Article Text

Abstract
China’s population has rapidly aged over the recent decades of social and economic development as neurodegenerative disorders have proliferated, especially Alzheimer’s disease (AD) and related dementias (ADRD). AD’s incidence rate, morbidity, and mortality have steadily increased to make it presently the fifth leading cause of death among urban and rural residents in China and magnify the resulting financial burdens on individuals, families and society. The ‘Healthy China Action’ plan of 2019–2030 promotes the transition from disease treatment to health maintenance for this expanding population with ADRD. This report describes related epidemiological trends, evaluates the economic burden of the disease, outlines current clinical diagnosis and treatment status and delineates existing available public health resources. More specifically, it examines the public health impact of ADRD, including prevalence, mortality, costs, usage of care, and the overall effect on caregivers and society. In addition, this special report presents technical guidance and supports for the prevention and treatment of AD, provides expertise to guide relevant governmental healthcare policy development and suggests an information platform for international exchange and cooperation.
- cognition disorders
- economics, behavioral
- public health administration
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
According to the seventh Chinese national census of 2020, individuals aged 60 years and above and those aged over 65 years totalled 264 018 766 and 190 635 280, accounting for 18.70% and 13.50% of the population, respectively.1 Compared with the 2010 census figures, China’s ageing population grew faster, and the incidence rate, morbidity and mortality of diseases associated with ageing were significantly higher.2 Alzheimer’s disease (AD) incidence continues to increase, and its social and economic burden is magnifying, posing major medical and social problems that threaten China’s urban and rural residents.3 4 According to a recent national cross-sectional study, China has 15.07 million individuals aged 60 years and over with dementia, including 9.83 million with AD, 3.92 million with vascular dementia and 1.32 million with other forms of dementia. In addition, the prevalence of mild cognitive impairment (MCI) in those over 60 years of age is 15.5%, with 38.77 million individuals affected by it.5 A national study showed that the 2015 annual treatment cost of patients with AD in China was US$167.74 billion, with ever-rising treatment costs expected to reach US$1.8 trillion by 2050.6 However, the country’s diagnosis and treatment rate for AD remains low, with few medical specialists and minimal public awareness. Therefore, improving the prevention and treatment of AD under the government’s leadership is urgent.7–9
The China Alzheimer Report 2022 was jointly compiled with input from various experts and researchers in China. This report was designed to support the implementation of the Healthy China Action plan (2019–2030),10 provide effective measures to prevent and slow down the occurrence of AD, reduce the burden on families and society and respond to WHO recommendations. The China Alzheimer Report 2022 specifically describes epidemiological trends, evaluates the economic burden of disease, outlines current clinical diagnosis and treatment status and delineates existing public health available resources for AD and related dementias (ADRD). In addition, this special report presents technical guidance and supports for the prevention and treatment of AD, provides expertise to guide relevant governmental healthcare policy development and suggests an information platform for international exchange and cooperation. Finally, it strives to align with international standards regarding ADRD while also addressing issues specific to China.
Data source and analysis
The burden of disease data for ADRD was collected from the 2019 China provincial section of the global burden of disease (GBD) research. The GBD used multiple reliable data sources and adopted a unified and comparable method to comprehensively analyse the burden of disease in countries or regions worldwide from 1990 to 2019.11 12 The death data mainly were taken from the cause of death monitoring in the China Disease Surveillance Point System and the cause of death registration report information system of the Chinese Center for Disease Control and Prevention. Prevalence data in China were derived from relevant surveillance, large-scale surveys, and systematic reviews of published literature.13 Other important data sources included the monitoring of chronic diseases and their risk factors in China, the survey of Chinese residents’ nutrition and health status and the national health service survey.
Specific data sources could be found in the GBD Global Health Data Exchange Index (http://ghdx.healthdata.org). The classification and coding of diseases accorded to the International Statistical Classification of Diseases and Related Health Problems (ICD-10). The coding range for ADRD in ICD-10 is F00–F03.91 and G30–G31.9.
A summary of the detailed processes for estimating the burden of disease found in relevant published GBD literature is as follows: (1) for the estimation of cause-specific death, after redistributing the garbage codes in the cause of death data, we used the cause of death ensemble model to estimate the all-cause death rates and cause-specific death rates; (2) for estimating the prevalence of disease, we used Bayesian meta-regression to estimate the prevalence and distribution of related sequelae and used crosswalking to adjust the data of non-standard disease definitions to correspond to the standard definitions of GBD disease; (3) for the estimation of years lived with disability (YLD), YLD was obtained by multiplying the number of patients with the disease or its sequelae by the corresponding GBD disability weight; (4) for the estimation of years of life lost due to premature mortality (YLL), YLL was calculated by multiplying the number of cause-specific deaths by the GBD reference life expectancy corresponding to that age; (5) disability-adjusted life years (DALYs) were the sums of YLD and YLL .
A previous study showed that 63%–70% of persons with ADRD had AD.14 15 To fully describe the 2019 distribution of ADRD in China and various provincial administrative regions, the present study used DALY, YLL and YLD to estimate the disease burden of ADRD, to compare the cause of death and DALY ranking changes in urban and rural residents and to compare the main results of China with the rest of the world. Age-specific death rates, prevalence, YLL rates, YLD rates and DALY rates were all used to estimate the age-distributive characteristics of ADRD disease burden. When we calculated the age-specific prevalence and death rate, we divided all patients into 10 groups: 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84, ≥85 years of age. The report used GBD 2019 world standard population to standardise the death rates, prevalence, YLL rates, YLD rates and DALY rates. The distribution of ADRD burden in the provincial administrative regions in 2019 is found in the following tables.
Epidemiology and disease burden of ADRD in China
In 2019, the number of current patients with ADRD in China was 13 143 950 (table 1). The incidence of ADRD in all provinces and municipalities across the country was (56.47–207.08)/100 000, and the age-standardised incidence rate in the country was (96.28–117.32)/100 000. In addition, the ADRD prevalence in China was 924.1/100 000, the age-standardised prevalence was 788.3/100 000, the death rate was 22.5/100 000 and the age-standardised death rate was 23.3/100 000 (table 2). In total, the prevalence and death rate of ADRD were slightly higher than the global levels, and the data reflected higher rates for women than those for men. By gender, the prevalence rate (1188.9/100 000) and the death rate (30.8/100 000) of females were respectively higher than the prevalence rate (669.3/100 000) and death rate (14.6/100 000) of males. Interestingly, a pilot study in Shanghai using hospital-based samples reported a similar survival trend of patients with AD compared with that of the general population. Poor cognitive status and comorbid diabetes had a negative impact on the survival of patients with AD,4 and a noteworthy association between AD and specific types of cancer was observed in China.16
Prevalence of ADRD in China in 2019
Deaths due to Alzheimer’s disease and related dementias in China in 2019
Ranking changes of ADRD in China from 1990 to 2019
Cause of death ranking changes of ADRD in China
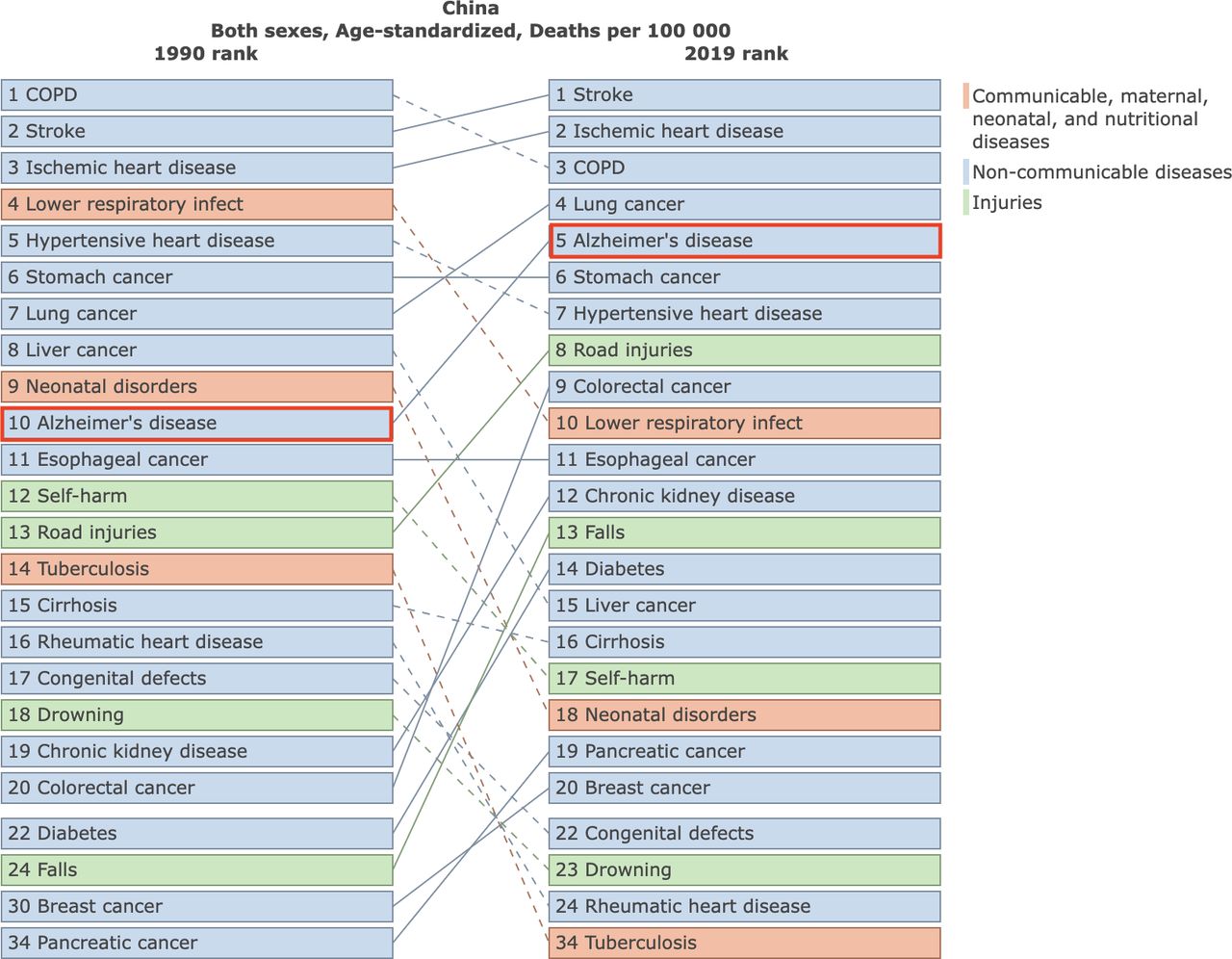
In 2019, the top five causes of death were cerebrovascular diseases, ischaemic heart diseases, chronic obstructive pulmonary diseases, lung cancer and AD, respectively. In the past 30 years, the ranking of AD deaths in China rose from 10th in 1990 to 5th in 2019, even though the age-standardised death rate declined by 0.39% (figure 1).

Change in the ranking of Alzheimer’s disease and related dementias deaths in China from 1990 to 2019. COPD, chronic obstructive pulmonary disease.
Disability-adjusted life years ranking changes of ADRD
The disease burden of ADRD in China from 1990 to 2019 rose from 27th to 15th, with a 5.7% increase of age-standardised DALY (figure 2).

Change in the DALY ranking of Alzheimer’s disease and related dementias in China from 1990 to 2019. COPD, chronic obstructive pulmonary disease; DALY, disability-adjusted life year.
ADRD comparison between the world and China in 2019
ADRD death comparison between the world and China
In 2019, deaths due to ADRD worldwide reached 1 623 276 (407 465–4 205 719); China contributed 320 715 (76 156–843 371) deaths or 19.8% of the world total (table 2). The age-standardised death rate for ADRD in the world reached 22.9/100 000 (5.8/100 000–59.2/100 000); China reached 23.3/100 000 (5.7/100 000–61.3/100 000), which was slightly higher than the world level.
ADRD prevalence worldwide compared with that in China
In 2019, there were 51 624 193 (44 276 969–59 021 502) individuals with ADRD in the world; in China the number of patients with ADRD was 13 143 950 (11 021 211–15 299 015), accounting for about 25.5% of the global population (table 1). The global age-standardised prevalence of ADRD was 682.5/100 000 (585.2/100 000–782.7/100 000); in China it was 788.3/100 000 (664.6/100 000–912.8/100 000), which was higher than the global level.
ADRD DALY worldwide compared with that in China
In 2019, the ADRD DALY worldwide reached 25 276 989 (11 204 523–54 558 243), of which 23% of the burden came from China (5 977 040 (2 678 980–13 100 564)). The global age-standardised DALY rate was 338.6/100 000 (151/100 000–731.3/100 000), while the age-standardised DALY rate in China was 368.5/100 000 (165.4/100 000–795.2/100 000) (table 6), which was slightly higher than the global level.
Deaths due to ADRD in China in 2019
Deaths due to ADRD by gender
As shown in table 2, the 2019 female death rate was 30.8/100 000 (7.3/100 000–80.2/100 000), twice as high as the male death rate of 14.6/100 000 (3.4/100 000–42.0/100 000). After age standardisation, the female death rate (24.9/100 000) was still higher than the male death rate (20.3/100 000).
Deaths due to ADRD by age groups
Age group analysis of ADRD deaths and rates among the population over 40 years old in 2019 showed a rise with advancing age and reached the highest point in the 85 years and over age group. Deaths for men in the over 85 years age group totalled 32 145, and the death rate was 945.4/100 000; deaths for women in this age group totalled 107 958, and the death rate was 1385.0/100 000. In all age groups, the death rate due to ADRD was higher for women than that for men.
Deaths due to ADRD by provinces and municipalities
In 2019, provinces and municipalities with higher crude ADRD death rates were mainly concentrated in coastal cities, such as Shanghai Municipality (34.0/100 000), and other areas of China, such as Chongqing Municipality (32.1/100 000), Jiangsu Province (31.1/100 000) and Zhejiang Province (30.1/100 000). After age standardisation, the ADRD death rate order of rank for municipalities and provinces was: (1) Tianjin Municipality (27.3/100 000), (2) Hebei Province (26.5/100 000), (3) Chongqing Municipality (25.3/100 000), (4) Zhejiang Province (25.2/100 000) and (5) Sichuan Province (25.1/100 000). The ADRD death rates in Northeastern China and parts of Central China were relatively low (table 3).
The burden of Alzheimer’s disease and related dementias in various provinces, autonomous regions and municipalities in China (/100 000)*
Prevalence of ADRD in China in 2019
Prevalence of ADRD by gender
As shown in table 1, in 2019 the number of individuals with ADRD in China reached 13 143 950 (11 021 211–15 299 015), of which the male prevalence was 669.3/100 000 (555.0/100 000–780.1/100 000) and the female prevalence was 1188.9/100 000 (1003.6/100 000–1379.0/100 000). The prevalence of female patients with ADRD was about 1.8 times that of male patients with ADRD. After age standardisation, the standardised prevalence rate of women (871.7/100 000) was still significantly higher than that of men (663.9/100 000).
Prevalence of ADRD by age groups
In 2019, ADRD numbers and prevalence rates for the male and female population aged over 40 years were on the rise and showed a rapid increase in people between 70 and 74 years of age. Men in the 80–84 years age group reached the highest number, with a total of 1 004 237 and a prevalence of 11 990.7/100 000. Women aged 85 years and over reached the highest number, with a total of 2 277 864 and a prevalence of 29 222.2/100 000. The prevalence rates of all age groups showed that rates for women were higher than those for men.
Prevalence of ADRD by provinces and municipalities
In 2019, the provinces and municipalities with the highest prevalence of ADRD were mainly concentrated in the Northeast, Eastern China and some central regions, including Jiangsu Province (1212.1/100 000), Shanghai Municipality (1137.6/100 000), Jilin Province (1081.4/100 000), Zhejiang Province (1078.6/100 000) and Liaoning Province (1077.5/100 000). After age standardisation, the areas with higher prevalence rates were found mainly concentrated in Northern China, Southern China and parts of Northeastern China. The top five ranking provinces and municipalities were Hebei Province (928.5/100 000), Henan Province (889.3/100 000), Jilin Province (882.4/100 000), Guangdong Province (845.5/100 000) and Zhejiang Province (815.6/100 000) (table 3).
Years of life lost due to ADRD in China in 2019
YLL due to ADRD by gender
As shown in table 4, in 2019, YLL due to ADRD in China reached 4 113 696 (972 998–11 434 550), with the YLL of females significantly higher than that of males. The YLL rate for males was 212.4/100 000 (48.4/100 000–603.1/100 000) and for females was 369.0/100 000 (87.3/100 000–1018.6/100 000), which was about 1.7 times the rate of males. After age standardisation, the standardised YLL rate was the same for males and females (274.6/100 000).
Years of life lost (YLL) due to Alzheimer’s disease and related dementias in China in 2019
YLL due to ADRD by age groups
In 2019, YLL due to ADRD and the proportion of individuals in the over 40 years age group increased for both men and women. There was a dramatic increase in individuals in the 75–79 years age group. Men aged 80–84 years had the highest YLL, with a total of 340 629 and a YLL rate of 4067.1/100 000. Women aged 85 years had the highest YLL, with a total of 825 079 and a YLL rate of 10 584.7/100 000.
YLL due to ADRD by provinces and municipalities
In 2019, provinces and municipalities with high ADRD, YLL rates were mainly concentrated in Eastern China and parts of Southwestern China, including Chongqing Municipality (410.9/100 000), Shanghai Municipality (390.0/100 000), Jiangsu Province (372.2/100 000), Zhejiang Province (357.1/100 000) and Sichuan Province (351.1/100 000). After age standardisation, the areas with higher YLL rates were mainly concentrated in Northern China and Western China. The top five ranking provinces and municipalities were Tianjin Municipality (297.7/100 000), Hebei Province (289.3/100 000), Chongqing Municipality (277.2/100 000), Sichuan Province (276.1/100 000) and Qinghai Province (275.3/100 000) (table 3).
Years lived with disability due to ADRD in China in 2019
YLD due to ADRD by gender
As shown in table 5, in 2019, YLD due to ADRD in China reached 1 863 344 (1 312 518–2 518 524), and the YLD for females was significantly higher than that for males. The YLD rate for males was 94.4/100 000 (66.1/100 000–127.9/100 000), and for females, it was 169.1/100 000 (118.7/100 000–228.1/100 000), which is about 1.8 times that of males. After age standardisation, the standardised YLD rate for females (125.2/100 000) remained higher than that of males (97.3/100 000) (table 5).
Years lived with disability (YLD) due to Alzheimer’s disease and related dementias in China in 2019
YLD due to ADRD by age groups
In 2019, ADRD YLD numbers for both men and women increased with ageing and were similar between the 80–84 years and over 85 years age groups. YLD rates showed a rapid increase in individuals in the 75–79 years age group. Men aged 80–84 years had the highest number with 111 206 and a YLD rate of 3270.7/100 000. Women aged over 85 years had the highest number with 352 324 and a YLD rate of 4519.9/100 000.
YLD due to ADRD by provinces and municipalities
In 2019, the provinces and municipalities with high ADRD YLD rates were mainly concentrated in Eastern China and parts of Southwestern China, including Chongqing Municipality (173.5/100 000), Jiangsu Province (173.0/100 000), Shanghai Municipality (163.1/100 000), Zhejiang Province (153.6/100 000 and Jilin Province (152.2/100 000). After age standardisation, the regions with higher YLD rates were mainly concentrated in Northern China, Southern China and parts of Northeastern China. The top five ranking provinces and municipalities were Hebei Province (133.9/100 000), Henan Province (128.7/100 000), Jilin Province (128.5/100 000), Guangdong Province (122.3/100 000) and Zhejiang Province (117.0/100 000) (table 3).
Disability-adjusted life years due to ADRD in China in 2019
DALYs due to ADRD by gender
As shown in table 6, in 2019, DALY due to ADRD in China reached 5 977 040 (2 678 980–13 100 564), of which 31.2% was disability-related burden, and 68.8% was premature death-related burden. The DALY rate for females was significantly higher than that of males. The DALY rate for males was 306.8/100 000 (135.3/1 00 000–704.3/100 000); for females, it was 538.1/100 000 (246.7/100 000–1154.7/100 000), which is about 1.8 times higher than the rate for males. After age standardisation, the standardised DALY rate for females (399.9/100 000) remained higher than that for males (321.3/100 000) (table 6).
Disability-adjusted life years (DALYs) due to Alzheimer’s disease and related dementias in China in 2019
DALYs due to ADRD by age groups
In 2019, ADRD DALY numbers and rates for both men and women increased with ageing and showed a rapid increase in the 75–79 age group. Men aged 80–84 years had the highest number of DALY with 505 000 and a DALY rate of 6029.7/100 000. Women aged 85 years and above had the highest number of DALY with a total number of 1 177 403 and a DALY rate of 15 104.6/100 000.
DALYs due to ADRD by provinces and municipalities
In 2019, the provinces and municipalities with high ADRD DALY rates were mainly concentrated in parts of Southwestern China and Eastern China, including Chongqing Municipality (584.4/100 000), Shanghai Municipality (553.1/100 000), Jiangsu Province (545.1/100 000) and Zhejiang Province (510.7/100 000). After age standardisation, the regions with higher DALY rates were mainly concentrated in parts of Northern China, Southwestern China and Eastern China. The top five ranking provinces and municipalities were Hebei Province (423.2/100 000), Tianjin Municipality (414.5/100 000), Chongqing Municipality (391.8/100 000), Zhejiang Province (391.1/100 000) and Sichuan Province (390.2/100 000) (table 3).
Diagnostic approaches for ADRD in China
Neuroimaging examination
Routine imaging technologies
To identify the degree of brain atrophy and possible causes of cognitive disorder, magnetic resonance imaging (MRI) and computed tomography (CT) are of the utmost importance in diagnosing AD. MRI is the first choice for its irreplaceably high resolution in neuroimaging, while CT serves as an alternative for patients with contraindications to MRI (eg, heart pacemaker). Routine sequences for MRI include T1-weighted imaging, T2-weighted imaging, fluid-attenuated inversion recovery and diffusion-weighted imaging.17 Although highly anticipated in cognition-related scientific research, other acquisition technologies, such as resting-state and task-state functional MRI, still have a long way to go before being widely used in clinical diagnosis.
Molecular imaging technology
The AD research framework (eg, amyloid-beta, tau, and neurodegeneration (ATN) system), established by the National Institute on Aging and Alzheimer’s Association (NIA-AA) in 2018, highlights the importance of positron emission tomography (PET) in the diagnosis of AD from the preclinical stage to the dementia stage.18 Depending on the substances targeted by radioactive tracer, AD-related PET examinations can be classified into three main kinds: Aβ-PET, tau-PET and fluorodeoxyglucose (FDG)-PET. However, the application of PET examination continues to be restricted by its relative expense and a lack of effective targeted therapies focusing on eliminating Aβ, tau or other pathological depositions.19 Whether it merits broad application in clinical work requires a comprehensive evaluation of its economic costs and health benefits.
Aβ-positron emission tomography
Increasing importance has been attached to Aβ-PET as it allows qualitative and semi-quantitative measurement of β-amyloid in the brain in vivo. The prevailing Aβ tracers include 11C-Pittsburgh compound B (11C PiB), 18F-florbetapir (namely 18F-AV-45, most commonly used in China), 18F-florbetaben and 18F-flutemetamol.20 It was reported that the sensitivity of Aβ-PET could reach 80%–100%, with a specificity of 66%–96%,21 leading to increased accuracy and confidence in the diagnosis. Meanwhile, the detection of preclinical AD raises the unresolved, inevitable ethical issue: whether and how to disclose the positive result of Aβ-PET to the examinees and their relatives.
Tau-positron emission tomography
Tau-PET, by definition, targets pathological tau protein and its filamentous aggregates deposited in the brain. For typical AD, tau’s distribution and expansion pattern follow the Braak hypothesis that pathological depositions progress from the entorhinal cortex to the neocortex.22 The most widely used drug approved by the United States Food and Drug Administration (FDA) to image tau for patients with AD is 18F-flortaucipir (Avid Radiopharms).23
Fluorodeoxyglucose-positron emission tomography
With a label of radioactive 18F, FDG is used to measure the level of glucose metabolism in the brain. AD is characterised by decreased metabolism in the posterior cingulate gyrus and frontoparietal lobe, with the frontal lobe being gradually affected as the disease progresses.24 Research conducted by Mayblyum et al 25 showed that compared with 11C PiB-PET measurement alone, a combination of high PiB and low entorhinal FDG uptake measurements could better distinguish prodromal AD from older persons with normal cognition. Meanwhile, it is essential to note that FDG-PET has an edge in the differential diagnosis of dementia and identifying the subtype of AD as it can intuitively visualise the low metabolic foci.
Neuropsychological assessments
To determine the extent to which global cognition or specific cognitive domains are impaired, professionally conducted neuropsychological assessments are necessary. Selecting appropriate scales can assist clinicians in making the diagnosis of dementia, evaluating the disease, and determining interventions. Neuropsychological assessments carried out routinely in memory clinics in China are as follows.
Cognitive assessments
Cognitive screening/assessing scales commonly used in memory clinics include the Alzheimer’s Disease-8 (AD-8), Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA) and Addenbrooke’s Cognitive Examination-III (ACE-III). MMSE is the first choice for clinicians to screen patients with mild-to-moderate cognitive impairment, while the utility of AD-8, also useful but somewhat basic, is limited to primary screening. The prevailing Chinese version of the MMSE, translated and validated by Katzman et al,26 has been widely used for >30 years because of its satisfactory sensitivity and specificity in detecting dementia. Due to the latent ‘ceiling effect’ and ‘floor effect’, it is not suitable to use MMSE alone to detect cognitive impairment in MCI or early AD, especially for those individuals who are highly educated. Thus, further evaluation by the MoCA, ACE-III, or other more comprehensive scales is necessary.
The MoCA is highly sensitive in assessing patients in the early stages of dementia. The Chinese version of the MoCA varies with cultural and regional differences. Five mainstream versions are the Beijing, Changsha, Guangzhou, Hong Kong, and Taiwan versions. Additionally, because the language-related task in the MoCA is not suitable for patients with low education, a specially revised version, the MoCA basic, was drafted and validated by Chen et al and Huang et al.27 28 Other cognitive scales testing global cognition (eg, ACE-III) or specific domains (eg, Auditory-Verbal Learning Test) are also recommended if time allows or if carried out in a memory clinic setting. Considering the five cognitive domains—attention, memory, language, verbal fluency and visuospatial abilities—the ACE-III is highly accurate in identifying early AD and frontotemporal dementia. The widely used Chinese version was adapted by Fang et al 29 for the first time when the relevant cultural norms were also established.
Non-cognitive neuropsychological assessment
Apart from cognition, the evaluation of independent living skills and neuropsychiatric and behavioural symptoms plays an essential role in diagnosing and treating AD. For assessing these abilities, the activities of daily living (ADL) scale, the most widely used tool in clinical practice, is classified into two types—the basic ADL and the instrumental ADL (IADL), with the Barthel index being the most favoured. By grading abilities like toileting and dressing, it is apparent that the ADL can provide a reference for whether intensive care should be provided to the individual with dementia. In addition, brain atrophy is often accompanied by neuropsychiatric and behavioural abnormalities. The scales that evaluate these symptoms for differential diagnosis (eg, pseudodementia) and timely antipsychotic intervention are indispensable. For example, the Geriatric Depression Scale, the Neuropsychiatric Inventory (NPI), and the Hamilton Anxiety Scale are among the most commonly used scales for this purpose.
Electronic screening tools
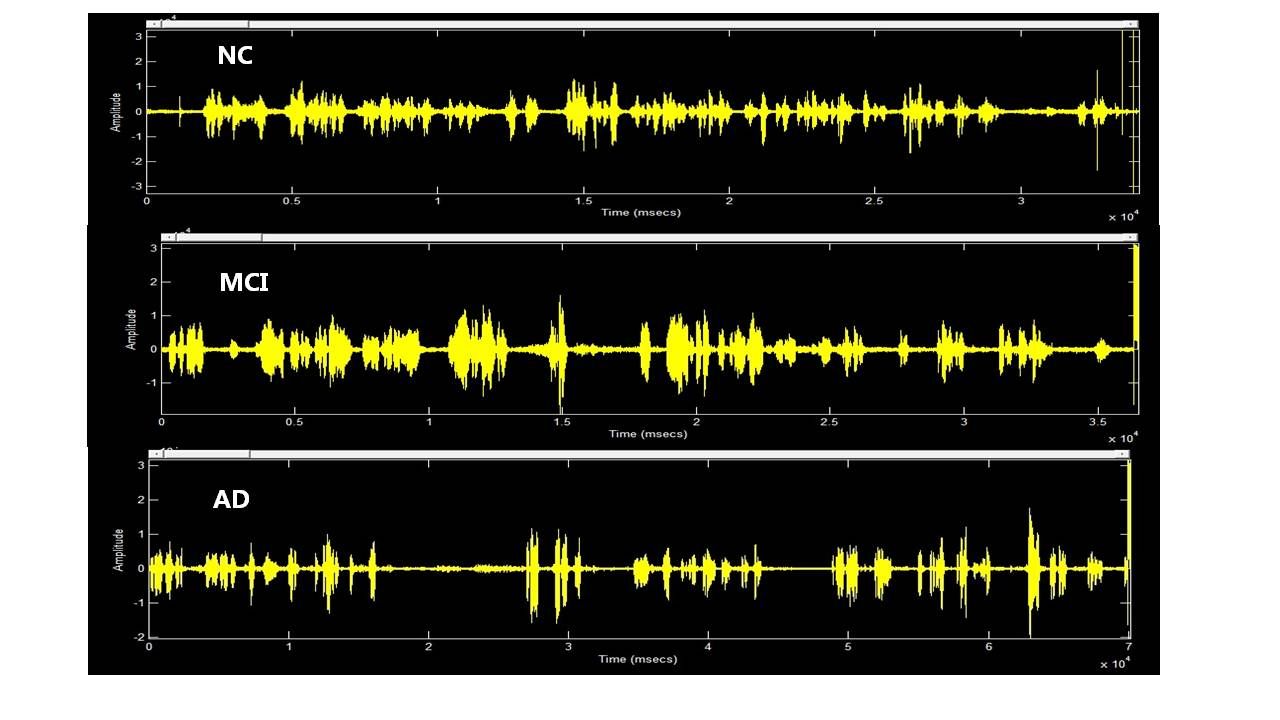
Several digital cognitive tests have emerged as popular screening tools for AD, especially in numerous community hospitals within China. Compared with traditional methods, digital screening significantly reduces the information bias resulting from examination by different clinicians. However, electronic devices may cause some difficulties for those with a low education level or poor vision and could cause excessive stress to users. Some commonly used digital screening tools include simple cognitive scales like the AD-8, IADL, and others involving tracking of eye movements and language characteristics. For example, an automatic speech recognition software programme developed by Qiao et al 30 has been shown to effectively distinguish MCI/AD from healthy controls by analysing the language features (eg, percentage of silence duration) of participants (figure 3).

Distinguishing normal controls (NC) from mild cognitive impairment (MCI) and Alzheimer’s disease (AD) using a self-developed software programme for speech analysis.97
Fluid biomarkers
An ideal biomarker reflects the pathophysiological features of AD with both high sensitivity and high specificity (≥80%). According to bodily fluids collected, AD biomarkers can be divided into three types: cerebrospinal fluid (CSF), blood and urine biomarkers.
CSF biomarkers
Similar to the AD-related PET examination mentioned above, the widely accepted CSF biomarkers mainly target Aβ (Aβ42, Aβ40) and tau protein, both recommended in the NIA-AA diagnostic framework. Multiple studies31 32 have shown that the Aβ42/40 ratio in CSF performs better when diagnosing AD and predicting progression than using Aβ42 alone, with a sensitivity of 93.3% and a specificity of 100%. Nevertheless, due to variability in current detection methods and assay batches, a unified cut-off has yet to be established.
As a biomarker of AD, CSF tau has a lower diagnostic accuracy than Aβ measurements, partly because tau-mediated neuronal damage occurs later than Aβ accumulation.33 Increased tau protein in CSF is caused by degeneration of axon and neurofibrillary tangles. Specifically, the level of total-tau (t-tau) in CSF has been shown to increase significantly by nearly 300%, with a sensitivity of 80%–90% in AD diagnosis.34 This phenomenon, however, can also be found in dementia with Lewy bodies, stroke, traumatic brain injury and Creutzfeldt-Jakob disease, suggesting elevated t-tau can only marginally help to distinguish AD from other neuronal injuries. Also, it is essential to note that tau has a variety of types of post-translational modifications, mainly phosphorylation. In comparison with t-tau, elevated phosphorylated tau (p-tau) in CSF can better characterise the pathology of AD—the formation of neurofibrillary tangles—with relatively better sensitivity (81%) and specificity (47.5%).35 More than 30 phosphorylation sites of tau protein have been found, such as p-tau181 (commonly used), p-tau217 and p-tau231. Janelidze et al showed that p-tau217 could outperform p-tau181 in differentiating AD from other neurodegenerative diseases.36
To achieve satisfactory sensitivity and specificity in AD diagnosis, it is necessary to combine various Aβ and tau biomarkers in CSF, for example, Aβ42/40 and p-tau, or even p-tau/Aβ ratio.37 However, the main limitation of the utility of CSF biomarkers is that lumbar puncture, an invasive operation, cannot be used in almost any outpatient memory clinic in China.
Blood biomarkers
A set of blood tests, including examinations of complete blood count, thyroxine, antithyroid antibodies, antisyphilis antibodies, folic acid and vitamin B12, are required for all patients with suspected AD to rule out other diseases associated with cognitive impairment. Remarkably, many new blood biomarkers are being developed and are expected to facilitate AD diagnosis or even replace CSF biomarkers in the future. Most of the blood biomarkers under development target either Aβ or tau protein.
Decreased total Aβ, Aβ42, and Aβ42/40 ratio and increased p-tau (eg, p-tau181, p-tau217) have been found in the plasma (or serum) of patients with AD as in CSF, making them potential biomarkers in diagnosis. Other promising blood biomarkers include neuro-exosomal synaptic proteins,38 neurofilament light chain39 and beta-secretase 1. It was reported that some blood biomarkers could detect AD much earlier than PET. However, it is worth noting the content of Aβ or other biomarkers in the blood is so small that testing for these measurements always comes with inevitably low sensitivity. Thus, an important area of research in this field is focused on developing better detection technologies for trace amounts of protein, for example, the optimised ELISA kit and immune-infrared sensor.40 No blood biomarker has been acknowledged by any canonical diagnostic guideline so far, suggesting there is a long way to go before its wide application.
Urine biomarkers
Previous literature suggested that urine AD7c-NTP has been demonstrated to be a sensitive and specific biomarker for diagnosing probable AD.41 42 Recently, a study by Zhang et al 42 showed that 68.8% of Aβ-positive subjects showed elevated urine AD7c-NTP levels, and AD7c-NTP level positively correlated with agitation score on the NPI. Additionally, according to the results of two Chinese pilot cohorts,43 44 both urinary monocyte chemoattractant protein-1 and dysregulated arginine metabolism are found to be potential biomarkers for diagnosing MCI/AD. However, there is also a long way to go before these can be applied in clinical work.
Genetic tests
Genetic factors have been identified as one of the most important causes and risk factors for AD. Depending on the presence or absence of familial history, AD is divided into familial AD (FAD) and sporadic AD (SAD). Most of the FAD, usually manifested as early-onset, is caused by mutations in presenilin 1 (PSEN1), presenilin 2 (PSEN2) or the amyloid precursor protein (APP).45 Of these, PSEN1 variants represented the largest proportion in Chinese FAD, and PSEN2 variants were responsible for late-onset FAD in China. Patients with the PSEN1 mutation seem to have an earlier onset age and are more likely to display language dysfunction, behavioural disorders and dyscalculia than those with the APP mutation. Thus, it is recommended that gene testing be performed on FAD families (especially those with early-onset or particular clinical phenotypes) by means of a designed gene panel, whole exome sequencing or whole genome sequencing. In contrast to early-onset AD, the major risk factor for late-onset SAD is apolipoprotein-E ε4 (APOE-ε4). It has been corroborated that carrying one APOE-ε4 allele could increase the risk of AD by 2-fold to 4-fold while the risk for APOE-ε4 homozygote could increase by 8-fold to 16-fold.46 Currently, the APOE genotype test by the PCR is available and performed routinely in most hospitals in China.
Ongoing clinical trials of potential diagnostic tools
Several diagnostic tools are being developed as the existing ones have yet to meet the urgent needs of clinics to make early AD diagnoses. The ideal diagnostic tool should have both satisfactory sensitivity and specificity in detecting AD in the early stages and use a method where samples can be easily collected (eg, peripheral blood, urine). Two diagnostic tools currently in clinical trials are the transient receptor potential canonical 6 (TRPC6) detection kit and the Elecsys CSF immunoassay (Roche).
The TRPC6 tool, developed by Wang et al 47 can supplement AD diagnosis by measuring the TRPC6 in peripheral blood and amplifying the TRPC6 mRNA using real-time PCR. Previous in vivo and in vitro studies have shown that TRPC6 could specifically interact with APP and inhibit it from being cleaved by γ-secretase, resulting in decreased production of Aβ.47 In addition, it was reported that the decreased TRPC6 mRNA in human blood cells was associated with impaired cognitive function, increased PiB uptake value and decreased CSF Aβ42.48 49 A large-scale randomised controlled trial involving six Chinese medical institutions is underway to determine the efficacy of its application.
Elecsys CSF immunoassay was designed to detect canonical biomarkers in CSF, namely Aβ42, p-tau and t-tau as mentioned, making it highly suitable for the NIA-AA system. As previously confirmed in Biomarkers for Identifying Neurodegenerative Disorders Early and Reliably (BioFINDER) (n=277) and the Alzheimer’s Disease Neuroimaging Initiative (ADNI) cohorts (n=646), the diagnosis of AD established by Elecsys biomarkers, especially t-tau/Aβ42 and p-tau/Aβ42, was in general agreement with PET classification (accuracy: 90%).50 51 According to the disclosed data from a previous global multicentre trial, Elecsys immunoassay was reported to effectively identify early AD and predict cognitive decline and conversion to AD in the non-AD elderly.52 This kit has already been approved on the market in the European Union and the USA and is going to be put into a multicentre clinical trial in China with 200 patients.
Therapeutic approaches for ADRD in China
Approved therapeutic approaches for AD
Treatments for AD include pharmacotherapy and non-pharmaceutical interventions. Pharmacotherapy includes cognitive-enhancing agents and medications for relieving the neuropsychiatric symptoms of patients with AD.53 Although numerous attempts have been made to develop effective drugs for AD, there are only a few medications approved for clinical use in China, including cholinesterase inhibitors-donepezil, rivastigmine, galantamine, Huperzine A, the N-methyl-D-aspartate receptor-antagonist memantine, Ginkgo biloba extract tablets and sodium oligomannate capsules (GV-971). However, they only provide symptomatic relief and fail to stop the progression of the disease. Atypical antipsychotics and selective serotonin reuptake inhibitors are therapeutic options for those with behavioural and psychological AD symptoms.54
GV-971 and monoclonal antibody aducanumab are the only two new drugs approved since 2003, and they shed new light on treatments for AD.55–57 GV-971, a marine-derived oligosaccharide, was approved in China in November 2019 for patients with mild-to-moderate AD. It was reported to target the brain-gut axis and may improve cognitive performance by regulating the imbalance of intestinal flora and reducing neuroinflammation.58 59 Aducanumab is a monoclonal antibody that explicitly targets Aβ, and is the first therapeutic approach to date that accurately increases Aβ protein clearance.60 It was granted ‘accelerated approval’ by the FDA for patients with mild AD on 7 June 2021, but questions remain about its efficacy and require more clinical evaluation.61 62 It is expected that the novel monoclonal antibody will be used for patients with AD in China in 2022, first in the Hainan Boao Lecheng pilot zone.63
Recent progress of clinical trials in China
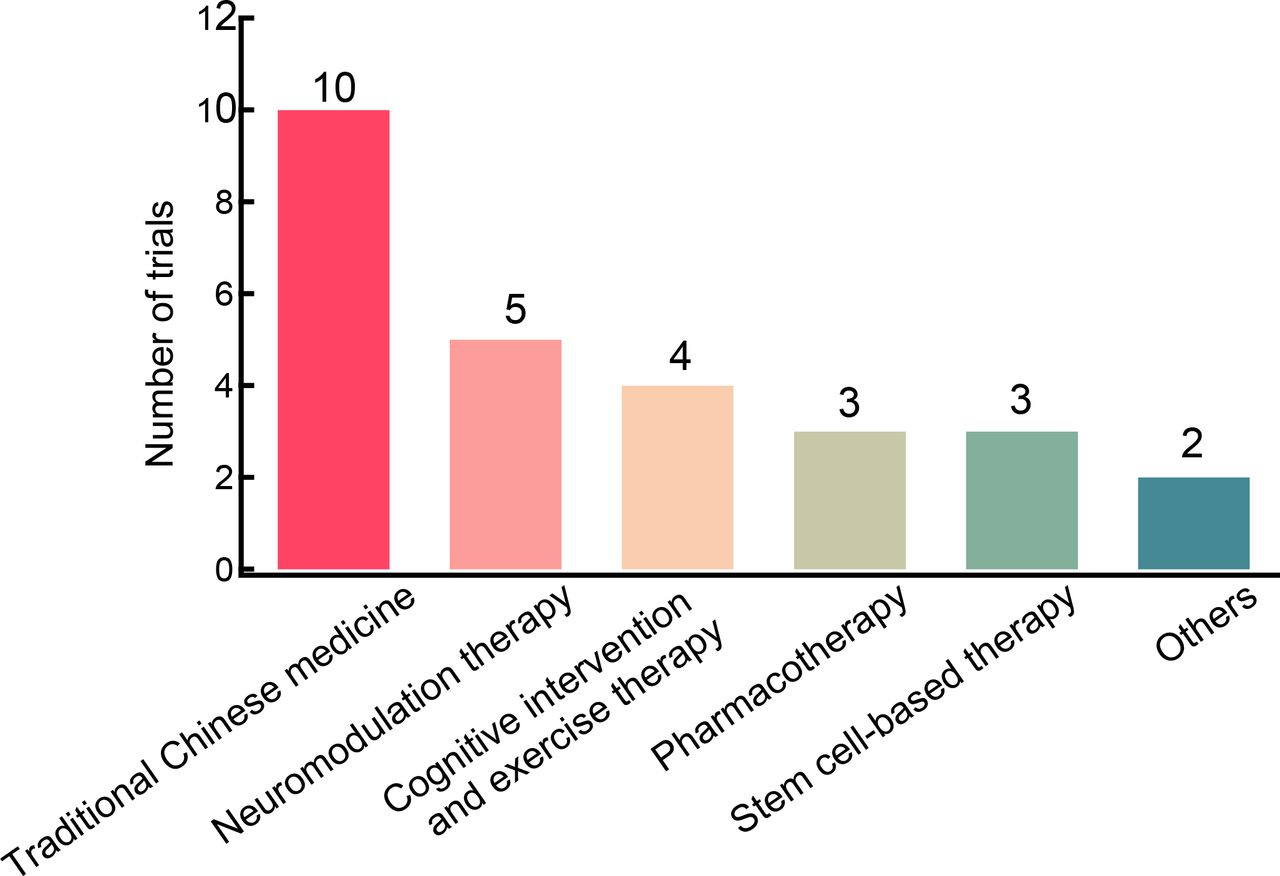
More than 200 drug candidates have failed or been suspended from clinical trials despite all the scientific efforts. In recent years, many therapeutic approaches, including anti-Aβ therapy, tau-based therapy, inflammation modulators, antioxidants, neuroprotective therapy, modulation of cellular calcium homeostasis, hypoglycaemic drugs, lipid-regulating drugs, and traditional Chinese medicine, have been investigated to explore their potential effects on patients with AD. ClinicalTrials.gov (https://www.clinicaltrials.gov/) and the Chinese Clinical Trial Registry (http://www.chictr.org.cn/) were queried to investigate the latest progress of clinical trials conducted in China. To date, 97 clinical trials have been completed in China or are still in progress, including 41 clinical trials registered since January 2019 (figures 4 and 5). Anti-Aβ therapy, neuromodulation therapy, stem cell-based therapy and traditional Chinese medicine are the main approaches involved in clinical use over the past 2 years. The latest progress in new strategies for AD is as follows.
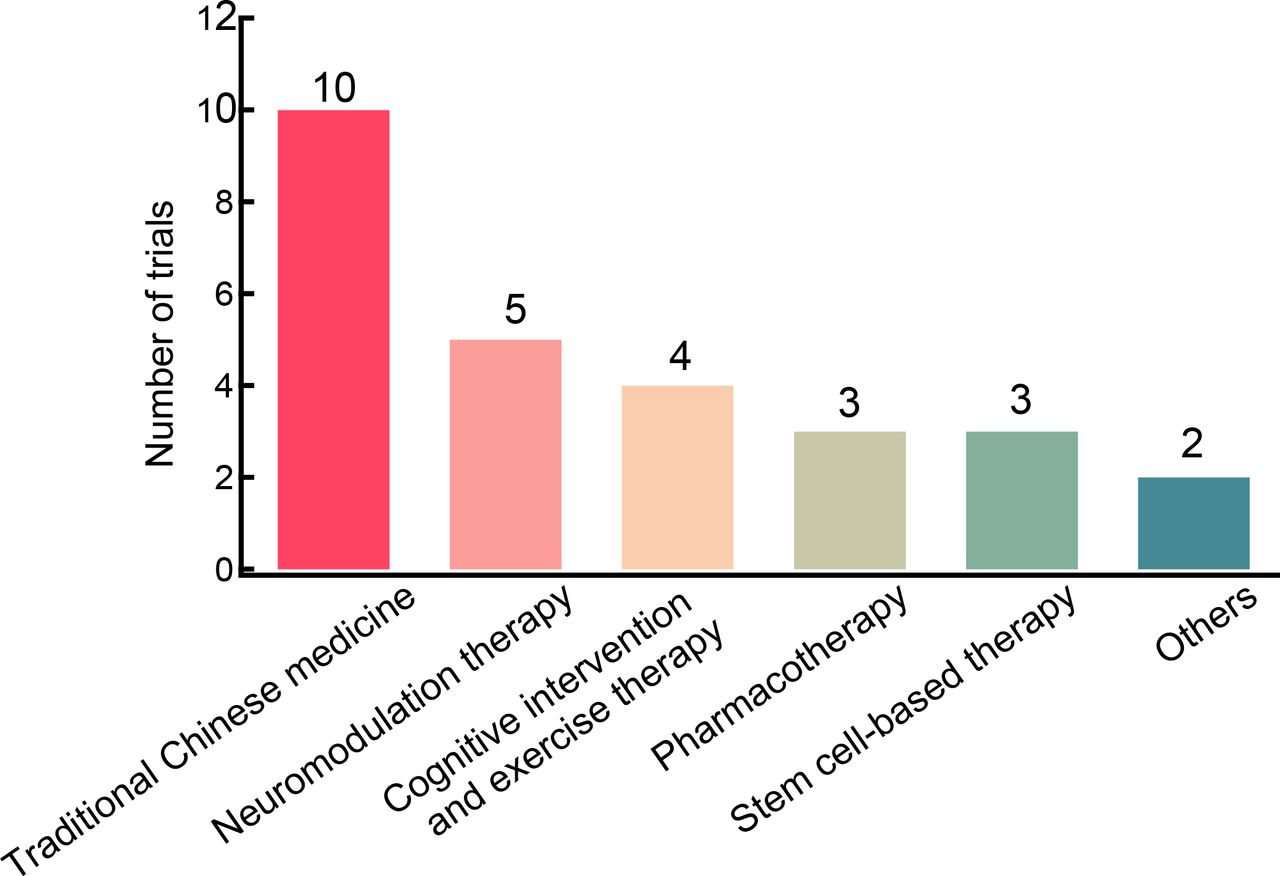
Alzheimer’s disease therapy trials registered on ClinicalTrials.gov.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Alzheimer’s disease therapy trials registered on chictr.org.cn.
Anti-Aβ therapy
Anti-Aβ therapeutic strategies aim to either increase Aβ clearance, such as immunotherapy using monoclonal antibodies against Aβ, or decrease Aβ production, including β-secretase inhibitors and γ-secretase inhibitors. Immunotherapy is considered one of the most remarkable therapeutic approaches64 and may be the first method to modify this disease.61 Currently, three monoclonal antibodies targeting Aβ are in clinical trials in China—SHR-1707, lecanemab and gantenerumab. SHR-1707 (ClinicalTrials.gov Identifier: NCT04973189) was approved for phase I clinical trials in March 2021. Lecanemab and gantenerumab, which are in international, multicentre trials, are currently in phase III. In phase II clinical trial, lecanemab revealed therapeutic potential in CSF biomarker reduction, but it failed to reach the 12-month primary end point.65 A phase III randomised trial of gantenerumab was halted early because no differences were observed in the primary and secondary end points, although it reflected dose-dependent and APOE-ε4 genotype-dependent effects on biomarker end points in prodromal AD.66 A phase III clinical trial carried out to evaluate the efficacy and safety of subcutaneous injection of gantenerumab on early AD is in progress. β-Secretase is supposed to play a pivotal role in the process of amyloid-β peptides generation. However, the β-secretase inhibitor lanabecestat failed in two phase III studies (AMARANTH and DAYBREAK-ALZ) because it failed to slow memory decline in patients with early AD and mild AD dementia. Moreover, side effects in the lanabecestat group, such as psychiatric adverse events, weight loss and hair colour changes, were reported in a higher percentage than in the placebo group.67
Neuromodulation therapy
The number of registered clinical trials of neuromodulation therapy for AD has continuously increased in recent years. Repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS) are the two most widely investigated non-invasive brain stimulation (NIBS) interventions. Accumulating evidence suggests that NIBS may be an effective method for patients with AD. Studies have found that daily tDCS at home for 6 months can improve or stabilise cognitive performance in patients with AD,68 and rTMS combined with cognitive training intervention improves memory in patients with AD.69 70 Currently, an array of registered clinical trials of tDCS, transcranial alternating current stimulation and deep brain stimulation are under investigation for their potential clinical use. However, many variables in the clinical trials, such as study design, inclusion and exclusion criteria, sample size or funding source, may lead to inconsistent results.
Stem cell-based therapy
Numerous animal studies have shown that stem cell therapy can decrease or restrain neuronal death. Self-renewal, multipotent differentiation capabilities, low tumourigenicity and immunomodulatory properties make it a promising choice for neurodegenerative diseases.71 Mesenchymal stem cells and human neural stem cells are desirable candidates for AD treatment. One phase I/II clinical trial currently in progress is looking at exosomes derived from allogeneic adipose mesenchymal stem cells (allogeneic adipose MSC-Exos) in patients with mild-to-moderate dementia due to AD. Meanwhile, two clinical trials are underway evaluating the safety and efficacy of injection of human-derived neural stem cells via nasal drip in moderate-to-severe early-onset patients with AD. Nevertheless, many problems still need to be solved before going into clinical therapeutic application, such as eliminating the immune response and improving survival rate or obtaining large-scale production of effective and compatible cells.
Chinese medicine
Recent studies showed positive effects on AD from Chinese medicine, including traditional Chinese medicine and innovative Chinese compounds. An increasing number of Chinese traditional herbal medicines, including Liuweidihuang capsules, Taisi capsules, Bushenyijing granules, Yizhi decoction and Wujiayizhi granules, have been introduced to clinical trials in the past 2 years. Acupuncture, one of the most representative non-pharmaceutical treatments in traditional Chinese medicine, has attracted increasing attention recently due to its effectiveness and few side effects. A 28-week controlled study indicated that acupuncture could improve cognition and global clinical status in patients with mild-to-moderate AD.72 Two clinical studies, Sanlian Xingshen Yizhi Acupuncture therapy and acupuncture combined with donepezil, are ongoing to evaluate the efficiency and safety of acupuncture on AD.
Other therapies
In one recent clinical trial, folic acid combined with vitamin B12 showed a positive therapeutic effect on cognition in patients with AD.73 Preclinical evidence suggested sulforaphane has a multifaceted neuroprotective effect on brain health. A randomised, double-blind, placebo-controlled study (NCT04213391) was carried out to study the efficacy and safety of sulforaphane in patients with prodromal to mild AD. In another clinical study, the antipsychotic amisulpride was used to relieve the neuropsychiatric symptoms of patients with AD. Also, music therapy combined with strong light therapy was found to improve sleep quality for those with sleep disorders.74 Non-pharmaceutical interventions, such as music therapy, cognitive interventions, aerobic exercise and diet therapy, have fewer side effects and may provide promising therapeutic options for patients with AD.
Although significant progress has been made in the past 2 years, many problems and limitations with clinical studies conducted in China continue to exist. Most trials have not been registered prior to implementation, and some have not been carried out in accordance with the standard statements of clinical trial reporting. More standardised top-level, large-sample size, multicentre studies are needed in the future.
In response to the appeal of ‘Healthy China Action (2019–2030)’,10 the General Office of the National Health Commission issued a document on how to explore more effective prevention and treatment service for patients with AD in August 2020. It aims to accelerate establishing a public service system with Chinese characteristics and explore an integrated intervention mode. In the future, the treatment of AD in China would include comprehensive management based on the patients’ life span cycle, including specific disease-modifying medications, treatment of comorbidities, early interventions for risk factors and changes in personal lifestyles.
Public health resources for the prevention and treatment of AD
In recent years, the ageing of the world’s population has intensified, and with it, the elderly population in China has grown significantly, showing a trend of accelerated increase. Along with this increase in ageing, the number of older adults with cognitive impairment also is expanding rapidly. Survey data show that from 2010 to 2020, the proportion of people aged 60 years and above in mainland China increased from 13.26% to 18.70% (from 177.65 million to 264.019 million).2 75 WHO stated that the proportion will rise to 28% by 2040.76 At the same time, the number of individuals with dementia in China is the highest in the world and is increasing rapidly. According to a nationwide cross-sectional study in 2020, the prevalence of dementia among people aged 60 years and above in China was 6.0%, and the prevalence of AD and vascular dementia were 3.9% and 1.6%, respectively.
The current context of disease-oriented outpatient service provision
Memory clinics have been established to diagnose, identify and treat patients with cognitive impairment (represented by AD) early in the course of illness while also providing nursing education for families and training for caregivers. The memory clinics offer patients timely professional diagnosis and treatment. Moreover, they have become medical units for clinical diagnosis and treatment with essential functions such as health education and chronic disease monitoring.77
Beginning the 1990s, neurology, psychiatry and geriatric departments of hospitals in large-sized and medium-sized cities in China have successively opened memory clinics; the names of these clinics have changed from the original ‘dementia clinic’ or ‘Alzheimer’s disease clinic’ to the present term, ‘memory clinic’. By 2014, 128 memory clinics had been opened in China.78 Since 2018, 26 medical institutions in Shanghai have opened memory clinics, including 11 comprehensive tertiary hospitals, 8 mental health specialty institutions and 7 primary community health service centres.
The ‘2019 China Alzheimer’s Disease Patients’ Family Survival Status Survey Report’ showed that the general population’s AD awareness had increased significantly in recent years.6 7 When symptoms of amnesia occur, >50% of individuals and their family members suspect AD in the affected party.7 The patients’ consultation rate within 1 year rose from 32.47% in 2012 to 77.43%, and timely consultation rates greatly improved. By 2019, 28.12% of all patients with AD were diagnosed in memory clinics; this high percentage reflects the vital role of memory clinics in the early detection and diagnosis of cognitive impairment disorders.
Government support and policy orientation
Government support
As the rate of population ageing in China increases, the accompanying increased risk of cognitive impairment has led to an increased social risk. In the future, this social problem is likely to escalate. The government and society are paying increasing attention to cognitive impairment disorders such as AD. In the ‘Healthy China 2030’ plan,10 the Chinese government has proposed to ‘improve effective interventions for diseases such as AD’ and ‘the public’s awareness of the prevention and treatment of AD in pilot areas will increase to 80% by 2022’.10 It is necessary to establish and improve the Alzheimer’s prevention and treatment service network; moreover, the screening rate of cognitive function among the older adults in the community is expected to increase to 80%. Additionally, it is essential to ‘establish a multidisciplinary team providing diagnosis, treatment and nursing services for patients with MCI and dementia that includes general practitioners, volunteers, social workers, psychotherapists, and so on’. In addition, the National Health Commission of the People’s Republic of China is conducting a study on the ‘Guidelines for Home Care of Older Adults with Dementia’. To reduce the occurrence of disability and dementia in the older adults at its source, on 9 April 2021, the National Health Commission of the People’s Republic of China issued the ‘Notice on Pilot Programs for the Prevention and Intervention of Disability (Dementia) in Older Adults’,78 which aims to carry out pilot programmes in 13 provinces (cities, districts). Furthermore, they formulated the ‘Technical Plan for the Pilot Prevention and Intervention of Disability (Dementia) among Older Adults’.79 The Inner Mongolia Autonomous Region and Guangdong Province collaborated in this pilot project. Recently, intervention projects have been fully implemented in cities and districts of 15 intervention provinces.
Shanghai is a large city with the most rapidly ageing population in China and was one of the first cities to witness the increase in its ageing population. In 2017, 170 000 older adults with dementia lived in Shanghai, accounting for 6.7% of older adults with registered permanent residences in Shanghai.80 The Shanghai government’s strategies for dealing with dementia are relatively advanced compared with the rest of the country, and the following shows some of their pioneering work. In the ‘Healthy Shanghai 2030 Planning Outline’,81 Shanghai proposed to ‘promote healthy ageing, be demand-oriented, build a full-coverage and integrated older adult health service system, as well as improve the health management for older adults and implement interventions for common chronic diseases, degenerative diseases and mental health problems among elderly adults’. One of the main tasks of the ‘Shanghai Implementation Plan for Developing Elderly Care Services (2019–2022)’82 is improving healthcare services for older adults with cognitive impairment. In addition, Shanghai issued the ‘Notice on Strengthening Care Services for the Elderly with Cognitive Impairment in Older Adults Care Services’,83 proposing to ‘improve institutional care, community intervention and social education for older adults with cognitive impairment to create a social environment full of concern, care and love for older adults with cognitive impairment, improve the level of care services for older adults with cognitive impairment and promote the high-quality development of older adult healthcare services’. The notice also states that efforts will be made to create more beds for the administration of cognitive care. As of the end of 2020, the city has built 4999 beds to facilitate dementia care, and by 2022, there will be 8000 dementia care beds available in the city. The latest ‘Fourteenth Five-Year Plan for the Development of Civil Affairs in Shanghai’84 was released on 13 August 2021. It once again emphasised the critical position of management and care services for older adults with cognitive impairment. Moreover, it emphasised that during the ‘14th Five-Year Plan’ period, Shanghai will continue to carry out the prevention, early identification and interventions for common mental disorders seen in older adults, such as cognitive impairment and depression. Furthermore, Shanghai will continue to prioritise pilot projects aimed at older adults and promote cognitive impairment-friendly communities to achieve full coverage in its districts. The plan also mentioned promoting the construction of cognitive impairment care beds in pension institutions, reaching 15 000 beds by the end of the ‘14th Five-Year Plan’ period.
The national government provides medical, rehabilitation, entertainment, education, and other social assistance services to disabled and older adults with dementia with particular difficulties in rural areas. The National Working Committee on Aging and other functional departments have organised several special surveys on the development of rural older adults across the country to fully understand the basic conditions of the disabled and older adults with dementia in rural areas.
Long-term care insurance
In June 2016, the Ministry of Human Resources and Social Security of the People’s Republic of China issued the ‘Guiding Opinions on the Pilot Program of Long-term Care Insurance’85 and selected 15 cities to carry out this pilot project together. Moreover, they mentioned the exploration of establishing a social insurance system that raises funds through social mutual aid and assistance to provide service guarantees for basic living care and medical care for persons with long-term disability and dementia. There were two groups of national long-term care insurance pilot projects, and 49 cities have participated in the projects as of 2021. By the end of June 2021, the total number of participants in each pilot city for long-term care insurance reached 134 million, and the cumulative number of people receiving benefits reached 152 million.
Advantages of long-term care insurance
Long-term care insurance raises funds through mutual social aid. It provides services and financial guarantees for people with long-term disabilities who have been determined to need a certain level of care for basic living and medical care. Shanghai stipulates that the long-term care insurance fund shall pay 90% of the service costs for community home care incurred by the insured persons during the effective period of the evaluation. In contrast, the long-term care insurance fund shall pay 85% of the fees for the care services provided by pension institutions that meet specific regulations.
Long-term care insurance eases the financial pressure of patients with cognitive impairment and their families who need long-term care and significantly reduces the financial burden associated with AD. Since the implementation of the long-term care insurance pilot programme, older adults who enjoy long-term care insurance have generally given positive feedback about the services provided by the programme. In addition to financial support, long-term care insurance also improves family care skills since most family caregivers lack an understanding of how to care for older adults with cognitive impairment and lack access to information. Furthermore, caregivers provide community-based home care under long-term care insurance by offering door-to-door services for older adults with cognitive impairment. The communication between caregivers and the family members of the older adults can also become a quick and accessible way for family caregivers to learn nursing knowledge. Compared with ordinary housekeeping service staff, professionally trained caregivers have more advanced professional skills and abilities.
The evaluation and support of long-term care insurance in patients with cognitive impairment
In August 2021, the National Healthcare Security Administration issued the ‘Long-term Care Disability Level Evaluation Standard (Trial)’86 requiring all pilot cities to uniformly meet the evaluation standard within 2 years. This standard evaluates the cognitive abilities of an assessed person. It uses cognitive ability and capabilities associated with daily living, perception and communication as its first-level index to comprehensively determine the long-term care disability level of the assessed person using a combined methodology. The standard mainly evaluates cognitive ability related to four aspects: orientation to time, person and place, as well as assessing memory. It also clarifies the evaluation standards and implementation targets and solves the difficulties of hidden costs and expenses caused by huge differences in the classification of disability levels between the various pilot cities.
At present, only six pilot cities have included people with dementia in long-term care insurance coverage. Shanghai has included the second to sixth grades of dementia in care insurance coverage. Many pilot cities have established dementia care areas in nursing institutions to provide services for older adults with dementia. At present, four cities have issued specifications for establishing dementia care areas. For example, the cognitive impairment bed unit set up in Shanghai adopts a ‘small unit’ layout model, which has a more flexible bed accommodation capacity. In addition, Shanghai has regulated in more detail the room layout and equipment requirements for these special areas to better meet the nursing needs of people with dementia.87
Resource allocation status for AD
Resource allocation for pension institutions
Pension institutions are essential providers of specialised cognitive impairment services. For example, some pension institutions have designated dementia care areas specifically designed to be friendly, safe environments that can better deliver daily services to patients.88 A survey in Beijing showed that the average occupancy rate of beds in the dementia care area in these institutions was 13.7% higher than ordinary beds. In recent years, Guangdong, Shanghai, Beijing and other cities have successively complied with the construction specifications, guidelines and service standards for dementia care areas; these standards are being used to guide the improvement of pension institutions and standardise related services, such as the ‘Work Plan for Dementia Care Bed Setting (Trial)‘89 and the ‘Guidelines for Dementia Care Bed Setting’90 issued in Shanghai in 2018.
There are three main types of existing pension institutions in rural areas, including social welfare institutions for older adults or retirement homes, apartments for older adults (nursing homes), and assisted living. They mainly accept older adults with no ability to work, no source of livelihood, and no one to support them financially. These older adults are guaranteed food, clothing, shelter, medical care and end-of-life/burial services, and are given various services such as daily life care and rehabilitation services. However, a serious shortage of assisted living centres in rural areas exists. Most small towns have only one nursing home that only provides water and electricity, cheap meals and simple living facilities. Also, cultural and entertainment facilities are lacking, along with little attention to the mental health of these older adults.91
Community-based and home-based resource allocation
With the further expansion of China’s elderly care service system, the importance of community-based and home-based care has gradually become more prominent. More than 90% of cognitive impairment patients in China currently choose home-based care, which is also the main future direction for dementia rehabilitation.
Different medical and elderly care institutions play various roles in preventing and treating disorders of cognitive impairment. Community health service centres are generally responsible for initial screening and intervention. In contrast, nursing homes, community day care centres and elderly care homes are responsible for the nursing care of patients. In addition, the community should be accountable for the health education of patients with cognitive impairment and their families, actively carrying out general public health intervention projects and activities that raise awareness about these issues. Finally, specialised geriatric nursing hospitals are responsible for treating patients with AD who are unable to care for themselves, are bedridden, have many complicating medical problems or require hospitalisation.
All provinces and cities have expanded their older adult services to include community and home-based care. For example, as of 2021, Jiangsu Province had built 18 200 home-based community senior service centres, 589 daycare centres and >7000 meal assistance points for older adults, with 2.6 million older people receiving specialised home-based services. At present, 77 subdistricts and towns in Shanghai have piloted the construction of the ‘Shanghai Dementia-Friendly Community’. Based on the characteristics of their respective communities and the needs of older individuals, ‘health education’ has been implemented to increase awareness of cognitive impairment among community residents. In addition, assessment of older adults in the community has been carried out to support early intervention, and training about non-drug-based interventions and guidance for family members is offered. For example, various methods of family support include psychological support, resiliency training and respite services. Finally, each subdistrict relies on community service centres for older adults and other facilities to establish a community support network for those with cognitive impairment.
Resource allocation for non-governmental organisations
Non-governmental organisations, including volunteer groups, public welfare organisations and other social members, play increasingly important roles in preventing and treating cognitive impairment disorders. They work with government agencies and communities to develop various activities, such as education and training for the general public.
For example, in 2013, the Changshou Road subdistrict in Shanghai organised public welfare organisations to open the city’s first memory school. To date, it has held >720 classes and has effectively served >14 400 people. In 2017, the Jian’ai Charity and Changshou Road subdistrict took the lead in launching the country’s first ‘Five-Year Plan’ for dementia-friendly community service in Shanghai, which has become an important project in the process of building a service system for the dementia-friendly community in Shanghai.
Volunteer organisations
Represented by Hong Kong, Shanghai and Shenzhen, various regions in China have carried out more work using volunteer services for senior citizens. Since 2008, volunteer organisations for older adults had matured to the point that they began to expand and develop rapidly. According to the China National Committee on Ageing, by the end of 2015, >540 000 associations for older adults had been established in grassroots communities nationwide, with 433.89 million people regularly participating in their activities. However, the nationwide development of volunteer services for older adults has been characterised by uneven development—large cities developing fastest, medium and smaller cities developing more slowly, and rural towns and other remote areas starting much later—with many shortcomings in the system of management and standardisation.92
The care of volunteer organisations is critical to older adults with cognitive impairment. The care from volunteers could improve their overall physical and mental health. Existing volunteer organisations mainly include student organisations and community resident organisations. According to a survey, the current volunteer organisation members were mostly students and middle-aged folks aged 65–74 years. They aid older adults and their families through phone calls or regular door-to-door visits, including chatting, cleaning, measuring blood pressure and providing relevant health information. For example, the ‘Guangci Home Ruijian Cognitive Science Popularization Volunteer Service Team’ in Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, carries out disease screening and education activities by sending volunteers to the community and family homes. Their goal and motto is ‘Early prevention, Early detection, Early diagnosis and Early treatment’. The team has also been supported by the Shanghai Voluntary Service Public Welfare Foundation.
Other public welfare organisations
Non-profit social service institutions committed to prevention and early intervention for patients with AD provide professional social support services for those in the community with cognitive impairment and their families. With the support of the Civil Affairs Bureau, city subdistricts and community organisations, they are committed to health promotion, such as community education, early screening, intervention and caregiver support. They also participated in the pilot construction of a dementia-friendly community. This involvement demonstrates the trend of social services in overall cognitive impairment healthcare provision. For example, the Beijing Senior Care Centre has been running a programme to care for seniors with dementia for 10 years. In this programme, the older adults share their life through the medium of art (eg, painting), which extends far towards meeting their deeper needs. Since 2013, Shanghai Jian’ai Charity Development Center has carried out ‘Anti-dementia Manual Assemblage’ activities in various communities to exercise the dexterity of the older adults through simple paper-cutting activities. At the same time, these activities provide a needed opportunity for older adults to interact with one another.
Self-help organisations
Self-help organisations are mainly composed of families and caregivers of older adults with dementia. They provide help to older adults through a combination of online and offline methods (such as WeChat) and participation in community activities. The families of older adults with cognitive impairment experience immense pressure in their responsibility towards caring for their family members. Self-help organisations provide caregivers with a platform for mutual communication and sharing. Through it, they learn from each other and share their struggles, creating a warm, supportive atmosphere.92
Internet technology support
Service map for cognitive impairment
The online hospital is a new application combining the internet and medical field services. It is a healthcare service platform that uses the internet as a carrier which can optimise the procedures for medical treatment and make the experience of seeing a provider more convenient. From 2011 to March 2020, the State Council, the National Health Commission, the National Healthcare Security Administration and relevant local government departments issued a total of 110 internet-related policies; from these, the online hospital began to issue pilot policies in Guizhou and Yinchuan in 2015. In 2018, the General Office of the State Council issued the ‘Opinions on Promoting the Development of “Internet Plus Medical Health”’,93 which clarified the boundaries of internet medical services. Three documents including the ‘Administrative Measures for Internet Diagnosis and Treatment (for Trial Implementation)’,94 ‘Internet Hospital Management Measures (for Trial Implementation)’95 and ‘Management Standards for Telemedicine Services (for Trial Implementation)’96 formulated by the National Health Commission and the State Administration of Traditional Chinese Medicine, further clarify the online and offline business development of online hospitals. Online services include triage, guidance, consultation, referral, appointments, registration, telemedicine (including video consultation, telephone consultation, graphic consultation, electronic prescription, billing and report query), medication guidance, health consultations, posthospital follow-ups, chronic disease management and contracting with family doctors. In contrast, offline services include providing patients with places for video consultation, health consultation, medication sales, delivery relying on retail drug enterprises and various medical services carried out after establishing cooperative relations with offline medical institutions.
With the current care service needs for cognitive impairment, the vigorous development of online medical platforms establishes a whole process service system. It includes prevention, screening, diagnosis, treatment, rehabilitation, care and support for cognitive impairment. The help of online hospitals breaks through the previous geographical and time limitations of medical institutions and nursing facilities. It effectively makes online and offline connections while significantly improving service efficiency. Moreover, it can provide convenient, accessible, evidence-based and reasonable guidance for patients with cognitive impairment and their caregivers. This can relieve their stress, which supports the prevention and treatment of cognitive impairment and further improves existing service systems.
At the beginning of 2020, the Shanghai Municipal Center for Disease Control and Prevention and the new online hospital jointly developed and improved a service map for cognitive impairment, expanding the scope of institutions and visually displaying various service resources in conjunction with special research results. Its main advantages are as follows: first, this makes it easier for experts to understand the organisation’s classification, layout and bed distribution. It also ensures that citizens can inquire about the organisation’s classification and surrounding organisations and readily obtain its general information (name, address, telephone number, bed information and pricing). Second, although cognitive impairment cannot be cured, early screening, early diagnosis and early treatment are essential for effective prevention and delay of the disease progression. It was for this reason that the platform was established via online hospitals. Functional modules such as online outpatient services, follow-up, rehabilitation, education, training, nutrition consultation, psychological counselling and legal assistance were established to conduct preliminary screening and self-testing for high-risk groups. Community families and primary, secondary and tertiary hospitals were linked to achieve hierarchical diagnosis and treatment and integrate service resources such as older adult care, which makes full use of the advantages of fast and efficient online hospital interconnection. The entire process of education, screening, referral, diagnosis, treatment, rehabilitation, nursing, care and hospice care for cognitive impairment is implemented through a combination of prevention and treatment, full-time and specialised integration, medical and nursing care and traditional Chinese and Western medicine. Third, through online video courses, live broadcasts and course training, various resources can be integrated to improve the public’s awareness of cognitive impairment. For the specific difficulties of caregivers, there are currently no support services, such as psychological counselling and legal assistance. It is foreseeable that in this new era during which COVID-19 will likely continue to affect people’s lifestyles profoundly, this online and offline integration model will play a significant role in the provision of healthcare delivery.
An example of internet medicine: the Shanghai Brain Health Alliance
The Shanghai Brain Health Alliance was implemented by the Shanghai Medical Society General Medical Section in conjunction with the online hospital. This is in accordance with the spirit and requirements of WHO’s Global Action Plan for public health, which is entitled the ‘Global Action Plan on the Public Health Response to Dementia 2017‒2025’13 and the Shanghai Municipal Government’s ‘Healthy Shanghai 2030’.81 It was established by 141 relevant institutions in the city. The Shanghai Brain Health Alliance is responsible for three main tasks. The first is to improve the clinical diagnosis and treatment of cognitive impairment in Shanghai. It aims to cooperate with Shanghai’s professional medical institutions to form a network that strives towards the prevention, screening, diagnosis, treatment, rehabilitation, standardisation of in-hospital treatment and out-of-hospital long-term management of patients with cognitive impairment. Furthermore, it aims to build a complete internal and external prevention management system, first prioritising primary diagnosis, followed by referral, acute and chronic treatment, and finally integration within the medical system to achieve ‘early prevention, early diagnosis and early treatment’. This will increase the detection and effective treatment rate of disorders and improve the city’s level of standardised prevention and treatment as a whole.
The second task is to improve the level of care for patients with cognitive impairment in the city, thus improving the collaboration and integration of healthcare and civil older adult care institutions. At the individual level, caregivers are more likely to obtain professional help, education and training to improve their care ability. At the institutional level, it will be easier to get professional medical support, enhance the quantity and quality of care institutions and improve the service level of the whole industry through the establishment of the alliance.
The third task is to enhance efficiency. An online and offline integrated prevention and care system has been built based on the online hospital platform. This overcomes obstacles posed by geography and time. For example, an online cognitive map 2.0 was launched to establish an online hospital specialised disease platform to display the city’s medical and care institutions (including parts of the Yangtze River Delta) to fully implement hierarchical diagnosis, treatment, drug distribution, evidence-based training, older adult care, rehabilitation, psychological counselling and legal assistance for the convenience of residents. Through the internet media matrix of communication and operation, promotion is used to improve the societal awareness of the disease and the concept of ‘health for all’.
Conclusion
The China Alzheimer Report 2022 is a comprehensive source of China’s socioeconomic information and the status of healthcare provisions as they pertain to dementia. Compared with the annual World Alzheimer Report, this report gives a detailed picture of ADRD within China, including epidemiological data and information on the diagnosis, treatment and public resources available for the care of those with AD. This paper is commissioned by the China AD report editorial board and includes the work of many highly respected researchers of this topic in China.7 It is an important source of information both within China and globally. It will be published biennially in the future.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors acknowledge the contributions of Dr Shengdi Chen from the Department of Neurology and the Institute of Neurology, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, in the preparation of the China Alzheimer Report 2022.
References
Dr Gang Wang is a professor and senior attending doctor, deputy chair at the Department of Neurology and Institute of Neurology, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine in China. His main research interests include the pathogenesis of Alzheimer’s disease (AD) and other neurodegenerative diseases, to find the detail molecular mechanisms and novel therapies for these neurodegenerative diseases.

Footnotes
RR, JQ, SL and XL contributed equally.
Contributors RR, JQ, SL, XL, PY, ZW, RT, JW, QH, JL, XX, YongH, SC, YuanZ, XY, PW, YiZ, YiW, YanH and HiY performed the literature search and drafted the manuscript. GW, MZ, CL and YingW designed the review and edited the manuscript. All authors read and approved the final version of the manuscript.
Funding This report was supported by a grant from Brain Science and Brain-Like Intelligence Technology of the Ministry of Science and Technology of China (2021ZD0201804).
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.