Article Text

Abstract
Background The mental health of current medical students is predictive of their mental health as future doctors. The prevalence of anxiety, depression and burnout is high among medical students, but less is known about the occurrence of other mental ill-health symptoms, such as eating or personality disorders, and factors contributing to mental ill-health.
Aims (1) To explore the prevalence of various mental ill-health symptoms in medical students and (2) to investigate what medical school factors and students’ attitudes contribute to these mental ill-health symptoms.
Methods Between November 2020 and May 2021, medical students from nine geographically spread medical schools in the UK participated by completing online questionnaires at two points in time, approximately 3 months apart.
Results Of the 792 participants who filled in the questionnaire at baseline, over half experienced medium to high somatic symptoms (50.8%; 402) and drank alcohol at hazardous levels (62.4%; 494). Adjusted longitudinal data analysis of 407 students who completed the follow-up questionnaire demonstrated that less supportive educational climates that were more competitive and less centralised around the students, lower feelings of belongingness, greater stigma towards mental ill-health and lower intentions to seek help for mental ill-health, all contributed to students’ mental ill-health symptoms.
Conclusions Medical students experience a high prevalence of various mental ill-health symptoms. This study suggests that medical school factors and students’ attitudes towards mental ill-health are significantly associated with students’ mental health.
- mental health
- prevalence
- anxiety
- attitude to health
- surveys and questionnaires
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Many medical students experience higher rates of stress-induced symptoms such as burnout and depression compared with non-medical students, which might indicate that medical schools’ approach to preparing future doctors has a negative impact on students.
WHAT THIS STUDY ADDS
This study explored various mental ill-health symptoms among medical students and found a high prevalence of symptoms such as anorexic tendencies, somatic and obsessive-compulsive symptoms and hazardous drinking.
The study also revealed that medical school factors (educational climate and sense of belonging) and students’ attitudes (stigma towards mental ill-health and help-seeking intentions) were associated with their mental ill-health symptoms.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A preventative approach that safeguards learning environments and addresses negative attitudes towards mental ill-health is crucial during medical school training.
Introduction
The mental health of medical students, our future doctors, is of primary importance as the mental ill-health of doctors has wide-ranging workforce consequences, including presenteeism (working while sick), absenteeism and workforce retention issues.1 Furthermore, doctors’ poor mental health links to reduced quality of patient care and an increased frequency of medical errors.2–4 Research suggests that students’ perceived stress and mental ill-health during medical school are related to their mental health later in their careers as trainees and fully qualified physicians.5 6 Thus, early intervention supporting the mental health of medical students is essential to prevent and improve doctors’ mental ill-health as it could potentially avert more complex issues later in their careers.
Furthermore, medical students are a unique group, as illustrated by a recent meta-analysis of depression and anxiety among college students, which included 64 studies and over 100 000 students. Results showed that medical students had significantly higher rates of both depression (39.4% vs 33.6%) and anxiety (47.1% vs 39%) compared with non-medical students.7 Understanding why medical students are more prone to mental ill-health symptoms is essential to institute appropriate health policies and interventions.
There is some indication that attitudes formed during medical school link to students’ well-being. Studies have revealed that despite suffering, medical students are reluctant to admit any difficulties to others openly; stigma towards mental illness and fear of repercussions due to a mental health-related diagnosis act as powerful deterrents towards help-seeking.8–12 Furthermore, medical school factors such as workload, lack of support and competitiveness link to burnout, reduction in empathy and career regrets.13–16 Although there are indications that various factors may play an important role in students’ mental ill-health individually, it is unclear what role these factors play when occurring together and if this role is similar for different types of mental health issues.
Researchers have also called for holistic multisite prospective longitudinal studies to identify factors associated with poor mental health among students.17 18 Building on existing research, this study is longitudinal and includes multiple UK medical schools. Moreover, previous research into the mental ill-health of medical students has concentrated on depression, anxiety and burnout,19–21 with less being known about other mental health conditions; investigating symptom prevalence will highlight which mental health issues might need to be prioritised through mental health interventions.
Objectives
The two objectives of this study are as follows: (1) to explore the prevalence of various mental ill-health symptoms in medical students and (2) to investigate what medical school factors and students’ attitudes contribute to these mental ill-health symptoms.
Methods
Study design
This is a longitudinal cohort study including a baseline (T0) and 3-month follow-up (T1); the study is presented following Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Study settings
A volunteer sample of medical students from nine geographically spread medical schools in the UK completed a web-based survey between November 2020 and February 2021. Medical schools originated from the following regions in England: London, North East and Cumbria, North West, South West, West Midlands and countries included in the UK (ie, Scotland, Northern Ireland, Wales). At the start of the survey, participants provided their email addresses when completing their consent forms on a secure platform—RedCap in the UCL Data Safe Haven. We used these email addresses to send follow-up invitations to participants. After completing the informed consent form, participants were redirected to another online platform, Online Surveys, to complete the survey to reassure students that their responses were completely anonymous and encourage open and honest answers. This step meant we could not match participants’ names or email addresses to their survey responses. Participants were asked to create a personalised code at the start of the survey, which allowed us to match their responses from T0 to T1. Those who took part at T0 were invited to complete the questionnaire again 3 months later (T1; February−May 2021).
Participants
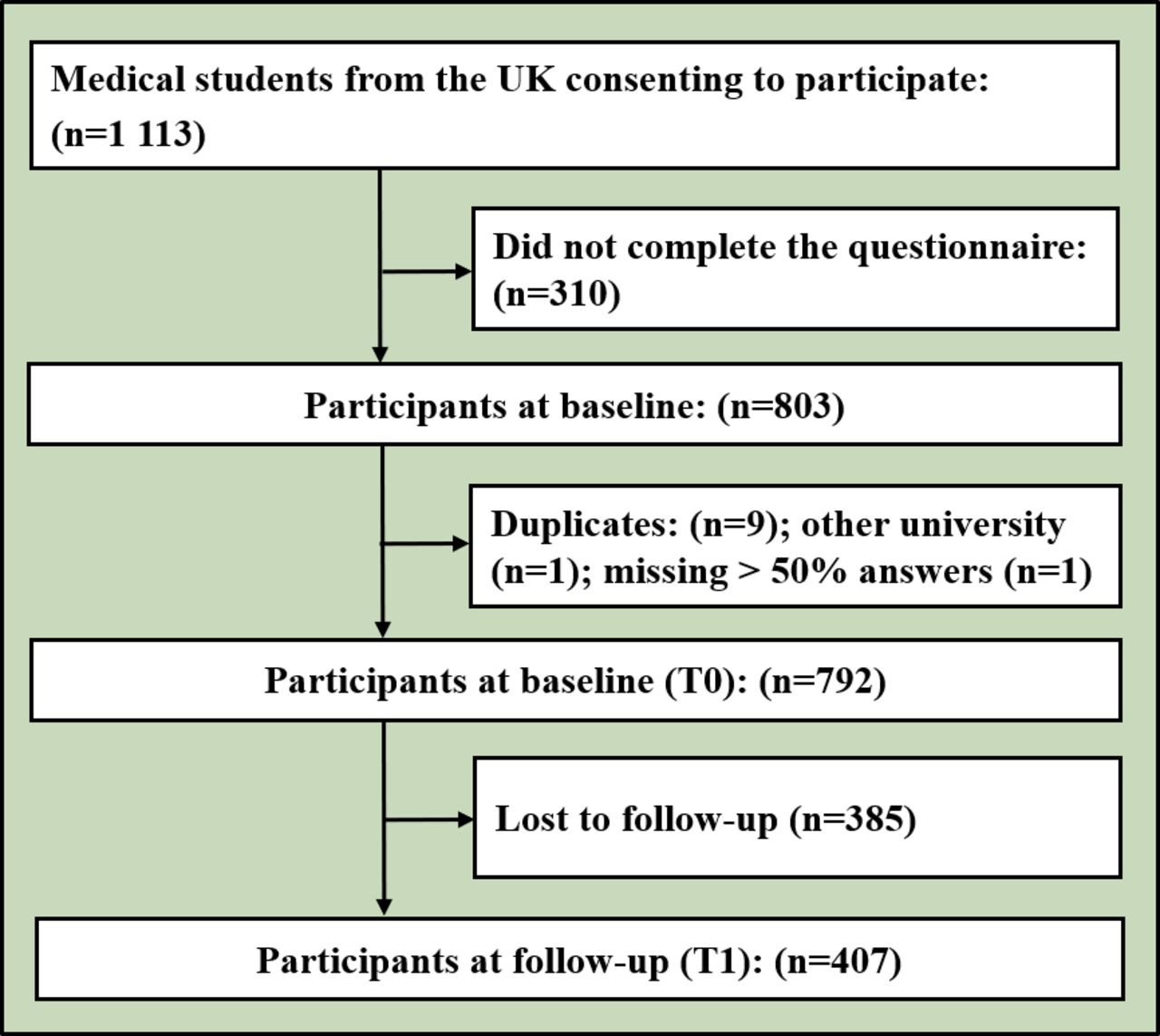
Staff at the nine medical schools distributed the study recruitment material to their medical students in various ways, including email, social media and lecture announcements. Of the 1 113 medical students who consented to participate in the study, 310 did not complete the baseline questionnaire. Of the 803 participants who completed the baseline questionnaire, 11 responses were excluded: 9 were identified as duplicates, 1 had missed >50% of the answers and 1 participant originated from another university that was not included in the study. A total of 792 (71.16%) responses at T0 were included in the baseline analysis. Of the 792 T0 participants, 385 students were lost to follow-up. Four hundred and seven (51.39% of a total of 792) were included in the follow-up analysis, T1. The number of participants at each stage is presented in figure 1.
{kind=link}
Study enrolment flowchart. T0, baseline; T1, 3-month follow-up.
Variables and measures
At both points in time, we used an identical questionnaire to measure a variety of mental ill-health symptoms (rather than clinical diagnoses) as outcomes and various influencing factors. The latter included eight measures: two educational climate measures, belongingness, help-seeking intentions, two stigma measures and two measures related to the impact of the pandemic. Two educational climate measures assessed the centrality of the learner, reflecting a supportive, respectful learning environment and a level of competitiveness. Two stigma scales differentiated perceived stigma and observed stigma, that is, witnessing stigmatising behaviour carried out by fellow students and/or supervisors at medical schools (including teaching staff, junior doctors and consultants). As the study was conducted during the coronavirus disease 2019 (COVID-19) pandemic, to account for its impact, we measured: (1) the extent to which students felt prepared in their learning and in their readiness to practice as a doctor due to the pandemic and (2) the support provided by the medical school during the pandemic. Participants also provided their sociodemographic characteristics and a list of experienced stressful events. Table 1 describes all measures.
Overview of variables and measures used in the study of factors contributing to UK medical students’ mental ill-health symptoms
Quantitative variables and statistical methods
SPSS V.26.0 was used for the analysis. Participants were allowed to miss up to one-third of the data for each scale, and mean scores were computed over the remaining items. All scales were approximately normally distributed (skewness and kurtosis between −2 and 2; no extreme outliers). Internal consistencies (Cronbach’s α) were deemed sufficient (>0.7; table 1), except for the pandemic scale about support (0.662). As no further improvements were possible and the scales were relevant to the study context, these scales were kept in their original form. Correlation matrixes (Pearson’s correlation coefficients) are presented in online supplemental appendix 1.
Supplemental material
The prevalence of mental health issues was calculated based on the diagnostic cut-off (table 1) for the entire baseline sample (T0). We chose this sample as we were not investigating the changes in mental health issues over time but instead aimed to understand the prevalence of mental ill-health symptoms among medical students at one given time. The T0 dataset offered a larger dataset for this aim.
Longitudinal data were used to investigate the factors associated with mental health issues. For continuous outcomes, unadjusted and adjusted growth curves were performed (an unstructured covariance matrix was compared with a compound symmetry matrix; residual maximum likelihood estimation). For dichotomous outcomes, unadjusted and adjusted Generalised Estimating Equations (GEE) (unstructured covariance matrix) were compared with the performance of an independent matrix (Fisher’s scoring). Based on differences in the outcome and associated factors among demographic characteristics (online supplemental appendix 2), we adjusted for stressful events, gender, ethnicity, sexual orientation, widening participation (widening participation students are students from disadvantaged backgrounds who receive premiums and/or supportive measures when accessing education. The aim of widening participation schemes is to increase diversity and representation within education), and the school year. Missing data were not imputed but handled by the analysis procedure, except for GEE, for which missing values were listwise deleted. P values <0.05, <0.01 and <0.001 for two-sided tests, and a Bonferroni correction (17 tests, p value with Bonferroni correction equals 0.003) are reported.
Results
Participants
The majority of the 792 medical students at baseline were female (585, 73.9%), of white ethnicity (501, 63.3%) with at least one parent/guardian/carer whose occupation was higher managerial (599, 75.6%) and were first-year students (230, 29.0%) (table 2).
Demographic characteristics of baseline and follow-up participants
Prevalence of mental health issues
Two hundred and thirteen (26.9%) participants who completed the baseline survey reported having an official diagnosis of mental illness.
The prevalence of measured symptoms of mental ill-health is presented in table 3. The most prevalent mental ill-health symptoms were somatisation and hazardous drinking: over half of the students experienced medium or (very) high somatic symptoms (402, 50.8%) and were drinking hazardously (494, 62.4%). Other prevalent mental ill-health symptoms included obsessive-compulsive disorder (OCD) (384, 48.5%), schizoid personality disorder symptoms (370, 46.7%) and anorexic tendencies (353, 44.6%). Approximately one in three students were burnt-out, had moderate/severe symptoms of anxiety/depression (305, 38.5%) and had histrionic personality disorder symptoms (270, 34.1%). Nearly one in five students experienced clinical insomnia (152, 19.2%) and paranoia symptoms (148, 18.7%). Lower prevalence was reported for bulimia tendencies, drug use, bipolar and antisocial personality disorder symptoms (<7%).
Prevalence of mental health issues in medical students in the UK
Predicting mental health issues
Results from the adjusted models are presented in tables 4 and 5 (complete information can be found in online supplemental appendix 3).
Estimates with 95% CI of adjusted models testing what factors associated with the mental ill-health symptoms—burnout and anxiety/depression-induced issues
Estimates with 95% CI of adjusted models testing what factors associated with mental ill-health symptoms—physical symptoms, substance use, personality disorder, mood disorder and official diagnosis
Burnout
More supportive medical schools’ educational climates, focusing on the centrality of the learner and with lower levels of competitiveness, significantly linked with less emotional exhaustion (centrality: Badjusted=−0.51, 95% CI: 0.80 to −0.23, p<0.001; competition: Badjusted=−0.42, 95% CI: −0.66 to −0.18, p<0.001), cynicism (centrality: Badjusted=−0.72, 95% CI: −1.03 to −0.41, p<0.001; competition: Badjusted=−0.33, 95% CI: −0.60 to −0.07, p=0.012) and higher personal accomplishment (centrality: Badjusted=0.62, 95% CI: 0.40 to 0.84, p<0.001; competition: Badjusted=0.21, 95% CI: 0.02 to 0.40, p=0.031). Students who felt that they belonged experienced lower levels of exhaustion (Badjusted=−0.19, 95% CI: −0.30 to −0.08, p<0.001) and had higher levels of personal accomplishment (Badjusted=0.22, 95% CI: 0.13 to 0.30, p<0.001).
Students who perceived mental health issues as more stigmatised (Badjusted=0.28, 95% CI: 0.08 to 0.48, p=0.006) and who were less inclined to seek help were more cynical (Badjusted=−0.18, 95% CI: −0.31 to −0.04, p=0.01). Feeling unprepared (with learning and for becoming a doctor) due to the pandemic was linked to higher levels of burnout (emotional exhaustion: Badjusted=0.19, 95% CI: 0.07 to 0.30, p=0.001; cynicism: Badjusted=0.15, 95% CI: 0.03 to 0.27, p=0.014; low personal accomplishment: Badjusted=−0.11, 95% CI: −0.20 to −0.03, p=0.012).
Anxiety/Depression-induced symptoms
Students who felt they belonged experienced lower levels of anxiety/depression symptoms (Badjusted=−0.08, 95% CI: −0.14 to −0.01, p=0.031) and higher levels of bulimic tendencies (Badjusted=0.58, 95% CI: 0.05 to 1.11, p=0.033). Perceived stigma about mental ill-health linked with increased levels of anxiety/depression symptoms (Badjusted=0.20, 95% CI: 0.09 to 0.31, p=0.001), anorexic tendencies (Badjusted=0.71, 95% CI: 0.37 to 1.04, p<0.001), bulimic tendencies (Badjusted=1.41, 95% CI: 0.43 to 2.38, p=0.005), binge-eating tendencies (Badjusted=0.74, 95% CI: 0.13 to 1.36, p=0.018) and OCD symptoms (Badjusted=0.39, 95% CI: 0.22 to 0.55, p<0.001). Students who felt unprepared due to the pandemic also experienced higher levels of anxiety/depression symptoms (Badjusted=0.11, 95% CI: 0.04 to 0.18, p=0.003). Observed stigmatising behaviour was associated with reduced binge-eating tendencies (Badjusted=−0.77, 95% CI: −1.51 to −0.04, p=0.039).
Physical symptoms
Students who felt that they belonged (Badjusted=−0.10, 95% CI: −0.17 to −0.03, p=0.006) and who were more inclined to seek help (Badjusted=−0.10, 95% CI: −0.19 to −0.02, p=0.013) experienced lower levels of insomnia symptoms. Perceived stigma was associated with insomnia (Badjusted=0.23, 95% CI: 0.11 to 0.35, p<0.001) and somatisation symptoms (Badjusted=0.15, 95% CI: 0.05 to 0.26, p=0.005). Those students who felt unprepared due to the pandemic expressed more severe symptoms of somatisation (Badjusted=0.07, 95% CI: 0.01 to 0.13, p=0.034).
Substance use
Belongingness was linked to higher odds of hazardous drinking (Badjusted=0.28, 95% CI: 0.07 to 0.49, p=0.010) while help-seeking intentions linked to lower odds of hazardous drinking (Badjusted=−0.30, 95% CI: −0.54 to −0.07, p=0.012). Students who observed stigmatising behaviour from their peers and supervisors were at higher odds of hazardous drinking (Badjusted=0.81, 95% CI: 0.36 to 1.27, p<0.001) and drug use (Badjusted=1.04, 95% CI: 0.27 to 1.80, p=0.008). Perceived stigma reduced the odds of drug use (Badjusted=−0.75, 95% CI: −1.43 to −0.07, p=0.031).
Personality disorders
Perceived stigma was positively linked to schizoid personality disorder (Badjusted=0.56, 95% CI: 0.24 to 0.89, p=0.001) and paranoia symptoms (Badjusted=0.42, 95% CI: 0.29 to 0.55, p<0.001). Belongingness was linked to lower odds of schizoid personality disorder symptoms (Badjusted=−0.31, 95% CI: −0.50 to −0.11, p=0.002) and help-seeking was linked to lower odds of paranoia symptoms (Badjusted=−0.09, 95% CI: −0.18 to 0.00, p=0.042). Students who observed stigmatised behaviour (Badjusted=0.48, 95% CI: 0.04 to 0.93, p=0.034) and those who felt more prepared due to the pandemic (Badjusted=−0.23, 95% CI: −0.44 to −0.02, p=0.035) had higher odds of developing histrionic personality disorder symptoms.
For the antisocial behaviour scale, running an adjusted model was impossible because of the small number of students scoring positive on this diagnostic test. Therefore, we performed two logistic regressions (with and without control variables), including antisocial personality disorder symptoms at baseline (online supplemental appendix 4). The adjusted model revealed that students from a less competitive environment (B=2.04, SE=1.04, p=0.049) and those who felt they belonged (B=−1.29, SE=0.56, p=0.022) were less likely to have antisocial personality disorder symptoms.
Mood disorder
There was a significant positive link between belongingness and bipolar symptoms (Badjusted=0.03, 95% CI: 0.01 to 0.05, p=0.013). Students inclined to seek help were experiencing lower levels of bipolar symptoms (Badjusted=−0.05, 95% CI: −0.08 to −0.03, p<0.001).
Official diagnosis of mental illness
Help-seeking intentions (Badjusted=−0.51, 95% CI: −0.81 to −0.21, p=0.001) and perceived (Badjusted=−0.77, 95% CI: −1.19 to −0.36, p<0.001) and observed (Badjusted=−0.53, 95% CI: −1.05 to −0.02, p=0.043) stigma increased the odds of having a mental health diagnosis (see online supplemental appendix 3).
Discussion
Main findings
Prevalence of mental health issues
The prevalence of mental health issues among UK medical students who participated in this study was high, with some mental ill-health symptoms occurring in more than half of the students. For example, 62% of medical students reported drinking hazardously. Both coping (ie, reducing negative affect and anxiety) and enhancement (ie, increasing positive affect) motivations could help explain these findings,22 considering the challenging medical school environment and the importance of socialising for young people. The time over which the data were collected in the present study included periods of easing pandemic-related social restrictions. Thus, students may have engaged in more frequent socialising activities and drank more than usual. However, other studies on students before the pandemic more generally report a similar or higher prevalence of alcohol use among undergraduate students in the UK and Ireland (62.8%–84%).23
Comparing findings from studies on medical students globally (see online supplemental appendix 5), the prevalence reported for more commonly explored mental health issues was mostly similar to those found here. For example, we found that 33.1% of medical students perceived their personal accomplishments as low and 38.5% had anxiety/depression symptoms, while systematic reviews on medical students globally report that 27.4% had low personal accomplishments21 and 39.4% had depression.7 However, general population studies report lower prevalence in comparison with our findings: systematic reviews show that 28% of the general population globally had depression and 26.9% had anxiety24 in comparison with 38.5% of medical students expressing anxiety/depression symptoms in our study. Other mental health issues, such as eating or personality disorders, have been less often explored in medical students, and evidence in comparable samples is lacking. Those issues are, however, significant to consider as higher stigma might be associated with these mental health issues and therefore reduce disclosing; for example, doctors are less likely to reveal substance use problems than anxiety.25 Health policy should specifically focus on preventative and awareness-raising campaigns regarding these issues to ensure that those who need support seek it.
Comparing our findings with studies exploring the prevalence of these mental health issues in the general population, we find the prevalence is higher among medical students (eg, binge eating: 1.4%26 vs 8.5%), including some drastic differences (eg, schizoid personality disorder: 2.82%27 vs 46.7%). This high prevalence may be partially due to the sample’s characteristics. The study focuses on young individuals facing several challenging life circumstances: becoming independent, establishing a career and long-lasting relationships, facing a changed learning environment and experiencing an increased workload.28 However, the COVID-19 pandemic may also have influenced the prevalence of specific health issues. Alcohol use and eating disorders such as anorexia nervosa, for example, have increased in prevalence since the beginning of the pandemic.29 30 Research also shows that the pandemic exacerbated symptoms for those with personality disorders.31
Factors associated with mental ill-health
An underlying medical learning climate in which disrespectful behaviours are engrained has been identified as the potential culprit for the issues experienced by medical students.32 33 Our study notably showed the detrimental impact of such a climate on burnout. Occupational and professional demands catalyse burnout34; for medical students, these occupational and professional demands manifest in their learning environment. A direct link between educational climate and burnout is also shown elsewhere.35 Interestingly, the educational climate—the centrality of the learner and competitiveness—did not significantly impact other mental health issues. This could be due to burnout being a mediator, as studies have shown that burnout is predictive of mental disorders.36 Therefore, improving the educational climate in medical schools is crucial for students’ well-being as it might prevent the exacerbation of mental health issues. Although the educational climate is resistant to change, successful efforts to improve learning environments have been reported, such as implementing a pass/fail grading system rather than numerical marking to reduce competitiveness among medical students.32
Furthermore, our results imply that students with a stronger sense of belongingness experienced lower symptoms of mental ill-health issues, aligning with the literature describing that not belonging and even uncertainty about belonging can lead to isolation, emotional distress, exhaustion and other health issues.37 These findings were relevant to a variety of mental health problems. Nonetheless, there is a potential flipside to belongingness, such as increased drinking behaviour: intoxication through alcohol is seen as a collective activity to be enjoyed in a group.38 Therefore, the students in our sample may feel like they belong due to more extensive networks of peers with whom they can engage in social activities, including drinking.
Stigma and help-seeking intentions were particularly impactful on students’ mental health. There are stigmatising attitudes to mental illness in the wider medical culture,39 and it is strongly represented in medical school.40 Stigma might prevent timely support-seeking40 and cause students to hide their symptoms, potentially worsening the problem or leading to self-medication.41 This is problematic in medical school and later when these students progress to become physicians. Research shows that, despite a recent reduction in public stigma towards mental ill-health42 and increased mental health campaigns specific for medical professionals,43 younger doctors still report holding more stigmatising attitudes towards mental illness and experience more barriers when seeking help than older doctors.39 This indicates there is still work to be done, and our research implies that efforts to reduce stigma towards mental illness in the medical community must start in medical school.
Finally, the results of this study showed the pandemic’s effects on medical students’ learning—leading them to feel underprepared for their studies and less equipped to become exemplary physicians—decreased their mental health. The culture of perfectionism in medicine can leave learners with diminished self-worth, a stigmatised sense of failing, less sleep due to worrying and prioritising learning activities and ultimately mental health issues.44 The findings were particularly relevant for burnout (manifesting from the professional environment) potentially because substantial changes were implemented in medical schools due to the pandemic, such as online learning and suspended placements.45 Noteworthy, the amount of perceived support from medical schools during the pandemic did not significantly impact students’ mental health. Despite the many policy changes, students may have felt medical schools were doing all they could to support them through the pandemic.
Limitations
This study’s participants may represent a particular type of students. For example, students experiencing mental health issues may have been more or less keen to participate. But due to the recruitment strategy, the researchers had little influence on whom and how many students were reached. The researchers mitigated this risk to the best of their ability by collaborating with medical schools to recruit a diverse sample and designing inclusive recruitment materials, both written and spoken. Furthermore, the geographical and demographically diverse selection means the sample is more likely to accurately represent the overall population of medical students, thereby contributing to the generalisability of the study.
Attrition bias, caused by the drop-out of participants, could impact the generalisability and sharpen the selection bias. However, there were no substantial differences between those who completed the follow-up survey (407) with those who did not (385) (online supplemental appendix 6).
Despite the elaborate recruitment strategy, some analyses were conducted over small groups of students, particularly for outcomes with a low prevalence, such as bulimic and binge-eating tendencies, antisocial personality disorder symptoms, bipolar symptoms and drug use. Although we were able to perform the analysis for these outcomes, the findings should be interpreted with caution. This may also explain why some results found for these outcomes are counterintuitive, such as students feeling underprepared due to the pandemic experiencing lower odds of binge-eating tendencies.
Data collection took place during the COVID-19 pandemic, and the possible impact of the pandemic on the results deserves consideration. Research in the UK on the COVID-19 pandemic’s impact on medical students’ mental health is explicitly scant. However, one study reported that students studying healthcare-related courses at a British university have had a negative impact on lifestyle behaviours, such as changes in diet and decreased exercise, and mental health, for example, worrying too much and feeling unable to cope.46 This reflects the global literature, which suggests the pandemic has negatively affected medical students’ mental health. For example, a study of 2 280 medical students across 148 medical schools in 9 countries (Brazil, Chile, Columbia, Germany, Italy, Japan, Mexico, Spain and Venezuela) found students reported negative changes in both their mental and physical health, including insomnia, emotional irritability, anhedonia, headaches and ocular tiredness.47 Therefore, as mentioned above, it is important to consider that the COVID-19 pandemic may have inflated the prevalence of certain mental health issues.
Implications
First, the educational climate and students’ attitudes towards mental illness impact the mental health of medical students. Thus, a preventative approach that safeguards learning environments and addresses perceived stigma and encourages help-seeking is crucial. Interventions should be tailored to students with a broad range of mental health problems and created through collaboration and dialogue between staff and students. Second, medical schools should stress the importance of healthy peer-to-peer and student-to-staff relationships, address stigma and avoid unnecessary competitiveness to help to create a healthier learning environment for students.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the UCL Research Ethics Committee (REF: 14983/002). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the medical schools, medical students, student volunteers and steering group members who supported this study. We would also like to thank Dr Rowena Viney for suggestions on improving the manuscript’s narrative.
References
Asta Medisauskaite obtained her PhD in Organizational Psychology from Birkbeck, University of London, UK, in 2018 and her master’s degree from the Vytautas Magnus University, Lithuania, in 2011. In 2017, Dr Medisauskaite started working at University College London (UCL), UK and now is a Senior Research Fellow at UCL Medical School, Research Department of Medical Education. Dr Medisauskaite is interested in occupational health psychology research, including mental health and wellbeing of medical professionals.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @astamedis
Contributors Concept and design: AM, MEWMS and AR. Acquisition, analysis or interpretation of data: AM and MEWMS. Drafting of the manuscript: all authors. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: AM and MEWMS. Guarantor: all authors.
Funding This study was funded by the British Medical Association (BMA) Foundation (Scholarship grant).
Disclaimer The views expressed here are those of the authors and do not necessarily reflect the position or policy of the BMA Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.