Article Text

Abstract
Pandemic, being unprecedented, leads to several mental health problems, especially among the front-line healthcare workers (HCW). Front-line HCWs often suffer from anxiety, depression, burnout, insomnia and stress-related disorders. This is mediated to a large extent by the biopsychological vulnerabilities of the individuals; socioenvironmental factors such as the risk of exposure to infection, effective risk communication to HCWs, availability of personal protective equipment, job-related stress, perceived stigma and psychological impact of the isolation/quarantine and interpersonal distancing also play the major roles. Despite the huge magnitude of mental health problems among the front-line HCWs, their psychological health is often overlooked. Some of the potential measures to reduce the mental health problems of the front-line HCWs are effective communication, tangible support from the administration/seniors, mental health problem screening—and interventional—facilities, making quarantine/isolation less restrictive and ensuring interpersonal communication through the various digital platforms, proactively curtailing the misinformation/rumour spread by the media and strict legal measures against violence/ill treatment with the HCWs, and so on. India, along with other countries who lately got affected by the COVID-19, must learn from the experiences of the other countries and also from the previous pandemics as to how to address the mental health needs of their front-line HCWs and ensure HCWs’ mental well-being, thereby improving their productivity. Current review attempts to highlight the mental health aspects of the pandemic on the front-line HCWs, discusses some of the contentious issues and provides future directions particularly concerning COVID-19 in the Indian context and other low-resource countries.
- mental health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Currently, the entire humanity worldwide is facing a severe healthcare crisis, that is, the unprecedented COVID-19 pandemic for the 21st-century population. In simpler words, a pandemic is defined as ‘an epidemic occurring worldwide, or over a very wide area, crossing international boundaries and usually affecting a large number of people’.1 However, it is not the first time that humanity is facing a pandemic. Over the last century, many pandemics such as Spanish flu, severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS), Ebola, swine flu, and so on have emerged and been tackled.2 Existing literature supports that pandemic, apart from causing mortality and physical morbidities, also leads to tremendous mental health problems (insomnia, anxiety, depression, stress-related disorders including post-traumatic stress disorders (PTSD)) in the sufferers as well as in the non-infected public.3–6
Front-line healthcare workers (HCW) are health workers who play a crucial role in providing care to infected persons. Working in such an unprecedented situation, usually beyond their capacities, and with a risk of contracting the infection, poses HCWs at an increased risk of mental health problems. Literature suggests a high prevalence of mental health problems among the front-line workers (such as burnout, insomnia, anxiety, depression, illness anxiety, PTSD, and so on) which is mediated by various biopsychosocial factors.3 7–9 Despite this, the mental health issues of the front-line HCWs and other health workers are often overlooked.3 8 10 11 It is often considered that such disasters are often dealt with by this group of population and hence they would be able to manage themselves well.
The COVID-19 is the latest entrant in the list of pandemics causing infection. Although mental health issues related to patients, especially those related to quarantine/isolation or social distancing,11–13 are increasingly recognised and efforts are being made to mitigate its psychological impact, literature on the psychological impact of pandemic (including COVID-19) on the front-line HCWs is still elusive.
India was also not immune to be affected by COVID-19 and to face COVID-19-related medicosocioeconomic challenges. Considering the low-resource setting on healthcare aspects in the country, various strategies had been employed such as lockdown, the curtailment of routine outpatient services, postponing of elective surgeries, rotational duty shifts in phases, and so on. Lessons learnt from the experiences of the countries getting affected earlier and the measures they have undertaken to ameliorate the psychological impact of the COVID-19 on the HCWs can serve as a guide for India (and other lately affected counties), in terms of the planning and implementing necessary measures to mitigate the medicopsychological impact of COVID-19 among the front-line workers.
The current paper is aimed to review the available literature on mental health aspects of the pandemic on the front-line HCWs, discusses some of the contentious issues and provides future directions particularly concerning COVID-19 in the Indian context and can apply to other developing nations with low-resource healthcare facilities.
Methodology
The literature was searched in the PubMed, Medline and Google Scholar databases with the following search terms: ‘epidemics’[MeSH Terms] OR ‘infection’ OR ‘outbreak/epidemic’ OR ‘severe acute respiratory syndrome’[MeSH Terms] OR ‘ebolavirus’[MeSH Terms] OR ‘middle east respiratory syndrome coronavirus’[MeSH Terms] OR ‘COVID19’ OR ‘h1n1/09’ NOT ‘acquired immunodeficiency syndrome’[MeSH Terms] NOT ‘hiv’[MeSH Terms])) AND ‘health care providers’ OR ‘health professionals/care’ OR ‘nurse’ OR ‘para medical workers’ OR ‘frontline health worker*’ AND ‘mental health’[MeSH Terms]) OR ‘stress, psychological’[MeSH Terms]) OR ‘anxiety’[MeSH Terms]) OR ‘fear’[MeSH Terms]) OR ‘depression’[MeSH Terms]) OR ‘insomnia/anxiety’ (online supplementary file 1).
Supplemental material
The inclusion criteria were: articles dealing with the pandemics as per the World Health Organization's (WHO’s) list, an article published in any language with full text available and directly dealing with the mental health aspects of the HCWs. Exclusion criteria include: dealing with HIV/AIDS or other non-pandemic conditions, and not directly dealing with the mental health aspects of the HCWs. Bibliographic search, and grey literature search by visiting the official website of the WHO, Centers for Disease Control and Prevention (CDC), National Health Commission, China; CDC USA; Ministry of Health and Family Welfare, Government of India (GoI) were also conducted. The literature search included all articles until 7 April 2020.
Results
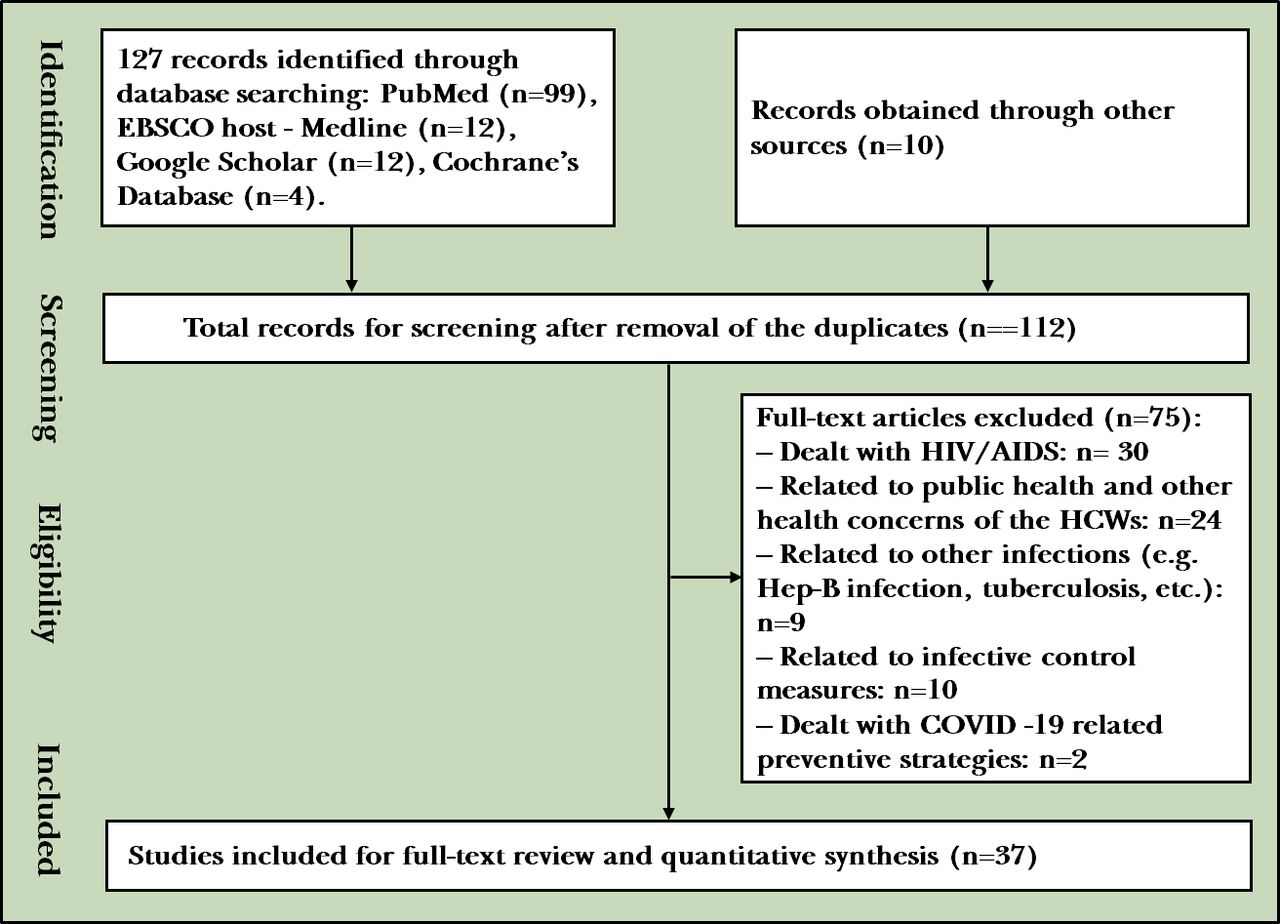
As the literature on COVID-19 is rapidly booming, a total of 127 articles were obtained until 7 April 2020. On data extraction, only 37 articles (including 10 articles obtained from the bibliographic search) were found to be eligible for inclusion in the review (process of study selection shown in figure 1). Most of the studies were related to SARS (16) followed by COVID-19 (10, including 3 Indian studies), influenza (4), MERS (3), Ebola (2) and psychological impact of quarantine and isolation (2). The majority of them were cross-sectional (24), out of which most were questionnaire survey-based (including online survey) (20) while some were interview-based (4, including 2 qualitative studies); however, two longitudinal studies were also available. The rest were viewpoints/commentaries (n=11). We could not find any review dealing specifically with the mental health aspects of the pandemic on the front-line HCWs.

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) figure depicting the process of study selection. HCW, healthcare worker.
The common mental health conditions assessed in the literature were: knowledge and attitude about the illness, coping strategy, and perceived health status (n=11), health distress (including burnout) (5), perceived stress and post-traumatic disorders (5), anxiety (5), depression (3), insomnia (3) and perceived stigma (4).
The sample size of the study varied based on the design and setting of the study. For instance, online survey-based studies had a relatively large sample size (varying from 333 to 1557) while hospital-based surveys were conducted on a sample size ranging from 148 to 333 (however, one study included 994 subjects). Comparative cross-sectional studies (30–40 subjects in each arm) and longitudinal studies were conducted (of 20 in each arm) with a relatively small sample size. As expected, the qualitative study was conducted with a sample size as low as 10.
The nurses were the most common population of the study followed by doctors. Interestingly, two studies also involved non-HCWs of the hospitals.
The magnitude of mental health problems in the HCWs
The literature revealed that a significant proportion of the HCWs during pandemic suffer from mental health problems including diagnosable mental health disorders (table 1). They are enumerated as follows.
Prevalence of mental health problems among the front-line healthcare workers during various pandemics
Emotional distress and burnout
A study from Canada reported that 36% of the HCWs facing the SARS epidemic experienced a high level of distress (measured by the Impact of Event Scale) with nurses having a higher rate than doctors.3 Another study conducted during the Ebola pandemic found that about two-thirds of HCWs suffered from the emotional exhaustion (Maslach Burnout Inventory).9 The latest studies conducted amidst COVID-19 reported that 62%–71% of the HCWs experienced some sort of distress (Physical Health Questionnaire-9, PHQ-9).8 Similarly, another study from Hubei (China) found the prevalence of depression among the front-line HCWs to be 50.4% (PHQ-9) with significantly higher rates in nurses, females and those working in the tertiary care setting.14
Anxiety disorders
The studies from China amidst COVID-19 have reported the prevalence of anxiety (both studies used Generalized Anxiety Disorder-7) among HCWs ranging from 44.6%14 to 62% (roughly 30% had a moderate or severe level of anxiety).8 A non-COVID study conducted in India during the swine flu has found that as high as 98.5% of the health professionals experienced the anxiety of mild type (Beck’s Anxiety Inventory)15 and another comparative study has reported significantly higher anxiety scores (Spielberger State-Trait Anxiety Inventory (STAI)) among the HCWs working in SARS unit than their non-SARS unit counterparts.16
Depression/depressive symptoms
Studies conducted during the SARS have reported a prevalence of the depression among the front-line HCWs to be 38.5% (vs 3.1% in non-front-line HCWs (Beck’s Depression Inventory))16 and 29%, respectively (General Health Questionnaire-12),5 with the latter study having found a higher prevalence among the nurses (45%) than the doctors. Studies that have evaluated stress and depression in HCWs after 1 year of the SARS epidemic had also revealed higher depression, anxiety and post-traumatic symptoms (ie, overall high degree of psychological distress).17 COVID-related studies had found high rates of depressive symptoms (as high as 50%) in HCWs.14 18
Insomnia
A comparative study from Taiwan reported that 37% of the HCWs working in the SARS unit suffered (vs 9.7% working in non-SARS unit) from insomnia (Pittsburgh Sleep Quality Index).16 The latest studies have reported the prevalence of insomnia (by Insomnia Severity Index) among the front-line HCWs to be around 35%–38%.8 14 18
Acute stress reactions and PTSD
Acute stress reactions and PTSD (early as well as late-onset) are common among the front-line HCWs. For instance, a study from China has found that the prevalence of the symptomatic PTSD (Davidson Trauma Scale) among nurses working in the SARS intensive care unit (ICU) and regular SARS unit was 33% and 29.5%, respectively (non-SARS unit nurses, 18.7%).16 A 1 year longitudinal study reported that HCWs who worked in the high-risk units (respiratory ward) experienced significantly higher PTSD symptoms (Impact of Event Scale-Revised, IES-R) than their colleagues working in the low-risk unit (general ward). It has been observed that the front-line HCWs’ stress score (Perceived Stress Scale-10 (PSS-10) score) correlated with their depression and anxiety score (Depression Anxiety Stress Scale).19 Similar reports of post-traumatic stress had been reported following the SARS pandemic among the Canadian HCWs 1 year after the SARS.17 The latest study from China reported that about one-third of the front-line workers experienced the least moderate grade of PTSD (IES-R) with the prevalence being significantly higher among the nurses (74.55) than the physicians (66.9).14
Other psychological problems
HCWs frequently suffer from other psychological issues such as health-related concerns (one-third of HCWs reported this),5 poorly perceived self-health,8 depersonalisation,9 low personal achievement9 and lack of control over their lives during the period of quarantine.10
Table 1 illustrates the mental health problems faced by the HCWs during previous pandemics and the available data related to the ongoing impact of COVID-19 on the mental health of HCWs.
Factors contributing to the mental health problems in the HCWs
Many biological, psychological and social/environmental factors and their interplay predispose an individual to an increased risk of mental health problems (table 1). They are enumerated as follows.
Biological factors
History of mood disorder and earlier age (vs later age) have been identified to predispose the HCWs for an increased risk of mental health problems during the period of pandemic.16 This is also mediated by socioenvironmental factors such as having a child3 5 or a sick elderly in the family, whom they have to additionally care for while delivering duties as HCWs during the pandemic.
Psychological factors
Literature suggests that the personality traits of the HCWs are one of the important determinants for the development of mental health issues during the pandemic situation. For instance, a study conducted during SARS pandemic on HCWs found that the individuals having anxious avoidant personality traits, fear of scrutiny and avoidant coping mechanism3 were at higher risk of mental health stress, supported by several other studies.3 20–22 Further, HCWs indulged in the emotion-focused coping strategies suffer from higher emotional exhaustion, stress, anxiety, depression and PTSDs.23 24
Similarly, HCWs suffering from role conflict (between the professional and familial role)24 25 and getting caught into potential moral injury exposure (defined as profound psychological distress which results from actions, or the lack of them, which violate one’s moral or ethical code26) have a higher rate of mental stress and mental disorders.27 More so, having a sense of unworthiness or being non-essential (among non-front-line HCWs)10 25 and resorting to denial (defence mechanism) towards the current psychological impact of an outbreak result in heightened risk of persistent stress and PTSD symptoms.19
On the contrary, personality traits such as hardiness (commitment, belief of having things under control, accepting a challenge, and considering it a chance to self-develop) directly mediate the positive mental health amidst an outbreak and also indirectly benefit the HCWs by decreasing their level of stress.28 Similarly, vigour (defined as high levels of energy, mental resilience, stamina and persistence when problems arise)29 is associated with a lower score on emotional exhaustion among the nurses during the SARS pandemic and also associated with a positive attitude towards the work and better organisational functioning.22 Further, altruistic acceptance of the work-related risk of contracting infection among the HCWs during the SARS pandemic was found to be negatively correlated with the long-term PTSD symptoms.
Literature also suggests that those involved in reflective practices (Aguilera model: self-awareness, problem sensing, and structuring, generating an answer, and evaluating it30) experience lesser mental distress,3 31 32 and develop problem-focused coping. Similarly, problem-focused coping strategy among the HCWs during the pandemic has been reported to decrease their mental stress16 and alleviated their fear,33 thereby decreasing the mental health problems.
Socioenvironmental factors
Inadequate communication and lack of information
Lack of proper communication from the higher authorities to the front-line HCWs and rapidly changing guidelines regarding infection control measures could lead to uncertainty, apprehension, lack of knowledge and a sense of uncontrollability over the situation. These act as important mediators for the development of mental health problems among the HCWs. Misinformation/rumour (often labelled as ‘misinfodemic’) prevalent during the pandemic, if not adequately clarified by the administration, adds to mental health stress among the HCWs.4 22 25 34
Risk of exposure to infection
The HCWs working in the high-risk area (screening out patient department(OPD), inpatient and ICUs) are at a higher risk of exposure to infection.5 12 28 35 A study from Wuhan (China) reports that as high as 87.5% of HCWs got infected from COVID-19.7 Such a high risk of exposure to infection gives rise to fear, apprehension and stress among the HCWs, which often get compounded by the fear of being a contagion for their family members and loved ones, resulting in significant mental health problems. Further, exposure to end-stage resuscitative procedures to save the lives of the patients including their colleagues could lead to PTSD.3 16 19
Social distancing
Avoiding interpersonal contact/communication (social distancing) is considered as an important measure to tackle the infective outbreak, greatly practised in the ongoing COVID-19.3 5 16 36 As a result, HCWs are mandated to maintain distance from their colleagues, both at the workplace and outside, which deprives them of otherwise much-needed social support. Further, maintaining social distancing from their family members (including sharing beds with one’s partner) results in lack of emotional support from the significant others and adds to emotional stress and mental health problems.3 10 22
Job stress/occupational stress
The HCWs contracting infections results in gross understaffing at the healthcare institutes.3 32 33 Such a situation poses the HCWs to work with limited resources, long working hours and frequently changing duties, and to work in an unfamiliar environment that, also with the new teammates, results in huge mental stress. This gets compounded by the unprecedented needs of quarantine/isolation and strict maintenance of interpersonal distancing. Western literature suggests that HCWs are often bound by the provincial order not to work at multiple places during pandemic resulting in financial difficulties.3 4 Further, front-line HCWs often are unable to impersonalise oneself while taking care for their infected colleagues and feel helpless for not being able to avert the mortality of their colleagues; senior physicians have also reported déjà vu experience and flashbacks (of their colleagues getting died) during pandemic.25
Personal protective equipment-related issues
It is not uncommon that front-line HCWs have to work with a limited supply of personal protective equipment (PPE).3 5 25 Such a scenario leads to fear and apprehension among the HCWs. The situation is often compounded by unclarity regarding which PPEs are adequate in a particular setting (screening OPD, low-risk wards, high-risk wards, ICUs, and so on) leading to confusion and worries. On the other hand, working under the restriction of PPEs (particularly mask) has also been reported to be a major cause of distress among the HCWs. Literature suggests that PPE comes as a major hindrance to properly communicate with the patient and one’s colleagues; moreover, working long hours with the PPEs also leads to significant burnout.5 31
Stigma
Perceived stigma among the HCWs has been reported to be a major mediator for psychiatric problems during the period of the pandemic. Studies conducted during SARS/MERS found that the prevalence of significant perceived stigma among the HCWs ranged from 20% to 50%.28 35 37 Literature suggests that perceived stigma is correlated with the stress (scores of PSS-10), mental health score (and 36-Item Short Form Survey),28 burnout25 and PTSD score.3
Isolation/quarantine
Isolation/quarantine is an important measure to curtail the infection amidst the pandemic.36 Front-line HCWs often have to work in the isolated wards where they happen to be the sole care providers for the patients.4 In the absence of much required interpersonal communication and social support, HCWs suffer the burnout and also experience the lack of self-control. Additionally, front-line HCWs often have to stay in quarantine (if suspected of exposure to infection) or in isolation (if contracted the infection) which deprive them of much-needed social support from their hospital colleagues and family members resulting in many psychiatric problems.9 10 12
Lack of support from organisation and colleagues
Literature suggests that HCWs often suffer from job-related insecurities, especially those who are asked to stay at home.5 The former may have a perception of being non-essential for the institute. Further, HCWs (especially nursing staff and other paramedical staff) may feel that they are lacking the necessary skills to tackle such a novel infection25; they often have fear of being scrutinised by their superiors and might be blamed for any error; they also feel the necessity of hand-holding and role-modelling by their seniors at the workplace.3 10 Further, HCWs need support from their administration concerning their family matters, finances, incentives and recognition for their efforts.33
Moreover, mental health issues of the HCWs during such a crisis are often overlooked. The much required periodic screening for any mental health problems usually is elusive. And usually, there is no provision of mental health services for them to seek help from.11 It is not uncommon for the HCWs to access resource material or seek online/telephonic counselling to allay their mental health problems.7 8
Role conflict
The available literature suggests that many a time HCWs suffer from a role conflict (between their role as health professionals and the role as a parent or family personnel). They frequently fear or remain apprehensive of being a contagion for their family members.3 25 Literature suggests that front-line HCWs having children report higher rates of anxiety, depression and distress. This may lead to avoidant coping strategies and absenteeism at the workplace, which adversely affect an organisation’s performance.10 27
Crowd behaviour
Literature suggests that pandemic caused by a novel agent that has no definite cure could lead to widespread anxiety/panic. This is often amplified by the misinformation/rumour circulated in the social media leading to a panic situation in the community—‘panicdemic’.6 In such a scenario, often ‘emotions go viral’ in the society which could lead to mental stress in an individual including the HCWs (emotional contagion). It can also heighten stigma towards the HCWs,38 resulting in increased mental health stress among the HCWs.
Misinformation
It is not uncommon that during the pandemic, especially during the early part of it, many misinformation and rumour are circulated in the social media, and so on.39 For instance, the limited number of PPEs, which leads to apprehension and fear among the HCWs; flaws in the PPEs being used; and any infection contracted by HCWs are highlighted disproportionately.3 34 This leads to mental health stress and exacerbates anxiety, depression and distress among the HCWs.6
Potential measures to address the mental health needs of the front-line HCWs
Effective risk communication to the HCWs
During the pandemic, especially during the early part, HCWs often suffer from uncertainties and fear, which become prominent if the risk is not effectively communicated (including measures to be taken to avoid infection) to the front-line HCWs by the higher authorities.3 5 Authorities/team leaders, by sharing succinct messages and authentic information, and regularly interacting (through the real or virtual platform) with their HCWs, could allay uncertainties and fear among the HCWs and bring about a sense of trust.
Involving mental health professionals in the core leadership
Having the mental health professionals (MHP) on board would ensure that the mental health issues of the HCWs are not getting overlooked.8 11 40 Some of the important steps to ameliorate mental health problems among the HCWs include regular screening for the mental health problems, normalising the psychological response to stress, having reflective approach towards one’s emotion and cognition, peer training in identifying burnout and delivering informal counselling, psychologically oriented meetings among the HCWs and the team leaders, and ensuring availability and accessibility of professional mental health services available and accessible for the HCWs.
Tangible support to HCWs from the leadership including regular communication
During pandemic, front-line HCWs often experience a sense of mistrust and helplessness. It can adversely affect their attitude towards work and lead to stress, thereby deteriorating the organisation’s performance.3 32 For instance, doubt regarding the efficacy of the right kinds of the PPEs to be used if properly clarified by a senior colleague/doctor, which may include seniors wearing the same PPEs (role-modelling) and working with them, could allay fear, anxiety and stress among the HCWs. Tangible support to the HCWs such as listening to their grievances, making the working environment conducive for working (eg, establishing a bathroom in the hospital premise, where an HCW can take a bath before leaving for their home, could significantly reduce the fear of being a contagion for their family members) and extending support related to the finances and specific family needs can bring about a sense of trust and self-efficacy among the HCWs.
Mental health support and services to the HCWs
Making availability of the mental health resource materials (including webinars); training in stress management (at the workplace or home) and problem-solving; arranging for confidential telephonic calls/online counselling or consultation with the mental health expert3 8; and arranging for a visit to a mental health expert could, to a large extent, reduce the mental health problems among the front-line HCWs. Amidst COVID-19, some of these steps have been taken by various international and national agencies.41–43
Involving HCWs in developing strategies
Literature suggests that involving HCWs (front-line and so-called non-essential HCWs) in planning and strategising for the pandemic can pay huge dividends. Apart from being clinically effective in fighting against the pandemic, it could also help in boosting the self-esteem of the HCWs (front-line and non-essential), and make them feel to be the part of the team, build their trust and promote a positive outlook about the work. Further, it results in decreased job-related stress, uncertainties, fear, anxiety and depression among the HCWs.10 32
Mitigate the psychological impact of the isolation/quarantine
HCWs and their contacts (colleagues and family members) often have to undergo quarantine or isolation during the pandemic. This may give rise to a sense of guilt for being a contagion for others, and also a sense of self-blame for causing understaffing at the workplace and adding to the workload of their colleagues. Further, isolation and quarantine also lead to severe restriction in one’s activities which often leads to worries and stress related to not being able to perform one’s professional and familial duties.4 9 10
By making quarantine/isolation less restrictive, arranging for telephonic/digital communication between the HCWs and their colleagues or family members, and through minor gestures (for instance, making a pizza available for a person in quarantine/isolation has been shown to decrease the mental health stress arisen during isolation3), psychological impact of the quarantine/isolation can be mitigated.
Ensuring availability of PPEs including developing less restrictive PPEs
Ensuring availability of the PPEs for the HCWs reduces the chances to get exposed to infection during patient care, and boosts their confidence to work without any fear, especially when many rumours centre around the unavailability of PPEs and its ineffectiveness circulates in the media.5 25
On the other hand, PPEs also act as the major hindrance for HCWs during caring for their patient. Acting as a barrier, it limits the interpersonal communication among the HCWs and the patients.3 5 It also leads to burnout, fatigue and job-related stress among the HCWs. Hence, innovations should be made to design less restrictive, flexible and easily wearable and removable PPEs.
Better information and e-resource system
A public health information system that is authentic and updated with wide dissemination could significantly reduce the psychological impact of misinformation/rumour on the mental health of the HCWs and the public.6 39 Fake news has shown to be associated with violence against HCWs or being ill treated. During isolation or social distancing, the internet serves as the major platform through which important information and resource materials (textual, audio, video) can be accessed, which can help in attaining and maintaining positive mental health .7 11 44 Lately, many international and national agencies including academic institutes have taken steps to generate e-resources for skill development among the HCWs and also addressing their mental health needs.
Implications in the context of COVID-19 from Indian perspectives
Although India (along with some of the South Asian, African and American countries) got affected by COVID-19 relatively late as compared with the Western Pacific and European countries,45 the spread of the COVID-19 has been rampant. As of 22 April 2020, more than 20, 000 confirmed cases and 559 deaths have been reported from the country.46 Like the global trend, a sizeable proportion of the front-line HCWs have also fallen prey to the COVID-19. To curtail the spread of the infection, the government was prompt to put in place surveillance across the national transit points and has implemented strictest measures including a nationwide complete lockdown (already spanned to 4 weeks) and mandatory social distancing. Consequently, uncertainties, movement restriction, difficulty in procuring the essential stuff and accessing other essential services (eg, transport, health services, and so on) are prevalent across the nation. This situation is compounded by the rounds of misinformation/rumour across the social media resulting in the stigma against the HCWs, and incidents of violence and ill treatment against them.47 48 Concerns regarding the availability of PPEs, course of the pandemic and isolation/quarantine are adversely affecting the mental health of the HCWs.
A few pieces of literature from India have have highlighted the impact on mental health of COVID-19.13 34 49 50 Governments (central and state) have also taken some of the noteworthy steps to mitigate the psychological impact of the COVID-19 among the patients, general public and HCWs, such as legal measures to prevent violence against or ill treatment with the HCWs. Similarly, safety and risk cover for the front-line HCWs are being ensured by the government, making the PPEs available and the insurance of a sum of 5 million rupees (Indian national rupees), respectively.51 But the ground-level implementation and the extent to which it allays the fear, anxiety and stress among the HCWs are yet to be evaluated.
Steps that need to be taken to avoid the spread of myths and rumours related to COVID-19 (such as drinking cow’s urine, taking alcohol cures COVID-19, using turmeric can boost immunity, non-vegetarian food consumption (meat) can lead to infection, and so on) and correcting the misinformation along with widely disseminating the correct information to the public are of paramount importance, otherwise all these would add to the pre-existing anxiety related to COVID-19 in the general public. Further, there should be some regulations on the news agencies also, along with some fixed protocol of reporting the news related to COVID-19, including the number of cases and deaths, to avoid any panic reactions among the public. More of the motivational and morale-boosting programmes of the public and HCWs should be undertaken actively to allay their anxiety. The government should take proactive measures to take full responsibility for the HCWs and their family members given any untoward incident related to COVID-19. In some states, the local authorities had declared monetary benefits and advanced monthly salaries to the HCWs (state of Haryana, and so on). All these boost the morale of the HCWs and they do not feel neglected by the government.
Similarly, proactive steps have been taken by the GoI in risk communication to the public/HCWs (through advertisement, online information portals and smart applications (Aarogya Setu Mobile App52)). Additionally, government and academic institutes have tried to address the mental health needs of the patients and the public by releasing the resource materials, conducting webinars and setting up help-line numbers; however, specific measures that address the mental health needs of the front-line workers are relatively scarce.
Learning from the experiences of the other countries and based on the findings of the available literature, some of the recommended measures to mitigate the psychological impact of COVID-19 among the HCWs are as follows: ensuring responsible media reporting and bringing about an attitudinal change among the public towards the HCWs; provision of screening for the mental health disorders, assessing the mental health needs, and institute-level mental health support and services for the front-line HCWs; researching the magnitude of mental health problems; and involving MHPs in the planning and implementation of the policies, and proactive role and leadership on part of the MHPs.
Conclusions
The current review was aimed to highlight the psychological impact of the pandemic on the front-line HCWs. The magnitude of mental health problems among the HCWs is huge; some of the common conditions are burnout, anxiety, depression, stress-related disorders, and so on. It is mediated by various biological, psychological and socioenvironmental factors. Lack of the effective communications, tangible support from the higher authority, misinformation, unavailability of PPEs, stigma and job-related stress are some of the major contributory factors for the development of the mental health problems among the HCWs.
Learning lessons from the previous pandemics and from the other countries that have successfully tackled COVID-19 and acting by it could mitigate the psychological impact of COVID-19 among the HCWs to a great extent. More research, especially from low and middle-income countries such as India, is required to design interventions tailored towards the need of the HCWs.
Acknowledgments
The authors are grateful to Dr Omkar Awadhiya, senior resident, Department of Internal Medicine, All India Institute of Medical Sciences (AIIMS), Bhopal, for providing some of the important insights about the mental health issues of the front-line HCWs during the COVID-19 service delivery.
References
Dr Snehil Gupta obtained his MBBS degree from Veer Surendra Sai Medical College and Hospital, Burla, Sambalpur (Odisha), India in 2012. He got training in psychiatry (M.D.) from the premier institute of the country at All India Institute of Medical Sciences (AIIMS), Delhi in India. After completing his MD in psychiatry, he worked as a senior resident (three years teaching programme) in the same institute till September 2019. He is currently serving (since October 2019) as the Assistant Professor, at the Department of Psychiatry at AIIMS, Bhopal (Madhya Pradesh) in India. He heads the common mental disorders (CMD) clinic of the Department of Psychiatry, AIIMS Bhopal. His main research interests include common mental disorders (CMD), women mental health, yoga and mental health, and public mental health.

Footnotes
Contributors SG drafted the manuscript and SS critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.