Article Text

Abstract
Background Christian clergy have often been identified as ‘frontline mental health workers’ and gatekeepers to mental health services. However, despite this, collaboration between clergy and mental health services remains poor, with some US clergy referring on as little as 10% of cases.
Aims In this study, we aimed to evaluate the collaborative relationship between UK clergy and medical practitioners, with the purpose of identifying key issues that should be addressed to improve such collaboration between the two services.
Methods We surveyed 124 clergy, 48 general practitioners and 13 psychiatrists in Wales. Part 1 of the survey covered four main themes: demographics; types of mental health cases seen by clergy and practitioners; referral rates between clergy and mental health services; attitude and relationship between clergy and mental health services. Part 2 was directed at clergy only and assessed how sensitive clergy were in identifying and referring on mental health disorders by using seven virtual case vignettes.
Results Clergy frequently encountered mental health cases and around 60%–80% regularly referred on to a healthcare professional. Clergy appeared very effective at identifying and referring on high risk scenarios, such as psychosis, suicidal ideation and substance misuse, however were less effective at identifying and referring on clinical depression and anxiety. Clergy rarely received referrals from medical professionals. Both medical professionals and clergy felt they needed to engage in a more collaborative relationship, and around of one-third of practitioners were prepared to offer training to clergy.
Conclusion Most clergy in Wales regularly encounter mental health cases and appear effective at recognising and referring on mental health disorders; however, a large minority do not (20%–40%). Clergy generally do not receive referrals from mental health professionals, despite the proven benefits. Therefore, improving collaboration, developing spiritual training for mental health professionals, and mental health training for clergy is likely useful, a notion that many clergy and medical professionals deem important and are prepared to support.
- attitude of health personnel
- community mental health Services
- health surveys
- quality of health care
- community psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- attitude of health personnel
- community mental health Services
- health surveys
- quality of health care
- community psychiatry
Introduction
Clergy have often been identified to act as frontline mental health workers and ‘gatekeepers’ to mental health services.1 In America, as many as 40% seek support from clergy for mental health concerns, with studies identifying that individuals with a mental health diagnoses were more likely to seek support from clergy alone, than psychiatrists and psychologists combined.2 3 Indeed, 15% of clergy time was found to be spent in pastoral counselling; however, despite this, referrals to mental health services in the USA are rarely made (in some cases as little as 10%).2 4
This discrepancy highlights the important question of ‘why is there a lack of communication between clergy and mental health services?’ numerous studies attempt to explain this lack of collaboration. First, Farrell and Goebert identified how 71% of clergy felt they did not have sufficient training to recognise a mental disorder; moreover, clergy have been shown to demonstrate both little knowledge and desire in learning about psychiatric skills and assessment, and the roles of a psychiatrist in the community.3 5 6
Second, the knowledge of psychiatrists in the roles of clergy in pastoral and mental healthcare is limited and that little training for psychiatrists in religion and spirituality is neither available nor willingly sought out.7–9 The insurance-based medical system in some countries such as the USA may also be a prohibitive factor in patients and clergy seeking additional, costly support. McMinn demonstrated how psychiatrists are often reluctant to refer patients to clergy.8 A UK study found that despite 93% of clergy referring at least one individual to a general practitioner (GP), and 67% to a community mental health team (CMHT), only 51% of clergy had received a referral from a GP and 38% from a CMHT.10 11 This is an important point to consider, as faith has been shown to be beneficial to mental health and coping strategies during times of ill health.12 Furthermore, it has important involvement in defining ‘a holistic approach taking account of physical, cultural, social, mental and spiritual needs’ in patient care, as outlined by the Department of Health 2009.13
Finally, a degree of mistrust has been observed between mental health professionals and clergy due to a lack of shared values.12 McRay et al showed how evangelical pastors often demonstrate an antipsychiatry way of thinking, and Leavey discussed how Pentecostal churches often believe mental illness should be ‘cured’ through spiritual means.5 6 Indeed, there are clear professional guidelines that prohibit proselytising from healthcare professionals in a position of power to their patients. In 2009, two nurses lost their jobs after offering prayer and spiritual advise to patients.12
In order to challenge these issues in collaboration, Oppenheimer highlighted six key themes which should be addressed: (1) recognition of clergy as frontline mental-health workers or gatekeepers to the mental-health system; (2) obstacles to collaboration; (3) the importance of shared values; (4) the need for more education or knowledge for the clergy and/or mental health professionals; (5) the benefits of collaboration to the professions, and (6) the role of clergy and mental-health workers in prevention.14 Examples of collaborative programmes implementing these themes exist within the National Health Service (NHS), including the ‘mental health working party’, which aims to provide mental health training for clergy. Furthermore, the Sheffield Health and Social Care NHS Foundation Trust have developed methods in promoting spirituality within mental health practice; however, despite this, clergy often desire a more collaborative relationship with mental health services.10
This study aimed to investigate the stance of clergy, GPs and psychiatrists in Wales on the above themes. A total of 124 clergy, 48 GPs and 13 psychiatrists in Wales were surveyed. Part 1 of the survey covered four main themes: demographic; types of mental health cases seen by clergy and medical professionals; referral rates between clergy and mental health services and attitudes and relationship between clergy and mental health services. Part 2 assessed clergy sensitivity in identifying and referring on mental health disorders by using seven virtual case vignettes. To our knowledge, only two other UK studies have sought to investigate the relationship between clergy and mental health services and hence due to the ever-changing nature of this relationship this topic is in need of review.10 11
Methods
Demographic
With regard to clergy, an online search for places of worship in Wales was conducted. A total of 891 Christian clergy were contacted via email (figure 1). A total of 124 participants responded (14% response rate). Sixty-five percent were male (32% female, 3% preferred not to answer), median age range was 51–60 years and median range of clerical experience was 11–20 years. A total of 99 considered themselves as ‘White British’, 4 ‘White European’, 3 ‘Irish’, 2 ‘Australian’ and 1 ‘Black African’. A total of 78 of the respondents reported themselves as Anglican, 9 Catholic, 8 Protestant, 5 Independent Evangelical, 1 Presbyterian, 1 Pentecostal and 7 ‘other’.

Participant demographic and inclusion criteria: 124 clergy, 48 GPs and 13 psychiatrists were included in the final analysis. GP, general practitioner; GMC,general medical council (GMC)
With regard to GPs and psychiatrists, all seven local Welsh health boards were contacted, and five distributed an online survey to all primary care and mental health services via email (figure 1). A total of 61 participants responded, 79% GPs and 21% psychiatrists. Thirty-nine percent were male (54% female), median age range was 51–60 years and median range of clinical experience was 21–30 years. A total of 45 considered themselves as ‘White British’, 2 ‘White European’ and 1 ‘Chinese’. A total of 29 were Secular, 24 Christian and 1 Buddhist.
Survey
A cross-sectional survey was conducted using a questionnaire based on Wood et al.10 Questionnaires were delivered via email to clergy and distributed via health board to GPs and psychiatrists. Questions aimed to cover four main themes: demographics; types of mental health cases seen by clergy and healthcare professionals; referral rates between clergy to mental health services and attitudes and relationship between clergy and mental health services. Questions on the ‘types of mental health cases seen by clergy and healthcare professionals’ and ‘referral rates between clergy and mental health services’ were rated on a four-point Likert scale: Never (0); Rarely (1); Sometimes (2); Frequently (3). Questions regarding ‘attitudes and relationships between clergy and mental health services’ were scored on a five-point Likert scale: strongly agree (1); slightly agree (2); neither disagree nor agree (3); slightly disagree (4); strongly disagree (5).15
Virtual cases
Seven virtual cases were designed based on common issues seen by clergy (online supplementary appendix A).10 Cases included: one case of mild depression; one case of severe depression with suicidal ideation; one case of generalised anxiety disorder; one case of obsessive-compulsive disorder (OCD) with religious themes; one case of delusions with religious themes; one case of delusions with non-religious themes; one case of substance abuse. For each case, clergy only were asked how likely: they would refer to mental health services or a GP; they would continue to manage and support the individual; they believed is due to a mental health condition; they believed is a spiritual problem. All responses were graded using a five-point Likert scale: very unlikely (1); somewhat unlikely (2); unsure (3); somewhat likely (4); very likely (5).15 A free text space was also provided for any additional comments clergy had on each case.
Supplemental material
Analysis
All data were anonymised and stored on an encrypted device. Questionnaire and virtual case data were logged into Statistical Package for the Social Sciences (SPSS) and analysed via qualitative and quantitative means. Linear regression models were used to analyse data comparing clergy and practitioner demographics to opinions of and experiences of collaborating with one another. A paired sample correlations test was used to analyse how often clergy see mental health issues against how often they refer on. P<0.05 was considered statistically significant. All data were tested for normal distribution. Free text responses were analysed via a textual analysis method. Free text was manually searched for comments on referrals, perceptions of mental illness and attitudes held by medical professionals and clergy in collaborating. Comments were then compiled into their respective categories and divided based on a positive or negative viewpoint.
Results
From the perspective of clergy…
Mental health issues seen and referral rates by clergy
American clergy have been identified to frequently interact with those with mental health issues, but rarely refer on.1 2 4 Hence, we sought to investigate how often clergy in Wales are approached by those with mental health issues and how often they refer on to mental health professionals (figure 1).
In figure 1, clergy were asked to rank on a four-point Likert scale how frequently they encounter individuals presenting to them with mental health issues and how often they refer these individuals onto mental health services, their GP or a mental health charity.
In our cohort, the most common issues seen by clergy included anxiety and depression, with only approximately 10% of clergy rarely or never encountering these issues. Substance misuse and religious themed OCD were also seen commonly by clergy. Suicidal ideation and delusions were seen least commonly, with 36% of clergy stating that they sometimes or frequently encountered these conditions—an important figure to not overlook.
With regard to referrals, depression, anxiety, substance misuse and suicidal ideation ranked as the most common conditions that clergy refer to medical professionals (on average, 72% of clergy stated they sometimes or frequently refer these conditions to medical professionals). Delusions and religious themed OCD were least commonly referred on by clergy (on average 42% of clergy stating that they sometimes or frequently refer on these conditions).
Overall, how often clergy saw mental health issues was significantly correlated with how often they made a referral (paired samples correlation (n=122; r=0.596; two-tailed sig p<0.001)), suggesting clergy who are not referring either are not encountering or are not recognising mental health issues in individuals seeking their help.
On average, clergy had sometimes or frequently seen and referred the above issues to a healthcare professional approximately 60% of the time.
Referral rates from medical professionals to clergy
Since faith and spirituality may be beneficial to mental well-being in some patients, we sought to investigate how often clergy receive referrals from healthcare professionals to provide pastoral care and social support.
On average, 80% of clergy had never received a referral from a healthcare professional, and only 7% stated they sometimes or frequently received referrals.
Ongoing support given by clergy
Having established that clergy are frequently approached by individuals with mental health concerns and that some do not refer onto a medical professional, we sought to investigate how often clergy provide ongoing support for an individual with mental health concerns.
Overall, 61% of clergy stated that they sometimes or frequently provide ongoing support for individuals with mental health issues, the most common being for anxiety and depression. However, on average, 39% of clergy stated that they never or rarely provide ongoing support for individuals with mental health issues.
Virtual cases
Clergy have often self-reported that they feel unprepared and undertrained to address mental health issues.16–20 Only half of clergy report some form of mental health training.17 We investigated how sensitive clergy are at identifying mental health conditions and how frequently they make appropriate referrals. To do this, we designed seven virtual mental health cases and asked clergy to rate on a five-point Likert scale how likely they believe the case is a mental health disorder and how likely they would refer to a medical professional. Cases included: one generalised anxiety disorder; one depression; one religious themed OCD, one schizophrenia with religious themes; one schizophrenia with non-religious themes; one substance misuse (alcoholism) and one suicidal ideation. All cases meet the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) diagnostic criteria for their respective condition, and thus a referral is warranted in each scenario.
Figure 2 shows how likely clergy believed virtual scenarios could be attributed to a mental health disorder and how likely they would refer each scenario onto a healthcare professional.
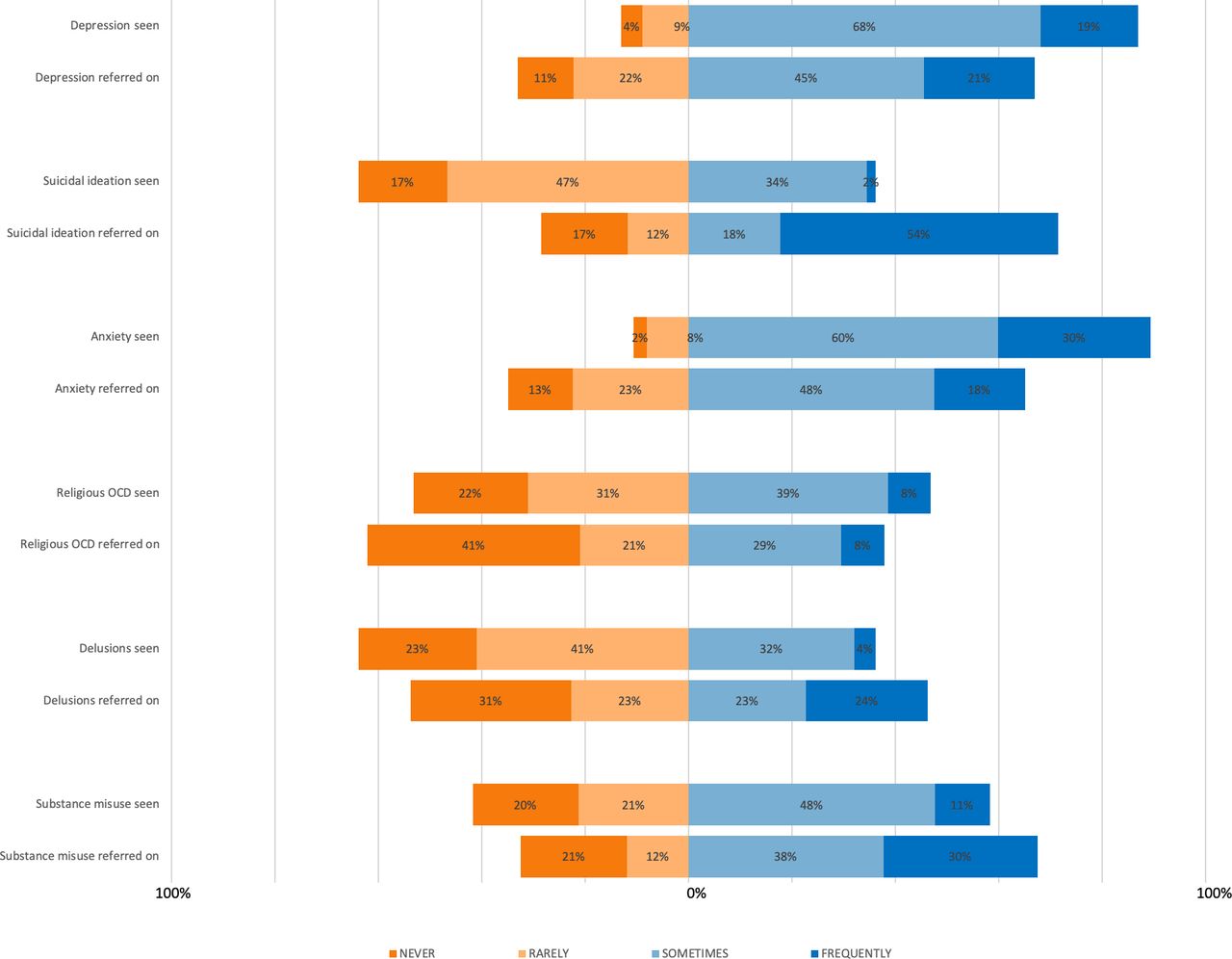
Clergy were asked how frequently they encounter individuals presenting to them with mental health issues and how often they refer these individuals onto a medical professional. OCD, obsessive-compulsive disorder.
Clergy appeared very effective at both identifying and referring on schizophrenia (religious and non-religious themed) and suicidal ideation. Clergy were also effective at referring on substance misuse; however, they were only moderately effective at identifying that this has a mental health disorder. With regard to depression, generalised anxiety and religious themed OCD scenarios, on average half of clergy were either ‘very unlikely’, ‘somewhat unlikely’ or ‘unsure’ whether they would attribute the scenario to a mental health condition and refer on. Overall, the more likely a member of clergy were to attribute the scenario to a mental health disorder, the more likely they were to refer onto a medical professional (paired correlates test, n=122; r=0.372, 2 tailed sig p<0.001).
When asked if they had any additional comments on the case, many respondents highlighted the need for an ‘urgent referral to a medical professional’ for the delusion (religious and non-religious), substance misuse and suicidal ideation cases. Furthermore, two respondents were able to recognise a number of red flag features in the suicidal ideation case, one stating: ‘planned and prepared for it. He's in a vulnerable risk group for suicide (age and sex)’. However, in the same scenario, another participant mentioned they ‘would not know what to do’. Despite all scenarios meeting a DSM-IV diagnostic criteria, many participants avoided referring the depression, religious themed OCD and generalised anxiety cases to a medical professional. These participants attributed these scenarios to social factors, such as ‘loneliness’ and being ‘overworked’ and wished to avoid labelling the scenario as a mental health problem. Hence, many stated they would ‘provide ongoing support’ and ‘try to establish the root cause of anxiety/low mood before referring to a GP’. Some stated they would ‘Only refer on to GP or other services if it persists or is hindering normal life’. A number of participants also stated they would encourage them to become part of the Church family and find support and comfort from that community before referring to a GP.
These findings therefore suggest that clergy are effective at identifying and referring on serious mental health issues, such as suicidal ideation, delusions and substance misuse. However, clergy appear less effective at identifying and referring on depression, anxiety and religious themed OCD. Although this may explain why some clergy do not refer onto healthcare professionals, clergyman attitudes and opinions are also likely an important contender.
Clergy opinions of mental health services
Mutual distrust and a lack of shared values have been previously identified as a potential explanation for the lack of referrals between clergy and mental health services.9 We therefore surveyed clergy on their opinions and experiences with mental health services, aiming to identify the source of any collaborative issues.
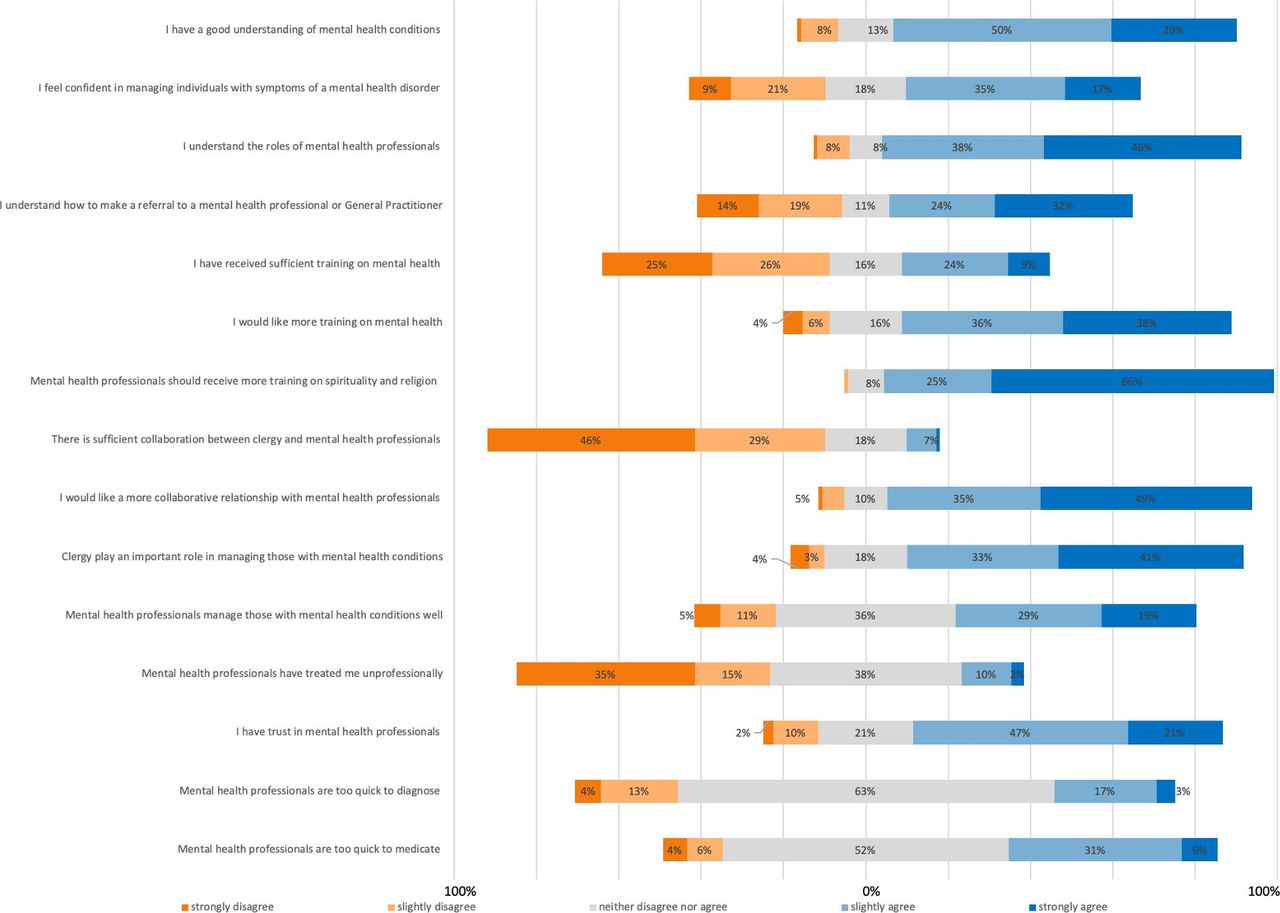
Figure 3 shows the opinions and experiences of clergy with mental health services and disorders. Generally, clergy who stated that they had a good understanding of mental health conditions were confident in managing mental health disorders, understood the roles of mental health professionals and understood how to make a referral to a GP. With regard to questions related to training, many clergy believed that they have not been offered sufficient training in mental health. Most clergy seemed in favour of receiving more training in mental health. Almost all clergy believed that mental health professionals should receive spirituality training. Clergy believed that there is currently insufficient collaboration between clergy and mental health services. Most clergy believed that they play an important role in managing mental health conditions and were in favour of forming a more collaborative relationship with mental health services.

How likely clergy believed virtual scenarios could be attributed to a mental health disorder, and how likely they would refer each scenario onto a healthcare professional. MH, mental health; OCD, obsessive-compulsive disorder.
Demographic subanalysis
Clergy demographics have often been seen to influence referral rates.21 22 Using a linear regression mode, referral rates were analysed for a statistically significant difference between clergy demographics. Gender, age, rural versus urban practice and denomination were used as covariates. No statistically significant difference was found between age, gender, urban versus rural practice and denomination (table 1A,B; F(4, 79)=0.924, p=0.454, R2=0.045). However, a trend was observed between denomination and clergy attitudes towards wanting more mental health training, in which Anglican participants were more in favour of receiving more mental health training when compared with other denominations.
Referral rates of clergy to practitioners versus clergy demographics (linear regression)
Referral rates of clergy to practitioners versus clergy demographics (model summary)
From the perspective of medical professionals…
Medical professionals have often been identified to rarely involve clergy in patient care.2 4 Indeed, in our cohort, 80% of clergy stated they had never received a referral from a medical professional. We therefore investigated how often GPs and psychiatrists reported that they refer mental health cases to clergy for community support.
Conditions seen and referred on to clergy by GPs and psychiatrists
Figure 4 shows how often GPs and psychiatrists encounter various mental health conditions in their practice, and how often they refer these cases to clergy for community support. Anxiety, depression, suicidal ideation and substance misuse ranked among the most frequent conditions seen by GPs and psychiatrists. In all cases, GPs and psychiatrists very rarely referred cases to clergy (on average 3% of GPs and psychiatrists stating ‘sometimes’ or ‘frequently’). Hence, combined with our findings from ‘Referral rates from medical professionals to clergy’, it is apparent that medical professionals rarely refer to clergy. In order to seek an explanation for this, we surveyed GPs and psychiatrists on their opinions in collaborating with clergy.

The opinions and experiences clergy hold of mental health services and mental health disorders.
Opinions of GPs and psychiatrists in collaborating with clergy
Medical professionals have often been found to hold negative views in collaborating with clergy in patient care, with many deeming this as inappropriate and showing little desire to expand their spiritual knowledge and hold a collaborative relationship with clergy.7–9 To better understand why referral rates to clergy are so low, we surveyed 48 GPs and 13 psychiatrists on their opinions in collaborating with clergy.
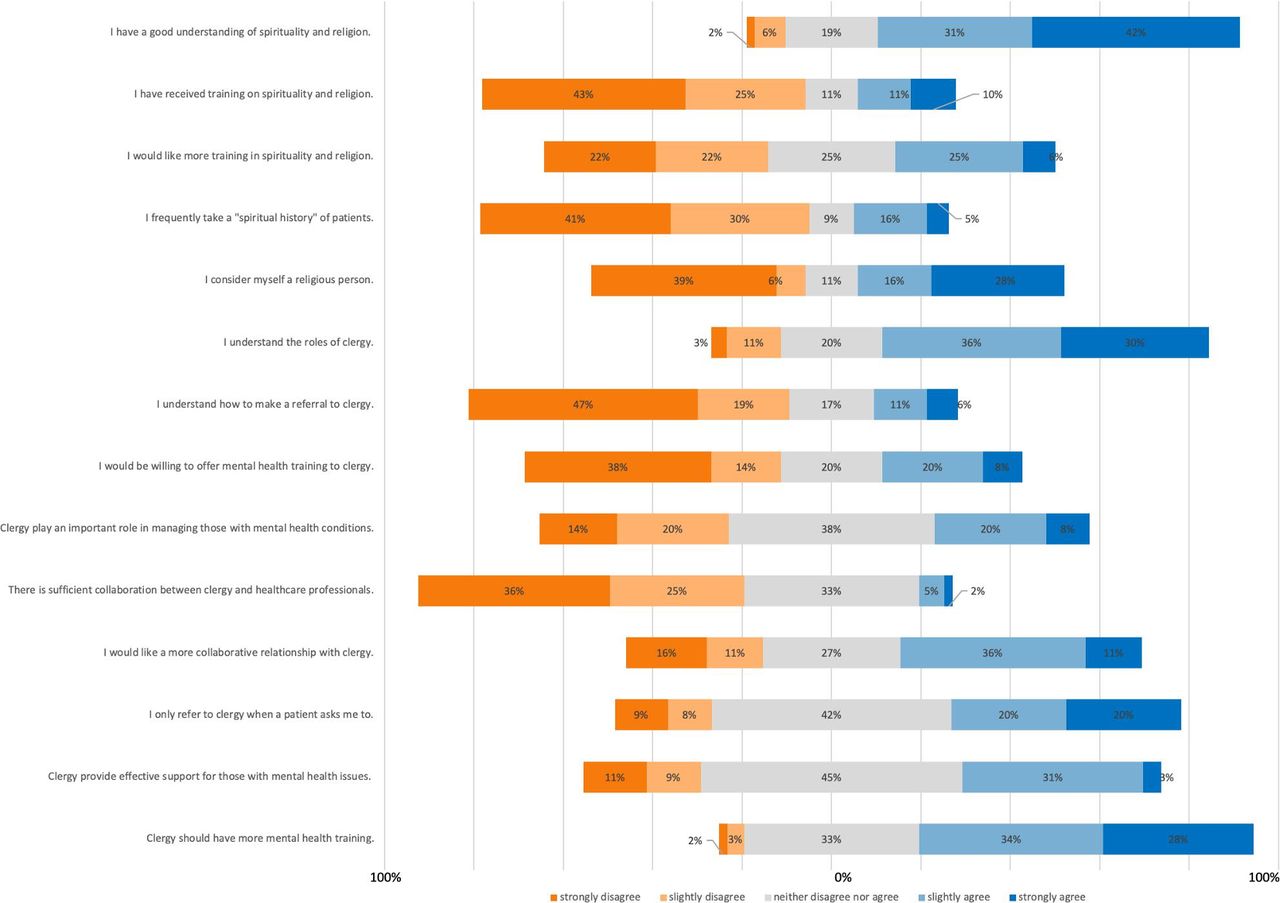
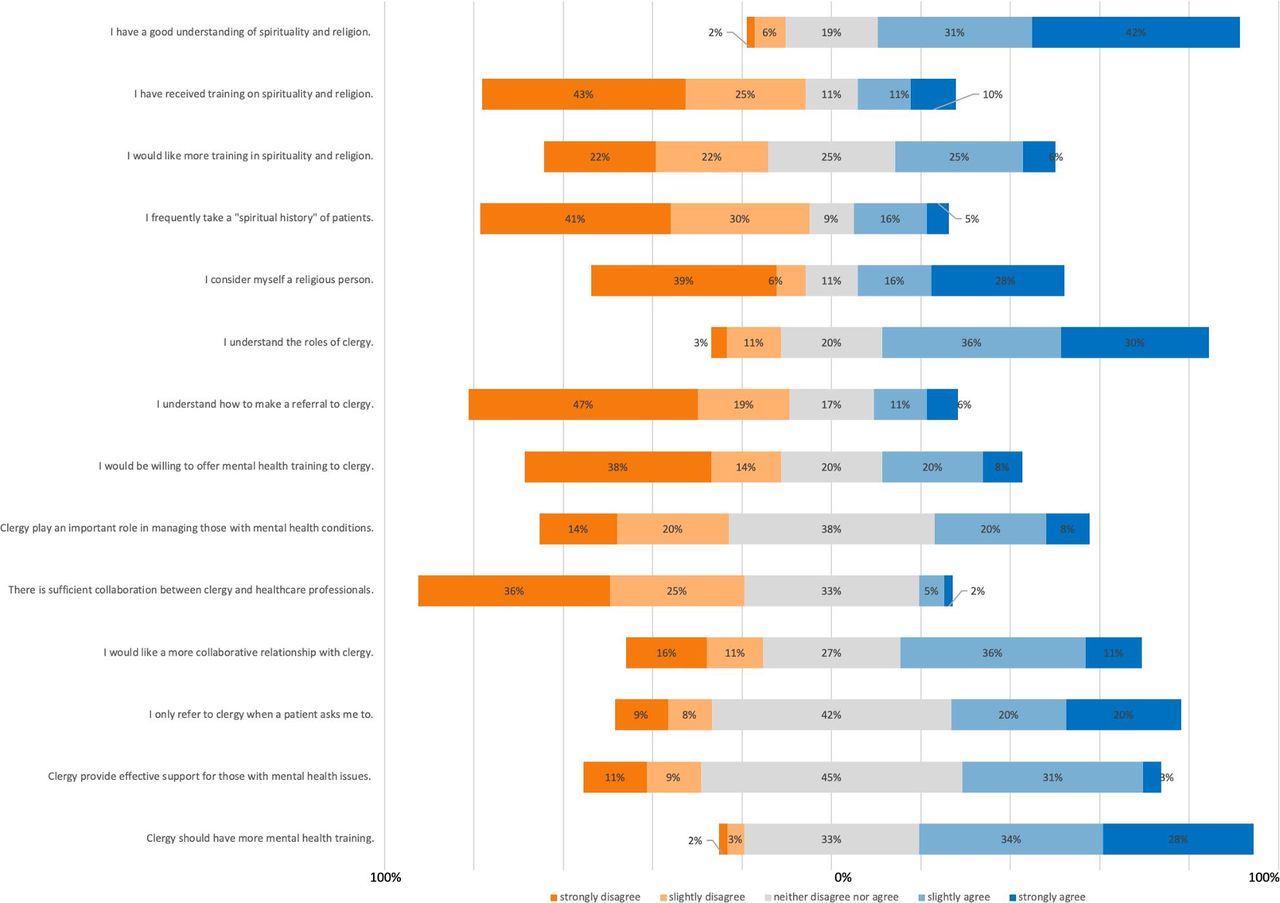
Figure 5 shows the opinions of GPs and psychiatrists of clergy, spirituality and religion. The majority of practitioners believed that they had a good understanding of spirituality and religion, and the roles of clergy in healthcare. However, most practitioners had received little training in spirituality and religion, and few regularly take a ‘spiritual history’. Sixty-one percent believed that there is insufficient collaboration between practitioners and clergy, and 47% were keen in improving this relationship. However, this said, only 31% would like more training in spirituality and religion. One-third of practitioners believed that clergy provide effective support and are important in managing those with mental health issues, and 62% believed it is important for clergy to have more mental health training, with 28% of practitioners stating that they would be willing to offer this training.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The opinions that GPs and psychiatrists hold of clergy, spirituality and religion. GP, general practitioner.
Overall, these results indicate that many GPs and psychiatrists recognise that there is insufficient collaboration between clergy and medical professionals and are keen to improve this. Most recognise the importance of training clergy; however, only one-third see them as a useful asset to community support.
Demographic subanalysis
In order to identify what groups, hold positive or negative views in collaborating with clergy, we performed a demographic subanalysis. Using a linear regression model, referral rates from practitioners to clergy were compared against practitioner demographics for statistical significance. Age, gender, religiosity, specialty and urban versus rural practice were used as covariates. Compared with GPs, psychiatrists were more likely to refer patients to clergy for community support (table 2A, table 2B; F(5, 48) F=4.05, p=0.004, R2=0.297). These results suggest that both psychiatrists and religious practitioners are more likely to hold positive views in collaborating with clergy, compared with GPs and non-religious practitioners.
Referral rates from practitioners to clergy versus practitioner demographics (linear regression)
Referral rates from practitioners to clergy versus practitioner demographics (linear regression)—model summary
Discussion
Main findings
In this study, we aimed to investigate the collaborative relationship between clergy and medical professionals. In our cohort, we found that clergy are frequently approached by those with mental health issues, especially with regard to anxiety and depression. Suicidal ideation was seen least commonly; however, 36% of clergy stated that they sometimes or frequently encountered individuals with suicidal ideation—an important figure to not overlook. This is a similar finding to Wood et al, who identified that depression and anxiety were among the most common issues encountered by clergy and suggested that this is due to them ranking as the most prevalent mental health problems in the UK (one in six adults).10 23 Similarly, since suicidal ideation ranks among the rarest mental health problems, clergy are less likely to encounter these issues.24 Interestingly, our cohort appeared to encounter more substance abuse cases compared with other city-based studies, an unusual finding as although commonly seen by clergy, South Wales has been shown to be below the national average in illicit drug-related hospital admissions.10 11 19 This said a large number of our clergy were based in rural areas, which have been shown to have higher rates of alcohol abuse compared with urban areas.25
With regard to referrals, around 60% of clergy commonly refer cases to mental health professionals, and nearly all clergy who encountered cases of suicidal ideation referred on. This is a similar finding to other UK studies, who found that around 80%–90% of clergy had referred to a healthcare professional at least once, in contrast to US clergy, where as little as 10% refer.4 10 11 However, this still leaves approximately 40% of clergy who rarely or never refer. It is therefore important to identify how often clergy provide ongoing support for individuals with mental health issues. In our cohort, around 70% of clergy provide regular support for those with mental health issues. This is not surprising, as clergy have been reported to spend much of their time offering pastoral care.2 Indeed, the importance of clergy as counsellors have been identified to be paramount in rural areas, due to the lack of community mental health services.26 However, studies have identified that US clergy may be insufficiently trained to provide effective pastoral counselling, especially with regard to depression.2 16–20 Furthermore, a US study found that 30% of mentally unwell Christian congregants who sought counsel from their church had experiences detrimental to their treatment, as a result of poor training in mental health counselling. These included abandonment and attributing mental illness to demonic activity and lack of faith.27
As clergy have been previously identified to lack skills and knowledge in psychiatric assessment and mental health, with 71% feeling as if they have not received sufficient training to recognise and manage a mental health disorder, we used virtual case scenarios to investigate how sensitive clergy were at identifying and referring on mental health disorders.28 We found that Clergy are effective at identifying and referring on serious mental health issues, such as suicidal ideation, delusions and substance misuse. However, clergy appear less effective at identifying and referring on depression, anxiety and religious themed OCD. This finding may suggest that since clergy feel more confident in managing common scenarios, such as depression and anxiety, they do not feel the need to refer the cases on. However, in cases such as suicidal ideation and psychosis, clergy are able to recognise their limitations and the danger of the situation and refer the case on, as identified by Mathews.21 Indeed, this may indicate that the ability of clergy to recognise and refer emotional distress and individuals who are a danger to themselves or others has dramatically improved since similar studies 30 years ago.29 Furthermore, a similar study used virtual cases to assess US Korean clergy on their conceptualisation and management of mental health disorders. They found that for scenarios such as depression almost all clergy conceptualised the problem as psychological and had no issues referring. However, for problems such as psychosis with religious delusions, half of clergy attributed this to a spiritual problem, and hence only 40% were willing to refer on.30 Interestingly, in our cohort, the religiosity content of the scenarios had no effect on how clergy conceptualised or referred cases. This could be because all of our cases were presented at the same time, and comparing one case of psychosis without religious themes to another with strong religious themes may have impacted on their assessment. Demographics may also influence clergy conceptualisation and referral patterns. Previous studies have identified that advanced theological education and a lower level of conservatism both have a positive effect on referral rates.21 In our cohort, only denomination showed a trend on the effect on clergy opinions of mental health services and referral rates, in which Anglicans appeared more willing to refer and collaborate with mental health services, as also seen by Wood et al.10 Therefore, the true answer to improve collaboration likely lied in understanding clergy opinion of mental health disorders and mental health services.14
We surveyed clergy opinions of mental health services. We found that most clergy believed mental health disorders could be explained with a more biological model over a spiritual model and seemed to respect mental health professionals, believing they managed conditions well. However, with regard to collaboration, clergy believed that they play an important role in managing those with mental health conditions and that there needs to be more collaboration between clergy and mental health services. Although most clergy believed they had a good understanding of mental health conditions and felt confident managing them, a large proportion did not understand how to make a GP referral and believed that they had not received sufficient training on mental health disorders and would like more. These findings support that of Van der Waal who conclude that pastors often favour biological explanations of mental illness and in many cases agree with the use of medications.19 Furthermore, they complement the notion that many clergy feel they need access to more mental health education and collaboration, and challenge the idea that many clergy hold antipsychiatry views of mental health disorders.6 10 19
Turning to the perspective of psychiatrists and GPs, we began by assessing referral rates from healthcare professionals to clergy for community support. In our cohort, both clergy and practitioners reported that referrals to clergy rarely occur (85% of clergy had never or rarely received a referral from a healthcare professional). This is consistent with a number of other studies, which in some cases, as much as 62% have never received a referral, despite evidence to support that prayer, spirituality and faith significantly improve physical and mental well-being and recovery.10–12 Many studies attribute this observation to the sceptical and ‘dismissive’ outlook of mental health professionals on clergy, which in turn can be explained by the lack of training healthcare professionals receive in spirituality and religion, preventing them from developing an appreciation for the value of clergy in supporting mental health disorders.5 7–9 Hence, we surveyed the opinions of GPs and psychiatrists in spirituality, religion and collaborating with clergy.
The majority of GPs and psychiatrists held positive views in collaborating with clergy and recognised that there is currently insufficient collaboration between medical professionals and clergy. One-third of practitioners were willing to rectify this by offering mental health training to clergy. This said, however, only a minority of practitioners recognised the usefulness in using clergy as a community support service for patients and were willing to receive training on spirituality and religion. This highlights how practitioners in our cohort generally favoured improving only a unidirectional flow of mental health referrals from clergy to practitioners. Indeed, several other UK studies have observed how practitioners generally hold positive views in collaborating with clergy, however rarely refer patients to clergy for medical issues, unless in the context of end of life care.31
Overall, our findings challenge that a number of studies who identified a degree of mutual distrust and antipsychiatry ways of thinking between clergy and mental health services and are consistent with Van der Waal and Wood et al, in that clergy are keen for more mental health collaboration and education.10 19 Indeed, a number of successful examples of collaboration exist, including training programmes for psychologists on collaboration with religious professionals and organisations.8 Two studies reported clergy and physicians spending mealtimes together and attending training courses improves relations and referrals.32 One scheme created a successful toll-free telephone number that pastors can call to receive free psychiatric advice, in addition to organising a number of mental health workshops on topics such as grief, conflict management and suicide prevention and developing a ‘crisis response manual’ for mental health emergencies.33 Much of these projects have received positive feedback, with programmes such as ‘clinical pastoral education’ training improving clergyman confidence and competence in dealing with mental health disorders.18
In conclusion, we have identified that clergy are frequently approached by those with mental health issues and that clergy appeared effective at recognising and referring on mental health conditions to a medical professional (especially when the patient was likely a risk to themselves or others). In contrast, referrals to clergy from medical practitioners rarely occurred. Hence, we surveyed clergy and medical professionals on their opinions in collaborating. Both clergy and medical professionals recognised that there is currently insufficient collaboration between the two services and both are keen to rectify this, with one-third of practitioners prepared to offer mental health training to clergy. This said however, only a minority of practitioners recognised clergy as a useful asset to community support for mental health patients, highlighting the preference of many practitioners for a unidirectional flow of referrals from clergy to medical professionals. Indeed, many practitioners deemed clergy as ‘inappropriate’ when planning patient community care, despite the proven health benefits of spirituality.12
Study limitations
When interpreting our results, it is important to consider our cohort only represents a minority population of the UK. We contacted 891 Christian clergy from seven different denominations across Wales with the aim of providing a holistic snapshot of clergy pastoral care and medical professional collaboration within NHS Wales alone; however, only 14% of clergy responded, a rate consistent with other similar studies.6 10 19 One possible explanation for the poor response rate was the length of the questionnaire, with participants taking on average 20 min to complete. Additionally, an online questionnaire was conducted and distributed via email; a large proportion of clergy and medical professionals could not be contacted as they had no available email address. Furthermore, 61% of clergy reported themselves as ‘Anglican’, a denomination that has been shown to be more open to collaborating with medical professionals.14 As seen by Wood et al who showed a 21.4% response rate, many of the churches we contacted responded stating they did not have a priest, and in some cases, clergy were ministers to multiple churches and so only gave one reply.10 Hence, our absolute response rate is likely higher. Nonetheless, these points highlight the challenge of obtaining a representative cohort. Our low response rate and findings of mutual positive views between services may indicate a degree of bias due to convenience sampling in this study. Despite correcting for religiosity in our statistical models, this could potentially skew our results to indicate a more positive attitudes in current and future collaboration between medical professionals and clergy. Telephone and in person interviews may provide an opportunity to reduce such bias in context of future research.
Implications
With regard to future practice, it is evident that clergy are in the privileged position of acting as ‘gatekeepers’ to mental health services and most seem willing to collaborate with mental health professionals. Here, we make four recommendations. First, we recommend establishing mental health first-aid and counselling workshops for clergy, and spirituality and religion workshops for healthcare professionals and medical students, in order to improve mutual understanding of one another’s roles and clinical mental health skills. Second, we recommend establishing an online or telephone referral service for clergy to mental health services, and vice versa, in order to provide an easy and accessible method in making referrals. Third, a listing of faith friendly practitioners and counsellors that clergy are able to work with and refer to may provide a more positive platform for mutual collaboration between services. Finally, we recommend organising gatherings for healthcare professionals and clergy, in order to improve interprofessional relationships. Notably, all three of these recommendations have been shown to be effective in improving collaboration.32 33
With regard to future research, we suggest conducting a similar survey and qualitative analysis of opinions held by Islamic, Jewish, Hindu, Sikh, Buddhist and Humanist clergy, in collaborating with medical professionals with regard to both mental health and medical patients. We also recommend conducting further investigation into the efficacy of mental health training for clergy, spiritual training for practitioners and clergy-practitioner referral pathways as methods to improve collaboration between the two services.
References
William Heseltine-Carp is a final year medical student with a keen interest in academic psychiatry at Cardiff University in the UK. He was recently awarded the Welsh Psychiatric Society Prize for his academic performance in psychiatry and frequently participates in psychiatric conferences, medical student teaching and clinical audits. His main research interests include early intervention strategies for anxiety and depression, identifying candidate markers for personalised psychiatric medicines, and investigating the frequency of undiagnosed mental illness in chronic disease patients.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was published. Corresponding author email has been updated.
Contributors WH-C conceptualised the idea, designed and conducted the survey and wrote the manuscript. MH supervised the project and edited the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data were anonymised and stored on an encrypted device. Questionnaire and virtual case data were logged into SPSS statistics. Data are available on request from the primary data collector and author. Contact -willhcarp@hotmail.co.uk, Cardiff university school of medicine. Both authors are willing for reuse of data, assuming appropriate recognition is given.