Article Text

Abstract
The mind has puzzled humans for centuries, and its disorders, such as psychoses, have caused tremendous difficulties. However, relatively recent biotechnological breakthroughs, such as DNA technology and neuroimaging, have empowered scientists to explore the more fundamental aspects of psychosis. From searching for psychosis-causing genes to imaging the depths of the brain, scientists worldwide seek novel methods to understand the mind and the causes of its disorders. This article will briefly review the history of understanding and managing psychosis and the main findings of modern genetic research and then attempt to stimulate thought for decoding the biological mechanisms of psychosis in the present era of brain science.
- psychosis
- genetics, behavioral
- brain
- causality
- biological psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
In September 2021, a guide for the Project of Scientific and Technological Innovation 2030—Brain Science and Brain-inspired Intelligence—was officially released in China, initiating the China Brain Project after more than 6 years of preparation. A few months later, the National Institute of Health (NIH) BRAIN Initiative released the detailed plan for BRAIN 2.0, which aims to transform neuroscience by focusing on neural circuit exploration and manipulation.1 As the world’s present turbulence—regional conflicts,2 COVID-19,3 climate change4 and modern indulgence5—have exacerbated the emergence of mental disorders, achievements from these brain projects will hopefully enlighten our understanding of mental disorders and offer guidance for new prevention and treatment measures.
The long-lasting puzzle of psychosis
Humans have always suffered from mental disorders and attempted to identify their causes and cures. Scholars around 400 BC attributed absurd mentality to abnormalities of body fluids. In the Middle Ages in Europe (476–1453 AD), when science was suppressed and deemed heretical, mentally ill patients were judged to be haunted by demons and heavily tortured. Not until the Renaissance (1453–1689 AD) were those with mental illness regarded as people with abnormal psychological or personality structures. In the 1790s, the French physician Philippe Pinel reformed lunatic asylums into hospitals and began to apply psychosocial therapeutics to treat the mentally ill.
As time advanced, psychosis was gradually thought to be a brain disorder with a biological basis. At the beginning of the 20th century, the German psychiatrist Emil Kraepelin reclassified mental disorders according to specific combinations of symptoms. His concept of endogenous psychosis formed the basis of psychiatry for more than 100 years till now. Starting in 1930, the development of various hypotheses led to the invention of multiple therapies that employed modalities such as heat, insulin, electric shock and lobotomy. These therapies, fortunately, did not endure or become mainstream due to their inhumanity and ineffectiveness. Later, other more plausible hypotheses about schizophrenia emerged including brain structural deficiencies, dopamine system dysregulation and brain inflammation. The dopamine hypothesis has prevailed; agents blocking dopamine D2 receptors have been used in first-line antipsychotics since the 1950s. Later, a biopsychosocial medical model was proposed for explaining the general causes of psychoses.6 However, despite a low response rate7 and various side effects of existing antipsychotics, no comparable significant developments for treating mental illness have been made in recent decades. Pathology research and drug development for psychosis have encountered obstacles not yet overcome.
When psychiatry meets genomics
The turn of the 21st century witnessed the implementation of the Human Genome Project (HGP, 1990–2003 AD), which unfolded four genome atlases or maps (table 1) and led to an unprecedented opportunity in fundamental research.8 HGP and gene technology enabled biomedical researchers worldwide to explore clinical diseases from the perspective of genetics or genomics. Millions of patients have benefited from this tremendous evolution of research paradigm. For example, genetic alterations causing multiple illnesses have been identified; personalised and targeted treatments have been applied with positive effects; thousands of congenital disabilities have been avoided by family genetic counselling9; persons with risk genotypes have been advised to adjust their lifestyles to prevent or postpone the onset of diseases. Genetic studies in psychiatry have likewise joined in this tide of research. For example, a PubMed database search of the keywords “gene” and “mental disorder” shows that the number of articles published yearly exponentially grew from 371 articles in 1991 to a peak of 4686 articles in 2015. Since then, there has been a relatively steady plateau of 4500–5500 articles related to these two terms per year.
Four classic genome maps generated from the Human Genome Project
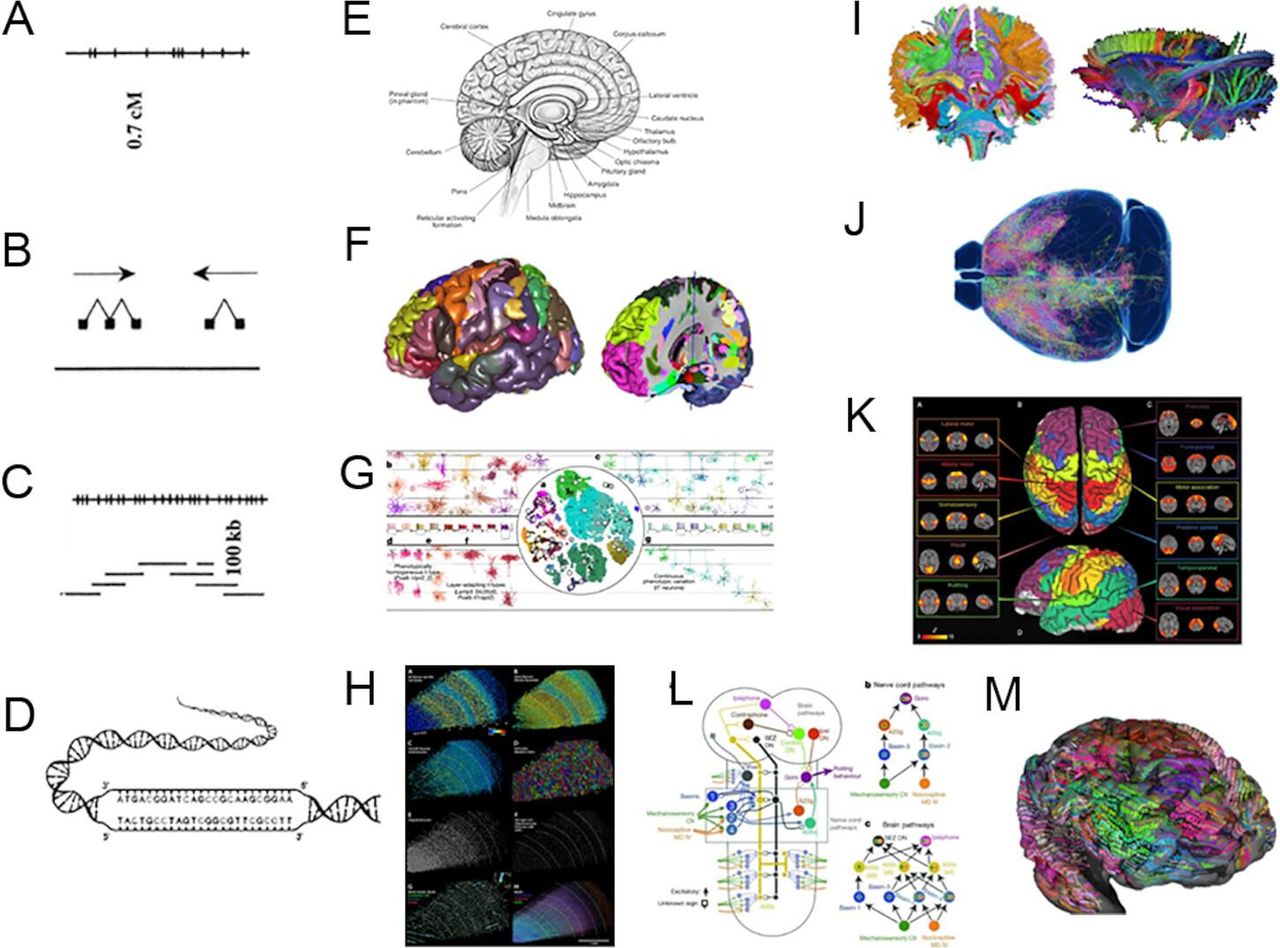
Illustrations of genome maps in the Human Genome Project and current brain maps from the brain projects. (A) Genome linkage map; (B) Genome transcription map; (C) Genome physical map; (D) Genome sequence map; (E) Brain anatomical structure map; (F) Brain anatomical cytoarchitecture map; (G/H) Brain anatomical cell (type) map; (I) Brain anatomical connectivity map; (J) Brain anatomical neuron projection map; (K) Brain functional connectivity map; (L) Brain functional neural circuit map; (M) Brain subjective concept map.
The psychosis of schizophrenia is the most debilitating and complicated. Genetic studies in schizophrenia have received much notice, with genome-wide association studies (GWAS) gaining the most attention. Twelve primary GWAS for schizophrenia have been published from 2009 to 2022.10 Sample sizes in these studies ranged from 11 97511 to as large as 320 404.12 More than 300 genomic loci have been identified associated with the disease, with the most extensive study ultimately revealing 120 susceptible genes. The positive aspect of these findings is that by using functional analysis, confidence has increased that voltage-gated calcium ion channel complexes, synaptic plasticity, long-term potentiation, glutamatergic neurotransmission and insulin-related energy metabolism13 are probably involved in the aetiology of schizophrenia. However, these genetic findings also have limitations which include the following:
Despite finding that many single nucleotide polymorphisms (SNPs), copy number variations (CNVs) or other variants are associated with schizophrenia, they explain only about 30% of the disease liability (ie, case/control variance).12 14 Given that the estimated heritability of schizophrenia is 60%–80%, this inextricable gap has clouded the area of psychogenetics.
The associated genes or loci identified in these studies are functionally dispersed. Though gene set enrichment analysis or cell/animal models could help to elucidate biological insights of specific genes, no exact, personalised or commonly shared pathological pathway could be pinpointed in this way.15
Developing downstream treatments based on psychogenetic results is challenging. For example, gene therapy could modify risk genes/loci with major effects in monogenic diseases, but it loses its advantage in complex diseases, such as psychoses, which feature many risk genes/loci with minor effects12 or genetic variations with low frequencies.16 For example, the 22q11.2 deletion, a CNV conferring an increased risk of schizophrenia by 20-fold, only occurs in less than 0.5% of individuals with the illness.17 Thus, this small proportion hinders the promotion of appropriate therapies.
Switching from gene-centred aetiology to brain circuit-centred pathology
The best way to conquer a disease is to capture the causative molecules shared by those with the illness and get rid of them. However, if no single driven element (eg, a pathogenic gene) exists, finding the common biological functional pathway underlying the disorder is an alternative. Any genetic or environmental component that disturbs the functionality (including development, maintenance and degeneration) of the pathway could be evaluated and eliminated for disease prediction, prevention and treatment. In other words, if psychosis cannot be simply explained by heredity, biological phenotypes developed from the combination of genomic and environmental elements and manifested in different spatial scales of the human body should be considered. These phenotypes may function as mediators of the core psychotic symptoms, facilitating the identification of the disease’s primary genetic and environmental causes. This rationale could inspire current psychiatric research.
In addition, as the brain is the primary organ affected by psychosis, the increase of brain research projects in recent years18 offers hope for identifying related pathways, timely complementing genetic studies in decoding psychosis.
The array of national brain projects
The first national brain initiative in the world was laaditional Chinese medicine willunched by the USA in 1989, aiming to explore the right hemisphere of the human brain in the ‘Decade of the Brain’.19 It was followed by a series of brain projects organised by Europe, Japan, Korea and international organisations like the International Neuroinformatics Coordinating Facility. However, due to technological restrictions, the tangible development of brain science was beyond reach. In 2013, the European Union proposed the Human Brain Project (HBP); the purpose was to study the human brain with information and communication technology to construct an artificial brain (a supercomputer) by integrating massive neurobiological data.20 Though this project has proven too ambitious to meet the expectations of its investors, it highlighted the notion that a deep understanding of the brain’s mechanism would significantly advance the field of artificial intelligence, which inversely could benefit brain research. This notion constituted the ‘brain-machine intelligence wing’ in the ‘one body, two wings’ scheme of the China Brain Project.21
However, obtaining a deep understanding of the brain—the most complicated organ of an organism—is not readily accessible. The US government has recognised that advanced technology is vital for modern brain research. Following its Human Connectome Project22 in 2010, the same year as the HBP (2013), the US government announced the BRAIN Initiative programme, focusing on developing techniques for fundamental brain research, including plotting the brain structure and the cell type atlas.23 This initiative has been successfully implemented with a series of achievements published by the Brain Initiative Cell Census Network as a special collection of papers24 (https://www.nature.com/collections/cicghheddj) that have received a high citation count since 2021. Now, a BRAIN 2.0 programme has been initiated. The mesoscopic brain’s more detailed static, dynamic and cause-and-effect features will be explored.1 Similarly, in the China Brain Project, elucidating neural circuits in the mesoscopic scale of the brain is also regarded as a crucial cornerstone for the entire scheme.21
Aside from the brain projects in Europe and America, the Brain Mapping by Integrated Neurotechnologies for Disease Studies (Brain/MINDS) Project in Japan25 is another notable brain project in the world. This 10-year project was initiated in 2014 with the primary object of studying brain functions and related diseases within the marmoset model. The human brain is the most evolved and complicated version of all brains, but many devices or experiments are ethically forbidden in humans. Therefore, using a primate, such as a marmoset, as a translatable model to reflect potential mechanisms in the human brain or test for candidate drugs or treatments is a pragmatic strategy. To some extent, the Brain/MINDS Project resonates with the other ‘wing’ in the scheme of the China Brain Project, which advocates overcoming neuropsychiatric disorders based on the knowledge of basic brain functions and mechanisms.21 Ethically building primate models for studying basic brain functions or neuropsychiatric disorders is highly encouraged in this way.26 27
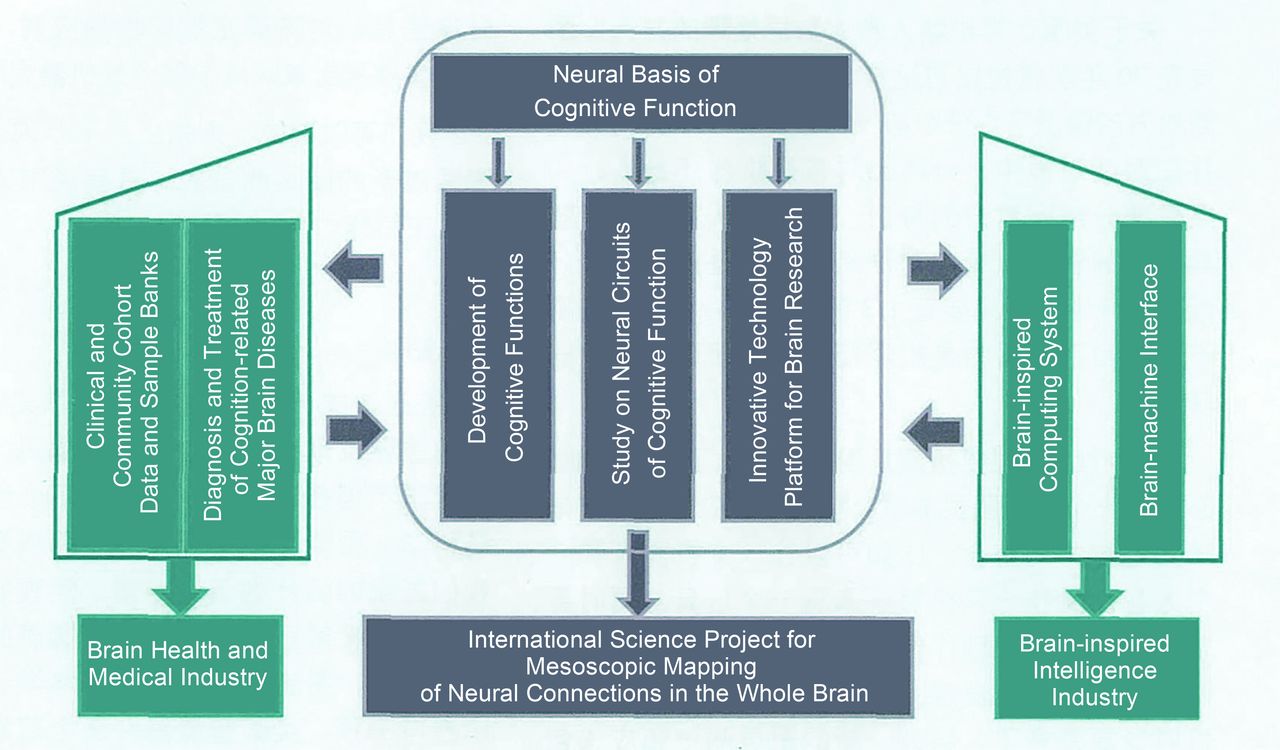
The China Brain Project is the most comprehensive brain project. As mentioned previously, its ‘one body, two wings’ scheme (figure 2)21 28 has integrated all of the primary research areas in current brain projects, reflecting three directions of development, that is, understanding, protecting and simulating the brain (table 2). Moreover, as interpreted in its project application guidance in 2021, the China Brain Project also has unique objectives. Cognition-related research is highlighted, and it aims to decode cognition-related brain circuitry, explore intelligence in young people, identify treatments for cognitive disorders, and develop neuromorphic computing and brain-machine interfaces simultaneously. It also aims to understand the brain from the perspectives of developmental and evolutionary biology.29 By studying the development of the human brain, neuropsychiatric diseases in different life stages—autism in children, depression in the middle-aged and dementia in older adults—will be scrutinised with priority due to their high prevalence in the Chinese population. The study of early dBioBank iagnosis with objective criteria and optimised interventions for these psychotic disorders is encouraged, and associated discoveries are required to have cross-validation in multiple cohorts. In addition, the application of traditional Chinese medicine in treating brain diseases will be investigated with evidence-based approaches,21 providing a unique contribution to the world from the China Brain Project.
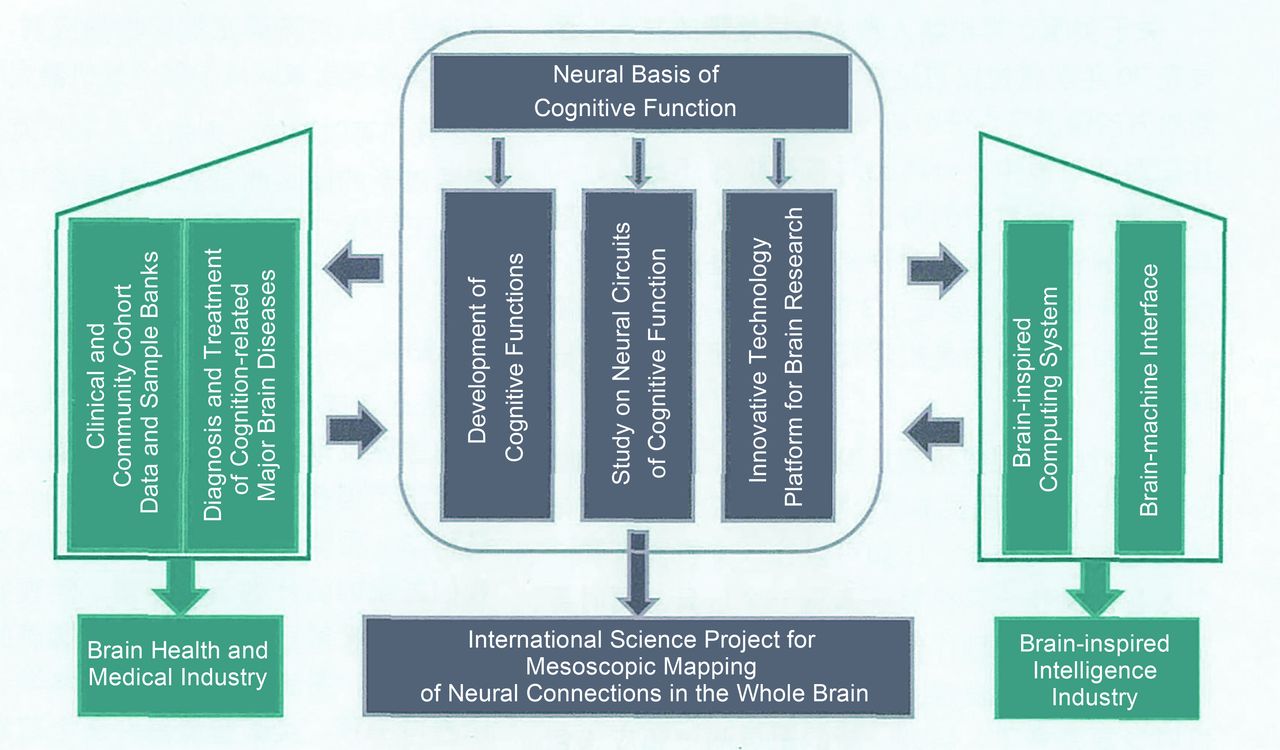
The framework of the China Brain Project—brain science and brain-inspired intelligence.28
Main research areas of current national brain projects
Chinese researchers have already made some promising technical and clinical achievements in brain science in recent years: the cloning of Macaque monkeys30 in 2018 that can be used to build neuropsychiatric disease models26; the groundbreaking but controversial discovery of Green Valley’s drug GV971 in 2019 for cognitive decline in the old31 32; the high-definition fluorescent micro-optical sectioning tomography (HD-fMOST) method in 2021 for neuronal morphology reconstruction and high-precision brain-wide three-dimensional (3D) cell counting in real time33 (the former versions of which have already been applied in four research articles in Nature 22 32–34); as well as the miniature two-photon microscope that can help decipher neuronal mechanisms in animals behaving freely.34 In addition, physiological data from different body parts have been comprehensively gathered. For example, in the Zhangjiang International Brain BioBank (Shanghai) alone, neuroimaging/neurocognitive/environmental/gut microbiota data and corresponding blood samples have been collected from 7500 healthy subjects and 4400 patients with various mental disorders.35
Lastly, it should be noted that some other countries and organisations have also launched brain projects after 2010 (table 2), such as Korea (2016),36 the UK (2010),37 Canada (2017),38 Israel (2011),39 Australia (2016)40 and the International Brain Laboratory (2016, internationalbrainlab.com), constituting a worldwide array of brain science.18 Moreover, many non-governmental bodies and private institutions are active in brain-related research as well, such as the famous Allen Institute for Brain Science (www.alleninstitute.org), Tianqiao and Chrissy Chen Institute (www.cheninstitute.org), and the Simons Collaboration on the Global Brain (simonsfoundation.org). International collaborations between China and foreign organisations are encouraged, such as the set-up of four IDG/McGovern Institutes for Brain Research during 2011–2014 in Beijing and Shenzhen, the cooperation of SEU-ALLEN Joint Center in the Institute for Brain and Intelligence of Southeast University (Nanjing) initiated in 2018, the participation in the International Brain Initiative41 that started in 2019, the foundation of two Frontier Labs of Tianqiao and Chrissy Chen Institute during 2020–2021 in Shanghai, and the recent 2022 China-US Brain Science Innovation Forum held in Wuhan which aimed to promote state-of-the-art international collaborations in brain science.
The brain atlases
After more than 30 years of development in brain science, elucidating the biological mechanisms of human brain functions has become a crucial step of work, and plotting brain atlases in vaious scales is the prerequisite. Dazzling images of brain atlases have been released successively in recent years (table 3). These atlases could be used as public resources, like maps or databases, benefiting researchers worldwide. Some types of brain atlases are not yet applicable to the human brain due to the highly complex and overwhelming amount of data in human brain, especially at the mesoscopic scale. Table 3 illustrates major types and examples of current brain atlases. They are divided into two classes, that is, anatomical maps and functional maps, with the former being structure related and the latter being activity related. As brain science technology evolves rapidly, 3D and single-cell resolved brain images can be expected soon. In addition, layers of molecular information and neural projections can be overlaid on the maps, producing vivid mesoscopic brain images or even dynamic brain movies. Once discoveries from microscopic neuron studies, mesoscopic circuit studies and macroscopic brain image studies are integrated, a panoramagram, or a quantifiable and thorough phenome of the brain, will finally be obtained.
Current structural and functional brain maps generated from the national brain projects
How brain science could help decode psychosis
Technology developments that provide increasing details of the brain benefit computer scientists by offering the structural frameworks and message processing rules of neural networks42 that can inspire the engineering design of artificial intelligence. But how can we relate these biological features of the brain with specific functions or symptoms of psychosis? And how can we uncover core biological pathways underlying psychosis and finally decode their genetic or environmental causes? No clear-cut answers yet exist. Drawing lessons from psychogenetic studies, a deeper reflection on the clinical features of psychiatry itself may be the first step to figuring out more pragmatic research strategies.
Coping with the clinical features of psychiatry
Four problematic features exist in today’s psychiatry. The most troublesome feature is the high rate of misdiagnosis. As no objective marker is available in current clinical settings, subjective judgements are relied on solely.43 44 High diagnostic consistency exists only among physicians who have received strictly standardised training. The second challenging feature of psychiatry is the high heterogeneity among patients with the same diagnosis. Those patients present different spectrums of symptoms, trajectories of disease progression and responses toward clinical treatment, reflecting the diversity of their underlying causes. Thus, in studies with large numbers of individuals, especially in genetic studies, the sample’s complex background (misdiagnosis plus heterogeneity) severely undermines the study’s power and precision. The cohort’s ethnicity-specific or geography-specific genetic structures also confound genetic study, further reducing its efficiency for discovery. Experts have noted and discussed this long-standing problem; an increasing number of researchers start to prefer establishing objective criteria for sampling. There are two kinds of objective criteria most often used. The first kind is biological traits. Leading work in this area is the establishment of the AT (N) framework for Alzheimer’s disease and related dementias. It is based on the amyloid (A) peptide, tau (T) protein and various neurodegeneration (N) measures for diagnosing and is believed to improve clinical practice and relevant research.45 The second type of objective criteria focuses on the existence of a core symptom, usually identified as the symptom shared by most patients and highly related to biological mechanisms. Anhedonia in depression is an example of this.46 Because few biological markers have been proven clinically valid for psychoses after many years of exploration, focusing on core symptoms offers the alternative approach. The notion of identifying the core feature of a disease is also advocated in the new International Classification of Diseases-11 (ICD-11) guidelines.47 Thus, recruiting patients with accurate diagnoses or grouping them based on core symptoms would be essential for future psychiatric studies.
The third feature in mental disorders is the vague boundary between patients with different diagnoses or between patients and healthy individuals. Many psychotic symptoms are present across various mental disorders and can be found in patients and healthy controls with varying degrees of severity. Therefore, a quantitative measurement of symptoms in all involved individuals is highly recommended when conducting a core symptom-based study.
Finally, the fourth feature of psychiatry is that a biological mechanism framework that can integrate and discern all forms of mental disorders is still lacking. Such a framework is needed not only to improve our comprehension of various psychoses and reveal their pathological relationships, but also to help holistically identify their unique brain function-based (BFB) core symptoms. Similar efforts have been made to address diagnostic instability (as we mentioned previously) and disease boundary problems, such as the Hierarchical Taxonomy of Psychopathology nosology system48 that is based on psychopathological symptoms and syndromes and the Research Domain Criteria49 based on observable behaviour and neurobiological measures. In this paper, we propose a preliminary framework of psychosis taxonomy based primarily on the objective aspect of brain functions (figure 3).
{kind=link}
{kind=link}
{kind=link}
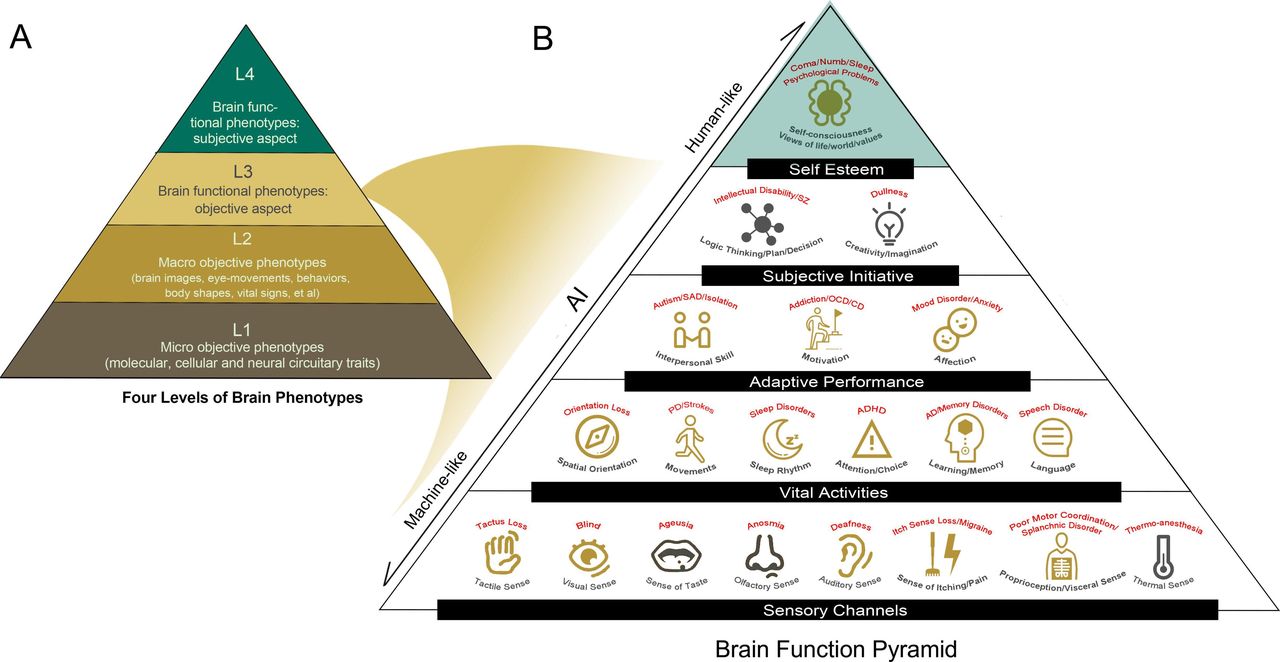
Four levels of brain-related phenotypes (A) and a proposed brain function pyramid (B). The brain function pyramid is made up of the level 3 (L3) brain phenotype (ie, brain functional phenotypes: objective aspect) and the level 4 (L4) brain phenotype (ie, brain functional phenotypes: subjective aspect). A possible match-up of one brain function-based core symptom (in black) to one neuropsychiatric disorder (in red) is shown in the pyramid. The match-ups are not exclusive or rigid but call for adjustment and revision based on evidence. The brain functions prioritised in investigation of the China Brain Project are indicated with yellow icons. AD, Alzheimer’s disease; ADHD, attention deficit hyperactivity disorder; AI, artificial intelligence; CD, conduct disorder; OCD, obsessive-compulsive disorder; PD, Parkinson’s disease; SAD, social anxiety disorder; SZ, schizophrenia.
Rethinking psychosis taxonomy based on brain function
We begin with a discussion on phenotypes. Currently, four levels of phenotypes are frequently studied in psychiatry (figure 3A). The first level, which we call ‘micro-objective phenotypes’, consists of measurable neuronal activities (microscopic or mesoscopic) and biomolecular (DNA, RNA, protein or metabolite) features. The second level, ‘macro-objective phenotypes’, includes macroscopic brain images, eye movement features, behaviour traits, skin test performance, body shape and vital signals; these can be measured by general medical equipment, some of which can be portable. The third level of phenotype, ‘brain functional phenotypes: objective aspect’, includes brain functions or symptoms which are usually measured by a third person administering tests or questionnaires, such as assessments of memory or language. The fourth level of phenotype, ‘brain functional phenotypes: subjective aspect’, addresses psychological structures or schemes, such as views of the world and one’s own life, and can only be measured by self-reported questionnaires. Current brain projects focus mainly on exploring the first and the second level of phenotypes in the brain, while BFB core symptoms in psychoses mainly belong to the third level of phenotype. Moreover, in the third level, various mental disorders can be matched to abnormalities of specific brain functions. In this way, we further constructed a hierarchical brain function pyramid, as shown in figure 3B.
The bottom tier of the brain function pyramid is the brain functions related to sensory channels, and their abnormalities could induce sensory losses, such as blindness. The second tier is the brain functions related to vital activities; abnormalities in these functions lead to diseases such as insomnia, attention deficit disorder and Alzheimer’s disease. The third tier is the brain functions related to adaptive performance; deficits in this area will induce diseases such as autism, mood disorders and addictions. The fourth tier is the brain functions related to subjective initiatives, such as logical thinking and creativity; their abnormalities may be responsible for disorders like schizophrenia. The fifth and last tier of the pyramid corresponds to the phenotype level of ‘brain function: subjective aspect’. Its disorganisation will lead to psychological problems. This tier is also associated with consciousness and self-awareness, so we attribute conditions such as coma to its abnormality.
The brain function pyramid is organised as a hierarchy, indicating that the aspects are interdependent. For example, depression is considered an affection abnormality: it may be induced by an original anomaly in the lower tiers of brain function, such as sleep rhythm or memory disturbances, and may simultaneously affect the neighbouring or upper tiers of brain function, such as interpersonal skills or imagination. Similarly, in addition to the core symptoms of memory and learning ability disruptions, language and logical thinking problems could also be involved in Alzheimer’s disease. The pyramid design also allows for more complicated conditions where all brain functions are connected as a network by back-and-forth mechanisms. We hope this pyramid model could function as a research tool to assist in sorting biopathological structures and brain functional liabilities of mental disorders, identifying their BFB core symptoms and enlightening the design of psychiatric studies. We welcome any reasonable modifications to this framework and hope that it can be updated regularly as our understanding of psychosis deepens with time.
A proposed research paradigm
For discussion, we propose a research paradigm here that could be applied in studies of human samples to locate the causal biological pathway for psychoses.
STEP 1: Identify a brain function-based (BFB) core symptom. Researchers can learn from knowledge databases, rely on clinical insights or refer to our brain function pyramid to list candidate BFB symptoms for specific disease(s) under investigation. Then validate the symptoms in pilot brain imaging or bioassay studies to obtain the final BFB core symptom that is mostly related to the biological disturbance of the psychosis.
STEP 2: Recruit a cross-sectional cohort including specific patients and healthy controls. The sample size should be carefully determined to obtain adequate statistical power in subsequent analyses.
STEP 3: Collect biological phenotype data of interest. The phenotypes should include the BFB core symptom (quantitative), the whole genome (all SNPs or base pairs) and other biologically reasonable phenotypes in the levels of ‘micro-objective phenotypes’ (using platforms like molecular-functional MRI50 and potential mesoscopic imaging platforms) or ‘macro-objective phenotypes’ (figure 3A). The brain projects will signigicantly aid the selection of phenotypes in this step, as more and more biological mechanisms underlying specific brain fucntions will be revealed in the process.
STEP 4: Conduct causal inference analysis, including Mendelian randomisation51 and the Bayesian network method,52 to construct a causality network of the selected phenotypic traits.
STEP 5: Trim and optimise the causality network based on biological facts53; this will probably generate a causality chain (ie, the causal biological pathway) starting with genetic signals or other biophenotypes and pointing to the end of the core symptom.
STEP 6: Animal and cellular studies, such as those using non-human primate models54 and brain organoids,55 or longitudinal cohort studies can be conducted to validate the resultant causal pathway. For example, a correct causal pathway could induce psychotic-like symptoms in animals and help predict the onset or prevent the progression of the disease with high efficiency.
The novel features of this proposed paradigm include the following: (1) the application of BFB core symptoms; (2) the collection of mesoscopic and microscopic data from imaging platforms (though related technology has not yet been fully developed); (3) the application of causal inference analysis; (4) the optimisation of mathematical networks with updated biological facts and understanding; (5) the validation of results by longitudinal cohort studies. In this manner, any environmental or genetic factors inducing the causal biological pathway could be considered as risk factors especially for the subgroup of patients with the specific BFB core symptom. Similarly, any molecules or stimulants (such as sound, light, electricity or magnetism)56 57 that can rebalance the causal pathway could be regarded as potential treatments or therapies. This research paradigm could have multiple variations adjusted according to specific study purposes.
Conclusion
Psychosis is caused by the complicated interactions of genes and the environment. From national genome project to national brain project, the forceful development of technology has fuelled the next wave of studies decoding the mechanisms of psychoses. This article joins the efforts to pinpoint the elusive biological mechanism of psychosis, while a more holistic understanding of the disease is required as a precondition for appropriate study design.58 Given the excellence of the researchers participating in this work, we look forward to new research methods and exciting breakthroughs that can brighten the future of psychiatry.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Liya Sun obtained her bachelor's degree in Biological Science and Technology from Shanghai Jiao Tong University (SJTU) in China in 2008, and obtained a PhD in Biochemistry and Molecular Biology from SJTU in 2015. She is currently a scientific editor and assistant researcher at the editorial office of Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine in China since 2021. Her main research interest resides in precision medicine in psychiatry which aims to search for pathology-based and clinic-friendly biomarkers and treatments for schizophrenia and other mental disorders.
The Bio-X Institutes of SJTU was formed in 2005 by merging the Neuropsychiatric and Human Genetics Group (NHGG) and the Bio-X Life Science Research Institutes, representing a landmark in interdisciplinary research among the life sciences. To make significant progress in understanding the mechanisms underlying psychiatric disorders is one of the ambitious future plans of the Institutes (http://www.bio-x.cn/En).

Footnotes
Twitter @NO
Contributors LS wrote the manuscript. MX provided suggestions on statistics. YS provided suggestions on genomics and genetics. YX provided suggestions on brain function models. JC provided suggestions on brain projects and the article title. LH supported the idea and provided suggestions on overall manuscript.
Funding This study was funded by the National Natural Science Foundation of China (grant number: 81901354).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.