Article Text

Abstract
Background Presently, approaches for the early treatment of pathological anxiety in patients with chronic non-communicable diseases are lacking, thus delaying the initiation of symptom management at the early onset of the illness. Proactive psychological and psychiatric support, to alleviate subclinical symptoms of anxiety and to improve the quality of life in patients with chronic non-communicable diseases, is a promising candidate for the role of such therapy.
Aims To investigate and determine the effectiveness of proactive psychological and psychiatric support for alleviating subclinical symptoms of anxiety and improving quality of life, in patients with chronic non-communicable diseases.
Methods The study design was a monocentric randomised controlled trial with parallel groups. The study, involving 193 inpatients with chronic non-communicable diseases, complied with the ethical and deontological norms in accordance with the principles set out in the Declaration of Helsinki. Instruments used in the study included the Hamilton Anxiety Scale (HAM-A) to assess subclinical symptoms, the Scale of Somatic Symptoms and the Chaban Quality of Life Scale. Block randomisation was used to randomise patients to a 2-month-long study group with a proactive counselling psychiatry model care or a control group with standard regulated treatment for chronic non-communicable diseases. The allocation ratio was 1.15:1 owing to the expectancy of a higher percentage of dropout in the intervention group.
Results After 60 days of treatment (T2), there was a statistically significant difference in all clinical parameters between the study and control groups. The median HAM-A value differed between the groups by 4.87 points, with statistically significant lower results in the study group. The comparison of the study group’s scale values on day 1 and day 60 demonstrated statistically significant changes in all three indicators.
Conclusions Our results support existing evidence for the effectiveness of proactive psychological and psychiatric support to reduce subclinical anxiety and somatisation symptoms and to improve the quality of life for patients with common chronic non-communicable diseases. However, continued research on the effectiveness of proactive psychological and psychiatric support for patients with chronic non-communicable diseases is needed.
- psychosomatic medicine
- psychotherapy, multiple
- psychiatric somatic therapies
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
About 20% to 40% of patients in multidisciplinary hospitals suffer from mental illnesses, significantly complicating the course of their disease, therapy effectiveness and somatic pathology prognosis. The conceptualisation of proactive psychosomatic medicine currently being developed in the world offers another way of providing psychological-psychiatric medicine to patients in general medical units of multidisciplinary hospitals. Based on the successful experience of using this approach during the coronavirus disease 2019 (COVID-19) pandemic, proactive models of psychological-psychiatric care are being actively implemented in general somatic practice, providing an essential link in the management structure of somatic pathology. However, there is currently a lack of information in the scientific medical literature regarding the effectiveness of these proactive models of care in treating anxiety associated with chronic non-communicable diseases.
WHAT THIS STUDY ADDS
The study data show that proactive psychological and psychiatric support in somatic medical practice is viable and effective, especially for patients with subclinical anxiety manifestations.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study substantiates the feasibility of implementing proactive psychological and psychiatric care for patients with somatic diseases. Advanced research is needed to create personalised approaches and obtain further evidence of their effectiveness for patients of different nosology, age, gender and other groups.
Introduction
Without question, the medical community recognises that many patients with organic diseases and other forms of bodily illness also suffer from psychiatric and psychological problems. Various models of medical care to address these needs have been proposed, with some showing greater efficacy than others, even as the models continue to evolve and new ones are developed. One model that has gained the attention of researchers worldwide is proactive psychosomatic medicine (PPM), a qualitative approach to providing psychological-psychiatric services to patients in non-psychiatric departments of general hospitals. PPM is based on the biopsychosocial theory and its clinical implementation—consultation-liaison psychiatry. The main principles include initiative, purposefulness, intensity and integration with general medical care.1 2
The psychological-psychiatric care system evolved in general medical practice because of the need for new mechanisms to manage the psychological and social aspects associated with diseases. If insufficiently addressed, inpatients’ unmet psychosocial needs interfere with their medical treatment effectiveness. Consequently, some patients may experience a more severe course of the disease and increase their length of hospitalisation while simultaneously placing a greater burden on the healthcare system.3 Meta-analyses findings on the concept of proactive psychiatric counselling, with confirmation by medical experts’ consensus,2–5 showed that from 2011 to 2018, 20% to 40% of patients in multidisciplinary hospitals also had a mental illness, significantly complicating the course of somatic pathology, the effectiveness of therapy and the prognosis, especially for non-communicable diseases.6–8
It is indisputable that patients’ mental illness in multidisciplinary hospitals often hinders timely discharge, leads to additional specialist consultations and increases total medical care costs. Based on the studies mentioned above, evidence supports psychological-psychiatric counselling as an important method for monitoring somatic patients. The main features of the proactive model of consultation-liaison psychiatry were identified: multidisciplinary care that includes joint supervision and close patient observation by a psychiatrist, primary care physician, psychologist, nurse and social worker. This team not only makes recommendations for treatment, risk reduction and crisis management—typical of the traditional care models—but also exerts efforts to prevent behavioural barriers to care, avoid crises and boost the synergy of patients.4
In 2019, HOME Study,9 a randomised controlled trial, compared the addition of proactive psychological medicine to usual care and then measured the amount of time older, acutely ill patients spent in the hospital. It also formulated the following specific recommendations for the organisation of inpatient psychiatric services and psychological and psychiatric interventions for patients of general medical practice, using the model of consultation-liaison psychiatry:
An early proactive biopsychosocial assessment of recently hospitalised patients to identify all problems, including mental illness.
The creation of a plan for comprehensive supervision and systematic management of the specific problems likely to cause potential obstacles to a rapid hospital discharge.
The implementation of a comprehensive treatment plan, including daily psychosomatic examinations to measure the patient’s progress.
Integrated work with the staff of various departments (doctors, nurses, other counsellors and social work specialists) and outpatient services to ensure the implementation of the comprehensive care plan.
In December 2020, a resource document on proactive consultation-liaison psychiatry, initiated by the Council of the American Psychiatric Association, was approved for publication. This document1 emphasises the implementation of a model of proactive consultation-liaison psychiatry that contains the following four elements:
Systematic screening focusing on current mental health problems in somatic patients (patients hospitalised in certain health facilities are systematically checked for signs of active mental health problems, especially those who may be at higher risk).
Early clinical intervention (proactive measures tailored to individual patients with a combination of interventions for somatic and mental disorders).
Providing care based on a multidisciplinary team approach (the mental health team is part of a multidisciplinary hospital and provides comprehensive mental healthcare directly in a general hospital).
Integration of care with primary teams and services (a proactive psychological-psychiatric team closely coordinates the work with primary services in real time between clinicians with relevant experience: doctor to doctor, nurse to doctor/nurse, social worker to social worker/rehabilitation specialist and vice versa).
Proactive models of psychiatric care are now increasingly recognised and widespread because of the effectiveness of their implementation in treating patients during the coronavirus disease 2019 (COVID-19) pandemic. For example, some hospitals created separate departments specifically for treating patients with COVID-19 with acute psychiatric needs10; others chose to develop psychological-psychiatric units or consultation-liaison psychiatry care within the established structure of multidisciplinary hospitals.11 12 The positive effects of reducing the treatment costs and length of hospital stay of patients with COVID-19 were emphasised.13–16 Based on the recent success of these approaches during the pandemic, proactive models of psychological-psychiatric care have been widely implemented in general practice as an essential link in managing somatic pathology. However, current scientific literature lacks information regarding their effectiveness in treating the anxiety associated with chronic non-communicable diseases. Therefore, this study aimed to evaluate the effectiveness of the proactive consultation-liaison psychiatry model, using the PPM conceptualisation, for the relief of subclinical symptoms of anxiety in patients with chronic non-communicable diseases.
Methods
The study design was a randomised controlled trial with parallel groups. It adhered to the ethical and deontological norms in accordance with the principles set out in the Declaration of Helsinki. Initially, 209 subjects were selected from inpatients hospitalised at Kyiv Railway Hospital No 1 for non-communicable diseases from June 2021 to December 2021. Inclusion criteria for study participants were as follows: (1) all men and non-pregnant, non-breastfeeding women aged 18 to 65 years, (2) diagnosis of a non-communicable somatic disease and (3) a score of fewer than 24 points on the Hamilton Anxiety Scale (HAM-A). Exclusion criteria for study participants were: (1) participation in another study within 1 month of screening, (2) a diagnosis of mental disorder, (3) a history of traumatic brain injury or stroke, (4) abuse of psychoactive substances at the time of screening and (5) the use of antidepressants for 1 month or less before enrolment in the study. Before the study began, all participants reviewed the protocol and signed informed consent. One hundred and ninety-three subjects met the inclusion criteria, and they were then screened for signs of current mental health problems, especially patients deemed to be at risk.
Endpoints
The primary endpoint was the overall HAM-A score. Secondary endpoints were the overall scores on the Somatic Symptom Scale-8 (SSS-8) and the Chaban Quality of Life Scale (CQLS).
Psychodiagnostic tools
The HAM-A was used to assess subclinical symptoms. Further information about the patient’s condition was obtained using SSS-8 and the CQLS.
Hamilton Anxiety Scale (HAM-A). The Hamilton Anxiety Scale, consisting of 14 items, was administered to all subjects by a psychiatrist/psychologist during a structured clinical interview.17 Interpretation of the final score was based on the recommendations of the National Institute for Health and Care Excellence (NICE) guidelines for Generalised Anxiety Disorder and Panic Disorder in Adults: management (CG113). Asymptomatic anxiety was defined as a HAM-A score ≤9; mild anxiety as a HAM-A score of 10 to 15; moderate anxiety as a HAM-A score of 16 to 24 and severe anxiety as a HAM-A score ≥25.
Somatic Symptom Scale-8 (SSS-8). SSS-8 is a short self-questionnaire of somatic manifestations of depression developed by Gierk et al.18 It consists of eight questions, each rated from 0 to 4 points, where 0=‘not bothered’ and 4=‘very worried’. Somatic symptoms were assessed by calculating the total score, varying from 0 to 32 points. The degrees of manifestation intensity as measured by points of somatic symptoms were rated as follows: 0–3=minimum, 4–7=mild, 8–11=moderate, 12–15=severe and 16–32=very severe.
Chaban Quality of Life Scale (CQLS). CQLS, a questionnaire designed to assess the quality of life, contains 10 items regarding various aspects of the subject’s life. The participants are asked to rate various areas of their lives from 0=‘not at all satisfied’ to 10=‘extremely satisfied’. Quality-of-life assessment is done by calculating the total score, which can vary from 0 to 100. Score points correspond to the following quality-of-life levels: ≤56=very low, 57 to 66=low, 67–75=moderate, 76–82=high and >83=very high. Correlation coefficients between test and retest scores confirmed the reliability of CQLS (r=0.923, p<0.001) and Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q) (r=0.862, p<0.001).19
Research protocol
After receiving information about the study, providing written informed consent and undergoing a screening procedure, on day 1 of the study (T1), participants were administered the CQLS and SSS-8 questionnaires in addition to a structured clinical interview with the HAM-A to assess their anxiety. The groups’ sociodemographic information is shown in table 1. Group participation was determined by block randomisation to obtain equivalent groups. Patients were assigned to the PPM model study group (SG) (n=104) or the control group (CG) (n=89) who received standard treatment for chronic non-communicable disease according to established clinical protocols. After 60 days, a reassessment was performed using the HAM-A, SSS-8 and CQLS. Results are shown in table 2. The study design is presented in figure 1.
Sociodemographic variables of study participants
Repeated-measures ANOVA results for HAM-A, SSS-8 and CQLS

Flowchart of study design and distribution of respondents into groups. CQLS, Chaban Quality of Life Scale; HAM-A, Hamilton Anxiety Scale; SSS-8, Somatic Symptom Scale-8.
Statistical analysis
Qualitative data are presented through the number of observations and their percentage. The Shapiro-Wilk test was used to assess the normality of the distribution of quantitative indicators. The t-test for unrelated samples (in case of submission to the law of normal distribution) was used to estimate the difference between two unrelated samples. In the case of an abnormal distribution, the Mann-Whitney U test for unrelated samples was used to estimate the difference between two unrelated samples. The t-test for bound samples was used to estimate the difference between two bound samples in the case of a normal distribution; the Wilcoxon test for unbound samples was used in the case of an abnormal distribution. In addition, type III repeated-measures analysis of variance (ANOVA) was used to analyse the shifts difference in groups. Statistical data processing was performed with R, the programming language using the environment for statistical calculations EzR V1.54. Data were visualised using the Python programming language with matplotlib and seaborn add-ons.
Results
Of the 209 inpatients with non-communicable somatic illnesses who were eligible for participation, 16 refused participation and 193 were enrolled for screening procedures after being provided information about the study. Only data from the 193 subjects were analysed in the final processing of the results. The mean age of patients in the study group (n=104) was 36.08 (10.37) years, and the mean age in the control group was 38.78 (9.87) years (t=1.843, p=0.066). Of the total, 115 subjects (59.6%) were women (59.6% in SG, 59.6% in CG), while 78 subjects (40.4%) were men (40.4% in SG, 40.4% in CG) (p=0.992). One hundred and forty-five of the subjects (75.1%) at the time of the study were married (76.0% in SG, 74.2% in CG), and a minority (24.9%, n=48) were without a permanent partner (24.0% in SG, 25.8% in CG) (χ²=0.014, p=0.903). Almost all participants (n=185, 95.9%) were employed (97.1% in SG, 94.4% in CG). Only a few participants (n=8, 4.1%) were temporarily out of work (2.9% in SG, 5.6% in CG) (χ²=0.345, p=0.557). Thus, before randomisation, the groups had no significant difference in sociodemographic indicators (table 1).
Regarding participants’ somatic diagnoses, 101 (52.3%) had hypertension (48.1% in SG, 57.3% in CG, χ²=1.287, p=0.256), 56 (29.0%) had bronchial asthma (29.8% in SG, 28.1% in CG, χ²=0.010, p=0.918), 45 (23.3%) had diabetes mellitus (25.0% in SG, 21.3% in CG, χ²=0.182, p=0.669) and 16 (8.3%) had chronic obstructive bronchitis (4.8% in SG, 12.4% in CG, χ²=2.672, p=0.102). The majority of participants—167 (86.5%)—had one chronic non-communicable disease, while 26 (13.5%) had two comorbid diseases. Therefore, no statistically significant difference in morbidity was found before the randomisation of the groups.
At the start of the study, all 193 participants had subclinical anxiety as rated by the HAM-A scale: the mean score of the study group was 19.21 (1.04) and of the control group was 19.28 (1.06) (t=0.454, p=0.650). The initial SSS-8 measurements of participants’ somatic manifestation levels were as follows: 16 (8.3%) minimum, 50 (25.9%) mild, 61 (31.6%) moderate, 60 (31.1%) severe and 6 (3.1%) very severe. The average SSS score of the study group was 9.02 (3.81) and of the control group was 9.84 (3.96) (t=1.451, p=0.148). The initial CQLS results measuring participants’ quality-of-life levels at the study’s onset were as follows: 63 (32.6%) very low, 55 (28.5%) low, 41 (21.2%) moderate, 15 (7.8%) high and 19 (9.8%) very high. The average quality-of-life score of patients in the study group was 63.99 (15.21) and in the control group was 60.85 (14.50) (t=−1.458, p=0.146).
The results below show a reassessment of the presence and severity of anxiety, somatic symptoms and quality of life made at time point T2, 60 days after the initiation of proactive psychological and psychiatric support for the study group patients.
Anxiety
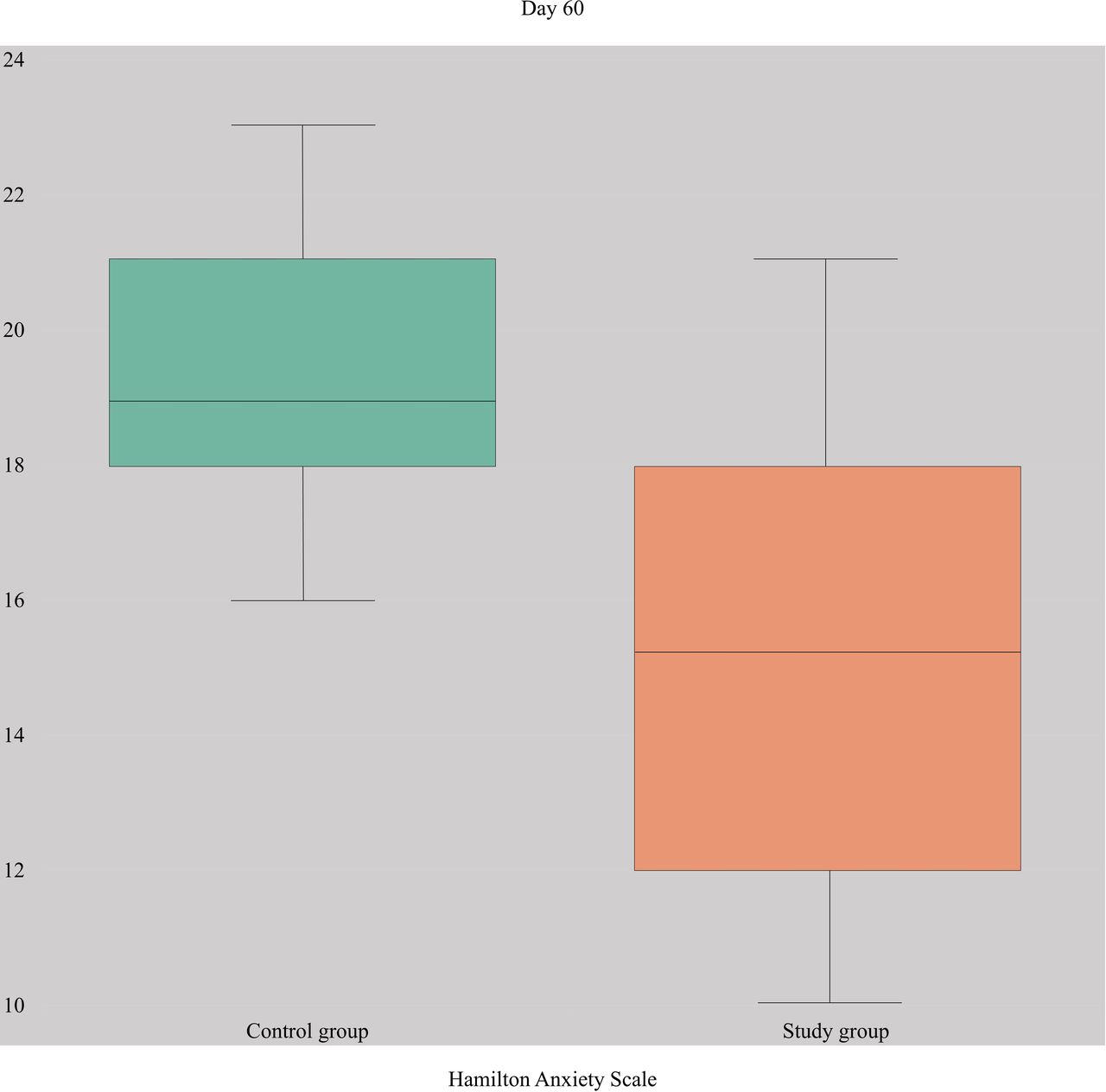
The median HAM-A value differed between groups by 5.22 points, with significantly lower results observed in the study group (14.34 (3.28), t=12.032, p<0.001) (figure 2), indicating a lower degree of anxiety in this group compared with the control group (19.56 (2.11)). The T2 HAM-A score for the study group also showed a significant decrease compared with the initial overall score (19.21 (1.04)). In addition, the results of repeated-measures ANOVA also revealed that the study group had better results over time than the control group (table 2).

HAM-A values and IQR in control and study groups. HAM-A, Hamilton Anxiety Scale; IQR, inter-quartile range.
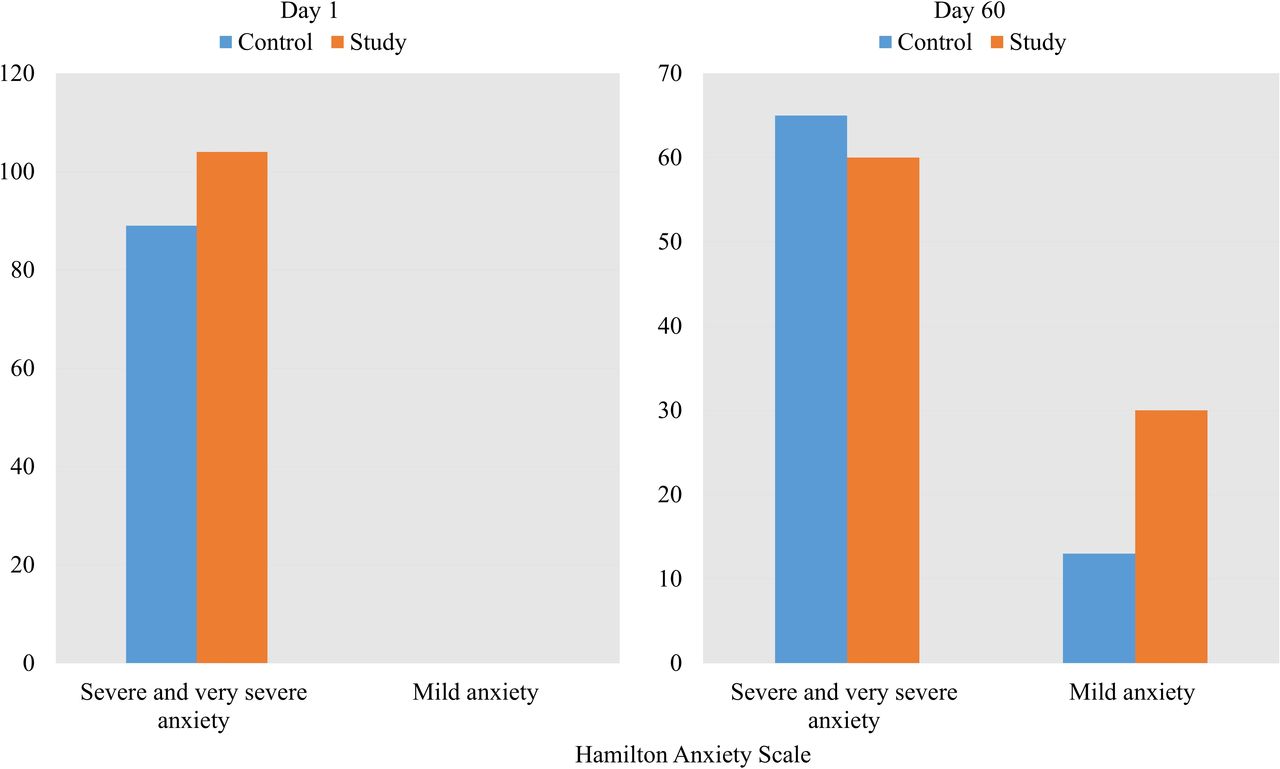
There was also a difference in the qualitative indicators of anxiety. At T1, all participants (n=193) had severe and very severe anxiety. At T2, of the 104 study group participants, 60 (57.7%) showed mild anxiety, while 30 (28.8%) showed severe and very severe anxiety. Data were missing from 14 (13.5%) participants. At the same time, a spontaneous but less common decrease in anxiety was found in the 89 control group participants, with 13 (14.6%) showing mild anxiety and 65 (73.0%) showing severe and very severe anxiety. Data were missing from 11 (12.4 %) participants. (figure 3). This difference was also statistically significant (χ²=50.90, p<0.001).

Comparison of qualitative HAM-A values between study and control groups on the 1st and 60th day. HAM-A, Hamilton Anxiety Scale.
Somatic symptoms
In addition to the reduction in anxiety manifestations, the occurrence and severity of somatic symptoms were also significantly reduced in study group patients; somatic complaints and manifestations decreased significantly (p<0.001) within the group (table 2). Somatic manifestation levels of the 104 participants in the study group at T2 were as follows: 69(66.3%) minimum, 9(8.7%) mild, 8(7.7%) moderate and 4(3.8%) severe. Data were missing from 14(13.5%) participants. Somatic manifestation levels of the 89 participants in the control group participants at T2 were as follows: 10 (11.2%) minimum, 12 (13.5%) low, 33 (37.1%) moderate, 20(22.5%) severe and 3(3.4%) very severe. Data were missing from 11 (12.4%) participants (figure 4A).
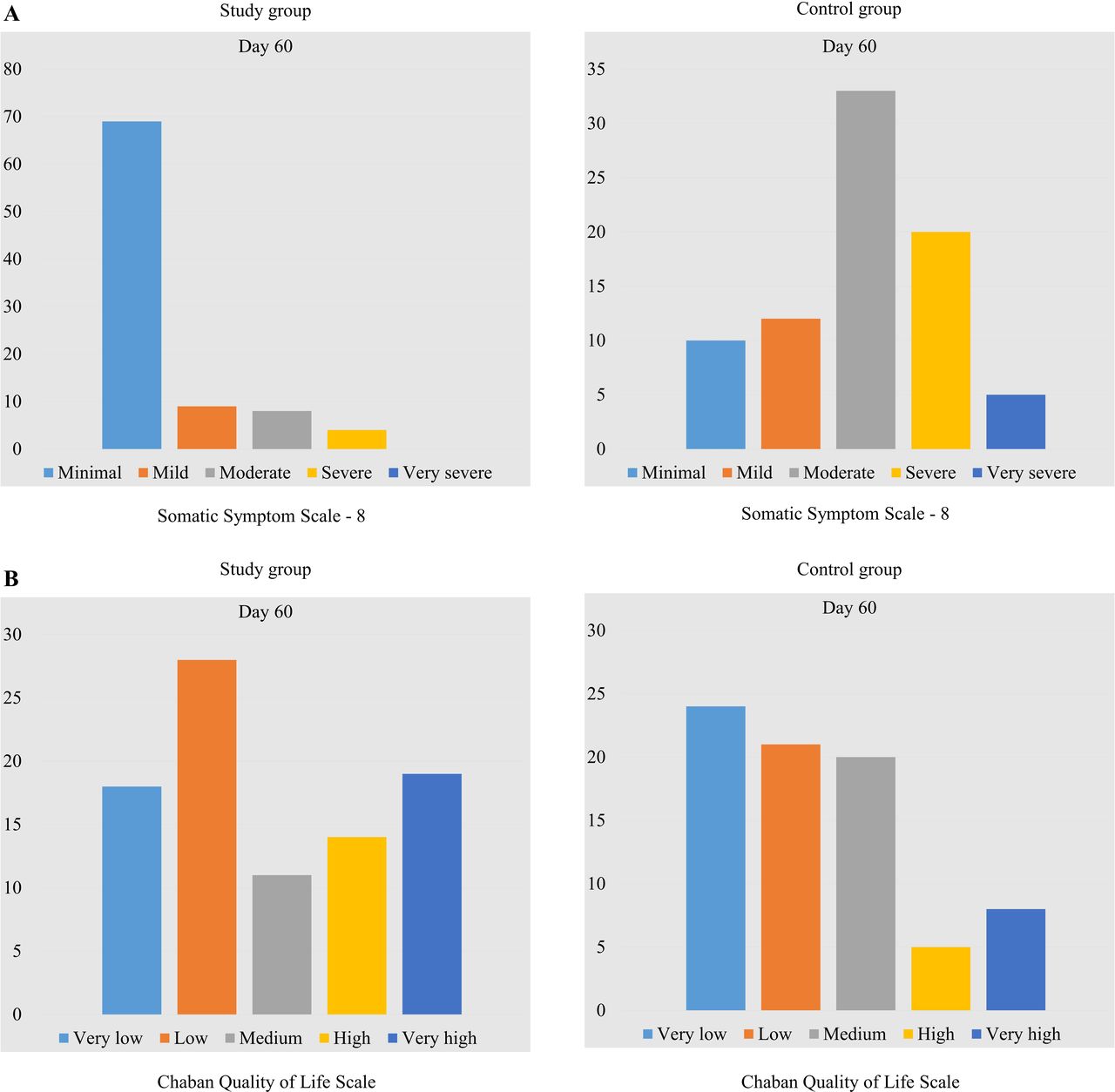
Comparison of qualitative SSS-8 values (A) and qualitative CQLS values (B) in all study participants on the 1st and 60th day. CQLS, Chaban Quality of Life Scale; SSS-8, Somatic Symptom Scale-8.
Quality of life
Improvement in quality of life was also recorded within the study group, with the difference between the two groups being statistically significant (p<0.05; table 2). At T2, levels of quality of life for the 104 study group participants were as follows: 18 (17.3%) very low, 28 (26.9%) low, 11 (10.6%) medium, 14 (13.5%) high and 19 (18.3%) very high. Data were missing from 14(13.5%) study group participants. In comparison, at T2, levels of quality of life for the 89 control group participants were as follows: 24 (27.0%) very low, 21 (23.6%) low, 20 (22.5%) medium, 5 (5.6%) high and 8 (9.0%) very high. Data were missing from 11 (12.4%) control group paticipants. A visual illustration of the data is presented in figure 4B.
The graph in figure 5 shows that after 60 days of proactive psychological and psychiatric support, anxiety symptoms decreased by 25.35% (a drop in median value by 4.87 points). The SSS-8 scale scores decreased even more by 63.08% (a decrease of the median value by 5.69 points). Moreover, CQLS quality-of-life indicators showed a 10.05% tendency toward improvement (an increase of the average value by 6.43 points).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
HAM-A, SSS-8 and CQLS score dynamics of the intervention and control groups on the 1st and 60th day. CQLS, Chaban Quality of Life Scale; HAM-A, Hamilton Anxiety Scale; SSS-8, Somatic Symptom Scale-8.
Discussion
Main findings
Our study findings support the effectiveness of proactive psychological and psychiatric support for treating somatically ill patients who also manifest subclinical anxiety. In this study, a multidisciplinary medical team implemented proactive psychological and psychiatric support by offering different interventions in the inpatient and outpatient treatment stages, including psychoeducation and low-intensity psychological interventions. Based on National Institute for Health and Care Excellence (NICE) recommendations, these methods show promising results in patients with anxiety disorders,20 and the psychoeducational measures have proven effective in treating mental disorders and non-communicable diseases.21
The selection of the tools used in this study to measure psychological impact was based on a systematic review and meta-analysis of 419 randomised controlled trials (n=53 288) published in 2021. This review focused on the effectiveness of multicomponent low-intensity psychological interventions based on awareness, cognitive–behavioural therapy techniques, acceptance and attachment therapy in both clinical and non-clinical populations.22 The findings emphasised the recommendations for using such treatment modalities in primary medical care and general somatic practice.20 Also, they cited well-argued evidence supporting the psychoeducation effectiveness in patients with psychosomatic pathology.21 Strengths of our study include its randomised controlled trial design and a sufficient study duration to detect the effect of proactive psychological and psychiatric support over time compared with regular treatment.
The allocation ratio, which was applied because of the expectation of a higher dropout rate in the intervention group, was used as a precaution, but the proactive psychological and psychiatric support of patients with chronic non-communicable diseases confirmed the effectiveness and efficiency of this method.
Limitations
The primary limitation of this study was the lack of a follow-up evaluation. Thus, it is impossible to compare the therapy’s effectiveness and the stability of the effects over time. Another limitation is the inevitable group heterogeneity among the studied patients with chronic non-communicable diseases. Further studies examining the effectiveness and safety of proactive psychological and psychiatric support in some homogeneous clinical populations are necessary to complement the results. Finally, the results of this study cannot be generalised to adolescent and elderly populations owing to the age of the study’s adult participants.
Implications
Our results support existing evidence for the effectiveness of proactive psychological and psychiatric support in treating patients with common chronic non-communicable diseases to reduce subclinical anxiety and somatisation symptoms and improve the quality of life. The application of this modality of psychological support for patients with chronic non-communicable diseases has already been shown to be feasible. However, its ongoing development and expansion require further research.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics approval
This study involves human participants and was approved by the Ethics Commission at the Kyiv Clinical Hospital on Railway Transport No 1 of the 'Health Care Center' Branch of the Joint-Stock Company 'Ukrainian Railway', protocol No 5 dated 20 May 2021. Participants gave informed consent to participate in the study before taking part.
References
Olena Khaustova graduated from the Luhansk Medical Institute in Ukraine in 1986 and, after completing her internship, received a specialization in psychiatry in 1987. She received a PhD with the thesis "Maladaptive mental reactions in workers of locomotive crews" in 1993, as well as a Doctor of Medical Sciences with the thesis "Mental and psychosomatic disorders in patients with metabolic syndrome X (diagnosis, clinic, prevention, treatment)" in 2006 at the Ukrainian Research Institute of Social and Forensic Psychiatry and Narcology. She also holds a master's degree in the "Sociology of Management and Public Relations" speciality in the Interregional Academy of Personnel Management in 2004. She has worked as a professor in the Department of Medical Psychology, Psychosomatic Medicine and Psychotherapy of Bogomolets National Medical University since 2009. She holds the position of professor in psychiatry and is also the Vice-President of the Ukrainian Association of Psychosomatic Medicine. She is the author or co-author of 487 publications, including 4 textbooks, 6 monographs, 18 manuals, 2 utility model patents, and 26 methodological recommendations. Scopus h-index: 2. Google Scholar h-index :16; i10 index: 30. Her main research interests include psychosomatic medicine, consultative liaison psychiatry, medical psychology, posttraumatic disorders, anxiety, and depression.

Footnotes
Twitter @MarkovaProf
Contributors OOK is the corresponding author who is responsible for the overall content as the guarantor, planned the study, organised the framework of the article, revised the manuscript and gave final approvement for the article. MVM organised the framework, collected the data and wrote the article. MOD collected the data and wrote the article. AOB was responsible for statistical analysis and wrote the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.