We hope future researchers can draw on this study to improve the design of future studies evaluating the extent that improvements to lifestyle mitigate adverse mental health in pandemic settings.
Separately, a potential link between pandemic-influenced lifestyle changes and physical health conditions may exist within HCPs, in addition to the potential impact of chronic psychological stress on physical health. This has been recently hypothesised within the general population regarding lockdown measures.26 Since the lifestyle and mental health of UK HCPs appears to have worsened during this 4-month period of the pandemic, further research is needed to examine the longer-term impact on physical health.
Conclusion
The general lifestyle of UK HCPs had deteriorated due to the pandemic (and worsened over a 4-months follow-up), and it is associated with an increased risk of depression, anxiety and low well-being. Conversely, an improved lifestyle over this period was associated with reduced symptoms of depression and anxiety and improved well-being. These findings provide support for helping HCPs in prioritising lifestyle improvements as an intervention to help mitigate the mental health impact of the COVID-19 pandemic in HCPs.
Data availability statement
Data are available upon reasonable request. Anonymised data, the data dictionary and survey materials are available from the corresponding author, AG, on request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Cambridge East, Research Ethics Committee (20/EE/0166). The participants gave informed consent to participate in the study before taking part.
Acknowledgments
We acknowledge the extensive support received from the Barts Education Academy and William Harvey Research Institute for sharing some of their resources needed to conduct this study. In particular, we acknowledge the excellent contribution of the following: Julekha Khanam from Barts Health NHS Trust, Elaine Colaco and Martyn Clark from Barts Education Academy, Christina Komodromos from Barnet, Enfield and Haringey Mental Health NHS Trust, Tania Toma from Imperial College Healthcare NHS Trust, and Ade Alele, Professor Sir Mark Caulfield and Professor Amrita Ahluwalia from William Harvey Research Institute.
References
Dr Mohammed Y. Khanji attended the National University of Ireland, Galway and graduated in 2004 with a MBBCh. He then graduated with a PhD from Queen Mary University of London in the UK. He currently works as a consultant cardiologist in the Department of Cardiology at Barts Health NHS Trust. He is co-chair of the East London Cardiovascular Disease Prevention (ELoPE-CVD) Group and Honorary Clinical Reader (Associated Professor) at Queen Mary University of London in the UK. His main research interests include cardiovascular disease prevention, population health, and cardiovascular imaging.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MYK and GC are joint first authors.
Contributors Conceptualisation: AG, JG, CM, VK and SMN. Data curation, formal analysis: GC, TG and AG. Funding acquisition and supervision: AG. Methodology: MYK, CM, SMN, IS, JG, VK and and AG. Project administration: GC and AG. Validation: MYK and AG. Visualisation: GC, AG and TG. Writing (original draft): MYK, GC and AG.Writing (review and editing) and investigation: all authors. AG is a principle investigator and responsible for the overall content as guarantor. The guarantor accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. AG is a Principle investigator and senior author.
Funding This work was supported by a Barts Charity project grant (MGU0586).
Disclaimer The funders had no role in the study design, data collection, data analysis, data interpretation or writing of the report.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.