Article Text

Abstract
Background Parkinson’s disease (PD) is associated with perceived stigma and affects quality of life (QoL). Additional health conditions may influence these consequences of PD.
Aims This study assessed the impact of health conditions on perceived stigma and QoL in persons with PD. We hypothesised that individuals with more health conditions would report more stigma and poorer QoL. We also examined the contributions of demographic and clinical characteristics to the correlations between health conditions and perceived stigma/QoL.
Methods We identified 196 eligible participants from the Boston University Online Survey Study of Parkinson’s Disease and examined their health history, performance on multiple stigma measures, and scores on the 39-item Parkinson’s Disease Questionnaire assessing QoL.
Results At least one health condition was reported by 79% of the sample, with a median of 2 and a range of 0–7 health conditions. More perceived stigma and poorer QoL were associated with thyroid disease, depression, anxiety, and the total number of health conditions. These correlations were related to younger age, less education, and earlier disease onset. Other health conditions (high blood pressure, back/leg surgery, headache, cancer/tumours, and heart disease) were not significantly correlated with stigma or QoL.
Conclusions Having more health conditions, or thyroid disease, depression, or anxiety, was associated with more perceived stigma and poorer QoL, with younger age, less education, and earlier disease onset affecting the associations. It is important to consider the burden of health conditions and how they affect persons with PD with specific clinical characteristics.
- Psychiatry
- Depression
Data availability statement
Data are available on reasonable request to the corresponding author, subsequent to publication of data from the larger project.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Parkinson’s disease (PD) is associated with perceived stigma and affects quality of life (QoL), but little was known about the role of additional health conditions, which are common in people with PD.
What this study adds
More perceived stigma and poorer QoL were associated with thyroid disease, depression, and anxiety, as well as with a higher total number of additional health conditions.
These associations were related to younger age, less education, and earlier disease onset.
How this study might affect research, practice or policy
This study reveals the interaction of other health-related conditions with specific demographic and clinical features that may complicate the lived experience of persons with PD.
This is information of potential importance to care partners, healthcare professionals, and individuals with PD themselves.
Introduction
Parkinson’s disease (PD) is characterised by motor and non-motor symptoms that can significantly impact quality of life (QoL) and lead to the experience of stigma.1–3 The cardinal motor symptoms are resting tremor, rigidity, akinesia/bradykinesia, and impaired posture and gait, all of which may be readily visible and judged by others. Most persons with PD (PwPD) also experience non-motor symptoms that may affect QoL as much as motor symptoms and are also stigmatising.4–8 Often those who are diagnosed with age-related disorders, such as PD, have other health conditions, many of which are disorders of ageing and affect QoL.9 To improve the care that PwPD receive, it is important to identify which health conditions are most likely to increase the burden of perceived stigma and impaired QoL that arise from PD, and to identify which PwPD with these conditions are most likely to be affected.
Disease-related stigma is the experience of devaluation, discrimination, or discomfort that is self-perceived or other-perceived, and it occurs in PwPD.4–8 Self-perceived stigma occurs when an individual experiences negative attitudes about themselves often due to visible symptoms, such as facial masking, tremor, shuffling gait, or stooped posture, resulting in the self-acceptance of stereotypes, discrimination, and prejudice.2 8 Other-perceived stigma results from other people’s negative reactions to PwPD and can be influenced by cultural factors, as well as gender stereotypes, where women are judged more severely on symptoms due to societal pressures and expectations.5 7–11 In men with PD, younger age is associated with higher perceived stigma, possibly reflecting life adjustment to changes in social, family, and occupational roles.8 Stigma is also associated with mental health disorders,12 and studies have found a strong role of depression in stigma perception and compromised QoL in PD.7–13 PwPD may experience stigma associated with both motor and non-motor symptoms, which can affect their daily activities and interpersonal relationships.2 9 10 For example, facial masking and abnormal body movements further impair social well-being and social interactions among PwPD.11 14 In addition, stigma is a predictor of QoL, making it an important component of multiple health conditions.1 The Health Utility Index ranked heart disease, head injury, high blood pressure, and diabetes as severely impacting QoL, with cancer, thyroid disease, and back injuries having a moderate impact, but it did not assess neurodegenerative disorders.9 15
How individual health conditions affect perceived stigma and QoL is a question of interest, as many PwPD manage multiple health conditions. The purpose of the present study was to evaluate the impact of additional health conditions on perceived stigma and QoL in PwPD. We hypothesised that PwPD with more health conditions would experience more stigma and poorer QoL. We expected that depression would predict stigma perception and QoL, as reported previously,8 9 and we examined several other health conditions for such associations.5 10 13 We assessed whether there were significant correlations between stigma/QoL and demographic and clinical variables. Because common problems of PD-stigma research are limited sample size and lack of a validated, PD-specific stigma measure, we addressed these issues by conducting online assessments and using multiple published stigma scales from which we additionally derived a stigma composite.
Methods
Boston University Online Survey Study of Parkinson’s Disease (BOSS-PD)
The goal of BOSS-PD was to evaluate the experiences of PwPD. We recruited volunteer participants through advertisements in the Fox Trial Finder, Clinicaltrials.gov, and American Parkinson Disease Association websites, and other community outreach. Inclusion criteria for PwPD were diagnosis of PD without dementia, age of 40 years and above, proficiency in English, access to a computer, and ≥8 years of education. As the overall BOSS-PD aimed to study participants with a primary diagnosis of PD, exclusion criteria were active neoplasms, serious cardiac disease, other serious chronic medical illness, prior intracranial surgery, history of traumatic brain injury, psychiatric or neurological diagnoses other than PD, history of alcoholism or other drug abuse, or treatment with electroconvulsive therapy.
Consent was obtained via an online form before participants were given access to the Qualtrics-based survey. Participants then provided demographic and PD-related clinical information and health history, answering yes/no as to whether they had ever had the following health conditions: headache, stroke, high blood pressure, back/leg surgery, cancer/tumours, thyroid disease, heart problems, kidney problems, diabetes, lung problems, alcohol use disorder, substance abuse, seizures, electroconvulsive therapy, deep brain stimulation, mental retardation, or brain surgery.
After providing consent, participants responded to the BOSS-PD questionnaires. Those pertaining to the present study are described here.
Quality of life: Parkinson’s Disease Questionnaire-39 (PDQ-39)
This is a measure of QoL designed specifically for PD. There are 39 questions, including a four-item stigma subscore; higher scores indicate poorer QoL.16 The PDQ-39 and its stigma subscale have a high internal consistency measured by Cronbach’s α, as 0.63 and 0.88, respectively. Convergent validity has been measured with moderate correlations between the PDQ subscales and assessments of health on the 36-item Short Form Health Survey (SF-36) that fell between r=−0.31 and r=−0.88.17
Stigma perception
The Stigma Scale for Chronic Illnesses (SSCI) assesses stigmatisation across various health conditions, with high internal consistency measured by Cronbach’s α of 0.97.18 The Stigmatization Scale (Harvey) evaluates stigma experienced by groups of people, such as members of minority groups, with an emphasis on social stigma and alienation.19 The internal consistency of the Harvey Scale was measured by Cronbach’s α of 0.94, and construct validity was measured by finding correlations with self-report of stigmatisation, such as powerlessness (r=0.33) and self-esteem (r=0.34).19 The Mental Health Consumers’ Experience of Stigma Scale (Wahl) assesses the stigma experienced by those with mental health disorders.20 High internal consistency of the Wahl scale was measured by Cronbach’s α of 0.63 and concurrent validity was found with moderate correlations to QoL (r=−0.33) and psychiatric symptoms (r=0.31).21 We evaluated each of these scales, together with the stigma subscale of the PDQ-39, with respect to health conditions. We also constructed a stigma composite by converting the participant’s score on each of the four stigma scales to a z-score based on the means of the sample and summing the z scores. Higher scores on the stigma measures indicate more perceived stigma.
Non-motor symptoms: Non-Motor Symptoms Questionnaire (NMSQ)
This lists PD non-motor symptoms for endorsement (yes/no), including neuropsychiatric, sleep, gastrointestinal, sensory, and autonomic symptoms.22
Motor symptoms
Participants were asked if they experienced specific motor symptoms (yes/no): tremor, rigidity, speech difficulties, masked facial expression, balance/posture, or dyskinesia. If they answered ‘yes,’ they received the following questions: (1) (BOSS-PDmotor): ‘How unpleasant do you consider your motor symptoms?’ (1=Not at all; 2=Mildly: They do not bother me much; 3=Moderately: They are very unpleasant, but I can stand them; 4=Severely: I can barely stand them); and (2) (BOSS-PDm-ADL): ‘Does your motor symptom affect your ability to engage in activities of daily living (ADL)?’ (ADL) (1=Never, 2=Rarely; 3=Sometimes; 4=Often; 5=Always). Total scores represented the sum of the six motor symptom ratings.
Non-motor and motor experiences of daily living: Movement Disorders Society Unified Parkinson Disease Rating Scale (MDS-UPDRS)
This is a standard measure of PD severity. We administered Parts I and II, respectively, the non-motor and motor aspects of experiences of daily living.23
Depression: Beck Depression Inventory-II
This is a 21-item self-report assessment of depression symptom severity on a scale of 0–3.24 A score of 14 or more is suggestive of clinical depression in PD.25
Anxiety
We included two widely used self-report scales to assess anxiety. Beck Anxiety Inventory (BAI) is a 21-item measure of symptom severity on a scale of 0–3.26 Parkinson’s Anxiety Scale (PAS) is a 12-item measure using a scale of 0–5.27 For both, scores of 13 or more are suggestive of clinical anxiety in PD.27 28
Statistical analyses
For analysis, we included only those health conditions that were endorsed by at least 10% of the sample (20 participants) for power purposes. We used t-tests to examine whether gender affected the clinical variables. We used point-biserial correlations to assess the association of a health condition (presence/absence) with stigma (for each scale plus composite) and with QoL (PDQ-39 total score). A p value of 0.01 was used to account for multiple comparisons; p>0.01 and <0.05 was considered a trend. Analysis of covariance (ANCOVA) was performed with independent variables being health conditions (ie, between those who reported depression vs those without depression) that were significantly associated with the dependent variables of stigma and QoL measures (ie, PDQ, SSCI, etc), to examine the influences of demographic (age, gender, education) and clinical covariates (age at PD onset, PD duration, motor symptoms (BOSS-PDmotor, BOSS-PDm-ADL, Movement Disorders Society Unified Parkinson Disease Rating Scale (MDS-UPDRS) Part II) and non-motor symptoms (NMSQ, MDS-UPDRS Part I)). Partial eta squared values were reported for the ANCOVAs, alongside the p values, as a measure of effect size. To limit the number of analyses, we chose the one stigma measure that most strongly correlated with each health condition. Another ANCOVA was similarly performed for each health condition that was significantly associated with the QoL measure, PDQ-39 total. We used ANCOVAs instead of regressions in our analyses, as many of the covariates were categorical variables and ANCOVAs allowed for more efficient analyses and interpretation of the data. For ANCOVAs, a p value of 0.01 was used to account for multiple comparisons; p>0.01 and <0.05 was considered a trend.
We categorised depression and anxiety as health conditions rather than as clinical characteristics, using the accepted cut-off scores for each scale to categorise PwPD as depressed/anxious or not. Hence, although the data on depression and anxiety were from the scales, whereas the data from the other health conditions were from yes/no endorsement responses, all were dichotomised in the same way and treated the same way in the analyses.
Results
Participants
Participants included 196 individuals (113 women, 81 men, 2 unspecified; age range 43–84 years old; education range 10–21 years). Table 1 provides demographic and clinical characteristics and scores on the stigma/QoL measures for the entire sample and for men and women separately. There were no differences between men and women on any demographics or the clinical, QoL, or stigma scores.
Participant characteristics, mean (SD)
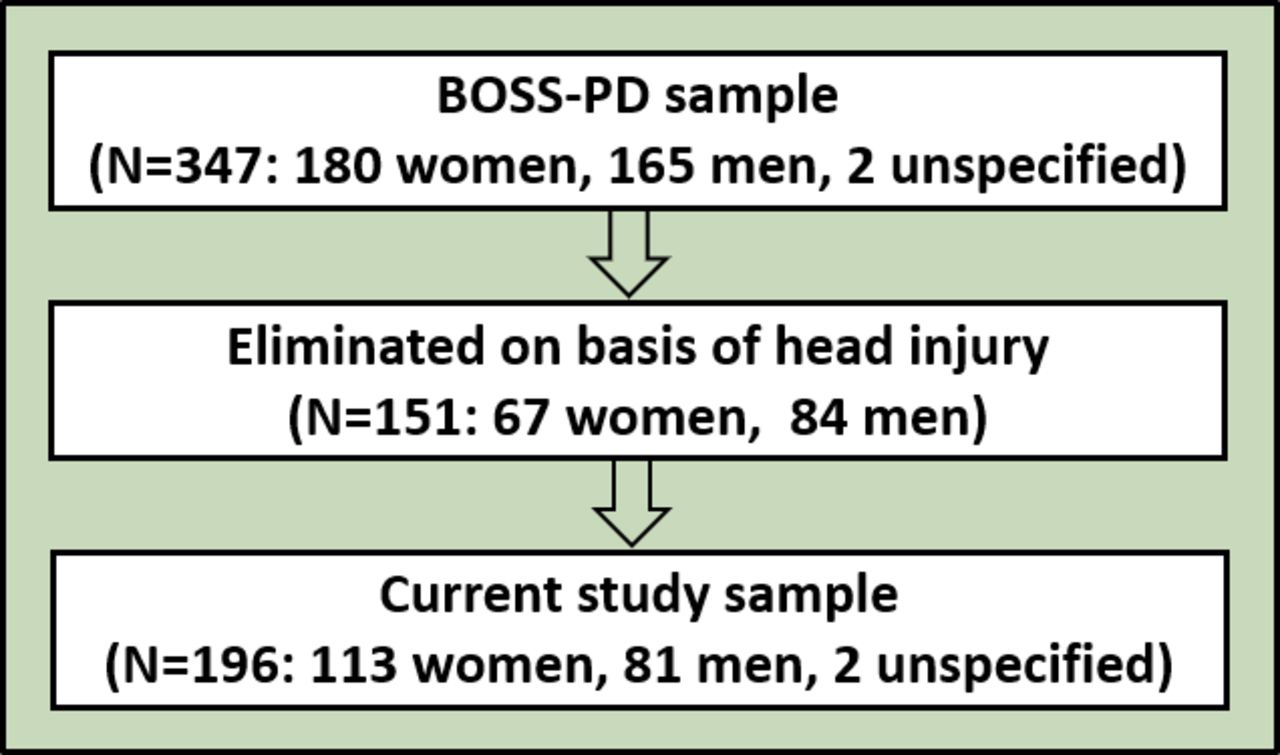
These participants were drawn from a larger sample of 347 who originally completed the BOSS-PD (figure 1). On the health history section of the survey, many potential participants endorsed ‘blow to the head,’ ‘loss of consciousness,’ or ‘concussion,’ although a history of traumatic head injury (with no further description) was an exclusion criterion. These individuals were consequently deemed ineligible. We retained participants who endorsed depression or anxiety for a number of reasons: many individuals may not recognise that depression and anxiety, which are common in PD, are psychiatric diagnoses, especially those with mild symptoms; a wide range of depression/anxiety symptom severity was represented in the current sample; and stigma was related to depression in an in-person sample of PwPD.8 Hence, we felt it was important to evaluate depression and anxiety in relation to stigma and QoL in the current sample, especially in light of its relatively large number of women, who are generally understudied in PD.

{kind=link}
Study flowchart. BOSS-PD, Boston University Online Survey Study of Parkinson’s Disease.
Prevalence of health conditions
The prevalence of health conditions reported by at least 10% of the PD sample was described in table 2 (entire sample, women, men). Of the sample of 196, 79% (155 in total, 91 women, 62 men, 2 unspecified) reported at least one health condition. High blood pressure was the most reported health condition, endorsed by 68 participants (35%). Conditions endorsed by less than 10% of the sample included kidney disease (13), diabetes (8), lung diseases (8), seizures (3), alcoholism (3), substance use disorder (3), stroke (1), brain surgery (1), electroconvulsive therapy (1), mental retardation (0), and deep brain stimulation (0). Participants reported a median of 2 health conditions with a range of 0–7: 41 PwPD had none, 48 had one, 48 had two, 25 had three, 21 had four, 6 had five, 5 had six, and 2 had seven, with no differences by gender.
Prevalence of health conditions in total sample and in women and men
More women than men reported thyroid disease (χ2=17.6, p<0.001). No other health conditions showed significant differences in the prevalence between men and women.
The prevalence of health conditions in our BOSS-PD sample was variable relative to the larger population of older adults. According to a US-based study by He and colleagues of two large samples (40 087 and 147 900 individuals aged 65 or above),29 the prevalence was similar for thyroid disease (19%–20%; BOSS-PD: 19%), and for having two or more chronic conditions (81%–83%; BOSS-PD: 79%), whereas high blood pressure (81%–84%), heart disease (38%–39%, ischaemic) and cancer (summed prostate, breast, colorectal, lung, endometrial; prevalence 19%–20%) were under-represented in our sample (BOSS-PD: 35%, 12%, 15%, respectively), likely reflecting that many participants in our sample were younger than age 65. By contrast, depression (14%–15%) was somewhat over-represented in our sample (BOSS-PD: 18%), reflecting the known high prevalence of depression in PD. The study by He and colleagues did not report on other conditions that we assessed in our sample.
Stigma composite, stigma scales, QoL and relation to participant characteristics
For the entire sample, Pearson’s correlations between the stigma composite score and the individual stigma scales were strong: SSCI (r=0.74, p<0.001), PDQ stigma subscale (r=0.68, p<0.001), Wahl Scale (r=0.59, p<0.001) and Harvey Scale (r=0.62, p<0.001). There was also a strong correlation between the total PDQ-39 and the stigma composite score (r=0.59, p<0.001). There was significant intercorrelation of scores on the stigma measures, justifying the use of the stigma composite. SSCI scores correlated with PDQ-stigma (r=0.60, p<0.001), Wahl (r=0.41, p<0.001) and Harvey (r=0.23, p<0.001); PDQ-stigma correlated with Wahl (r=0.30, p<0.001) and Harvey (r=0.14, p<0.001); Wahl correlated with Harvey (r=0.26, p<0.001).
The stigma composite score was significantly affected by younger age (r=−0.27, p<0.001; more stigma with younger age), younger age at disease diagnosis (r=−0.35, p<0.001), and longer disease duration (r=0.23, p=0.001), but not with gender or education level. It also correlated with higher scores on the MDS-UPDRS Part I (r=0.32, p<0.001) and Part II (r=0.36, p<0.001), more non-motor symptoms on the NMSQ (r=0.19, p=0.008), more motor symptom unpleasantness (BOSS-PDmotor; r=0.29, p<0.001), and more motor symptom impairment on daily activities (BOSS-PDm-ADL; r=0.34, p<0.001).
Relation of health conditions to stigma/quality of life
For the following health conditions only, there were significant correlations with one or more stigma scores or with the PDQ-39 total score. The results were shown in table 3 and summarised below. In general, the highest correlations for the stigma scales occurred for the SSCI.
Correlations (r) between health conditions and quality of life/stigma scores
Thyroid disease endorsement correlated with worse QoL on the PDQ and more stigma perception on the SSCI (p values<0.01) plus a trend on the stigma composite.
Depression endorsement correlated with worse QoL, more stigma perception per the composite score, and two stigma scales: SSCI and PDQ stigma subscale (all p values<0.001).
Anxiety endorsement, per BAI, showed moderate correlations with worse QoL and more perceived stigma: composite score, SSCI and PDQ stigma subscale, as well as a trend for the Wahl and Harvey. Anxiety per PAS was correlated with worse QoL and more perceived stigma: composite score, SSCI and PDQ stigma subscale (all p values<0.001), as well as a trend for the Wahl.
The total number of health conditions was related to poorer QoL and more stigma on the composite score and SSCI (all p values<0.001).
There were no significant differences in stigma perception or QoL between those who did and did not endorse high blood pressure, back/leg surgery, headache, cancer/tumours, or heart disease, using the planned alpha of 0.01 (all r values≤0.14, all p values>0.024).
Influence of demographic and clinical variables on the relation between health conditions and stigma/quality of life
To examine whether the above correlations between health conditions and stigma/QoL were driven by demographic or clinical variables, two ANCOVAs (using p of 0.01) were conducted for each health condition: thyroid disease, depression, anxiety per PAS (BAI showed similar results), and the total number of health conditions; one for QoL (PDQ-39 total) and the other for stigma (SSCI for thyroid disease, depression, anxiety, and total health conditions). We selected the SSCI for the ANCOVA regarding stigma because, as noted above, scores on this scale alone were significantly correlated with the endorsement of each one of the health conditions (thyroid disease, depression, anxiety) and with total health conditions. The results were in table 4 and summarised below. All health conditions were still significantly associated with QoL and stigma after controlling for clinical, demographic, and motor and non-motor variables.
ANCOVA F-values (P, effect sizes—partial eta squared) per clinical/demographic variables
Thyroid disease
Quality of life
Thyroid disease was significantly associated with QoL when controlling for clinical, demographic, and motor and non-motor variables. Additionally, younger age, less education, younger age of PD onset, more severe symptom-related impairment on the MDS-UPDRS Parts I, II, BOSS-PDmotor, more non-motor symptoms on the NMSQ, and more frequent symptoms on the BOSS-PDm-ADL were significantly associated with poorer QoL. Gender and disease duration were not significantly associated with QoL (PDQ-39).
Stigma
Thyroid disease was significantly associated with stigma when controlling for clinical, demographic, and motor variables. Additionally, younger age, less education, younger age of PD onset, more severe symptom-related impairment on the MDS-UPDRS Parts I, II, BOSS-PDmotor, and more symptoms on the BOSS-PDm-ADL were significantly associated with stigma (SSCI). Gender, disease duration, and non-motor symptoms (NMSQ) were not significantly associated with stigma. It should be noted that very few men (5%) endorsed thyroid disease, whereas 30% of women did.
Depression
Quality of life
Depression was significantly associated with QoL when controlling for clinical, demographic, and motor and non-motor variables. Additionally, being female, having less education, younger age of PD onset, more severe symptom-related impairments on the MDS-UPDRS Parts I and II and BOSS-PDmotor, more frequent impairment by motor symptoms on BOSS-PDm-ADL, and more symptoms on the NMSQ were significantly associated with QoL (PDQ-39). Age and disease duration were not significantly associated with QoL.
Stigma
Depression was significantly associated with stigma when controlling for clinical, demographic, and motor variables. Additionally, younger age, less education, earlier disease onset, and more severe symptom-related impairments on the MDS-UPDRS Part I and II were significantly associated with stigma (SSCI). Gender, disease duration, non-motor symptoms (NMSQ), self-reported motor symptom unpleasantness (BOSS-PDmotor), and motor symptom impairment (BOSS-PDm-ADL) were not significantly associated with stigma.
Anxiety
Quality of life
Anxiety was significantly associated with QoL when controlling for clinical, demographic, and motor and non-motor variables. Additionally, less education, younger age of PD onset, more severe symptom-related impairments on the MDS-UPDRS Parts I, II, and BOSS-PDmotor, more impairment by motor symptoms on BOSS-PDm-ADL, and more symptoms on the NMSQ were significantly associated with worse QoL (PDQ-39). Age, gender and disease duration were not significantly associated with QoL, although there was a trend toward an association between anxiety and QoL in women.
Stigma
Anxiety was significantly associated with stigma when controlling for clinical, demographic, and motor variables. Additionally, younger age, less education, earlier disease onset, and more severe symptom-related impairments on the MDS-UPDRS Parts I and II and BOSS-PDmotor were significantly associated with stigma (SSCI), and there was a trend toward this association with BOSS-PDm-ADL. Gender, disease duration, and non-motor symptoms (NMSQ) were not significantly associated with stigma.
Total number of health conditions
Quality of life
The total number of health conditions was significantly associated with QoL when controlling for clinical, demographic, and motor and non-motor variables. Additionally, younger age, less education, younger age of PD onset, more severe symptom-related impairments on the MDS-UPDRS Parts I and II and BOSS-PDmotor, more impairment by motor symptoms on BOSS-PDm-ADL, and more symptoms on the NMSQ were significantly associated with QoL (PDQ-39). Gender and disease duration were not significantly associated with QoL.
Stigma
The total number of health conditions was significantly associated with stigma when controlling for clinical, demographic, and motor variables. Additionally, younger age, less education, younger disease onset, and more impairments related to motor and non-motor symptoms on the MDS-UPDRS Part I, Part II and BOSS-PDmotor were significantly associated with stigma (SSCI), and there was a trend toward this association with BOSS-PDm-ADL. Gender and disease duration, non-motor symptoms (NMSQ) were not significantly associated with stigma.
Discussion
Main findings
Of the 196 eligible PwPD who participated in this online survey regarding their experiences living with PD, the large majority (79%) reported one or more health conditions. We found that health conditions impacted the perception of stigma and QoL. As predicted, a higher number of health conditions was significantly related to higher stigma perception and lower QoL. We also found higher perceived stigma/poorer QoL for the specific health conditions of thyroid disease, depression, and anxiety. For PwPD with each of these conditions, higher levels of perceived stigma or worse QoL were associated with younger age, less education, younger age at PD onset, more impairment on ADLs per the MDS-UPDRS Parts I and II, more non-motor symptoms on the NMSQ, and more motor symptoms/impact on daily living on the BOSS-PDmotor and BOSS-PDm-ADL. The relation of perceived stigma and QoL to depression in PD was anticipated based on previous literature.2 13 The close association of depression and anxiety in many psychiatric conditions and in PD likewise makes anxiety’s relation to perceived stigma and QoL readily interpretable. Thyroid disease’s association with stigma and QoL may reflect our sample’s relatively high representation of women. There is very little literature linking stigma to thyroid disease in particular, as opposed to head and neck cancers in general, and this topic clearly requires more investigation.
Two aspects of methodology distinguished our study from previous examinations of stigma and QoL in PD. First, we administered our assessment online in order to reach a large number of PwPD for this prospective study. Second, to examine stigma from multiple angles, we used four published stigma scales, and created a stigma composite from the individual scales, which was related to the effects of education and PD duration.
Regarding the online assessment, an advantage of this design was that it allowed us to collect data from a large sample with diverse health conditions. Women outnumbered men in the final sample, unlike in many in-lab studies of PwPD that have significantly more men, in part reflecting the elevated exclusion of men because of history of head injury (84 men excluded, 67 women). The study captured a wide range of ages (43–84 years) and education levels (10–21 years, although the mean education level was high). The sample was also heterogeneous regarding the clinical characteristics of age at onset, PD duration, and PD severity (from mild to severe). It was homogeneous with respect to race, however (mostly white).
Regarding the stigma measures, endorsement of thyroid disease was correlated with higher scores on the SSCI; depression and anxiety were correlated with scores on the SSCI and PDQ-stigma. The total number of health conditions was correlated with SSCI scores. Hence, in our sample of PwPD, the SSCI scale was most generally successful in picking up perceived stigma (related to thyroid disease, depression, anxiety, and total health conditions). It is not unexpected that the SSCI would be most sensitive to stigma in PD, as it was developed as part of a study of health-related QoL for persons with neurological disorders and its purpose is to assess stigma associated with chronic illnesses. Scores on the PDQ-39 stigma subscale correlated with those on the SSCI more strongly than with scores on the other two scales, but as the PDQ-39 stigma subscale comprised only four questions, the narrowness of scope may have led to it being less sensitive to stigma overall than the SSCI.
The Mental Health Consumers’ Experience of Stigma Scale (Wahl) and the Stigmatization Scale (Harvey) were not as sensitive as the others to the health conditions in question. Whereas the PDQ-39 is designed for persons with PD and the SCCI for those with chronic (neurological) illnesses, the Wahl Scale focuses more on general mental health associated stigma, and the Harvey Scale more on social and racial stigma. There was a trend toward correlations between endorsement of anxiety and scores on the Wahl (both measures) and Harvey (BAI), with p<0.05 and therefore not at the level of our conservative alpha of 0.01. The weaker strength of the relation with the Wahl may have reflected it being a more general measure of mental health than the more specific SSCI (chronic, neurological) and PDQ-39 (PD specifically). Regarding the Harvey, the large majority of our sample identified as white and not Hispanic and therefore presumably did not experience stigma based on race or ethnicity, although they may have experienced social stigma. Although it was less sensitive than the other scales to stigma in our sample, the Harvey may possibly be useful in a more diverse sample of individuals with PD.
Limitations
The limitations of our study are mainly those seen in much health survey research. All of our measures were self-report. Participants may have been unreliable in their reporting of health conditions, in part because there was potential overlap in symptoms for some of the listed health conditions, especially common ones such as heart disease and high blood pressure. There were also exclusion criteria that may have been missed, misinterpreted, or ignored by participants. For example, many participants reported head injury in their health history and consequently were removed from the study. (See the "participants" section of "results" for our justification for retaining those with depression or anxiety; we nevertheless acknowledge that some potential participants decided not to take the survey based on the psychiatric exclusion criterion, possibly affecting the generalisability of the results.) Certain groupings may have led us to miss the unique impact of particular conditions; for example, many different heart-related issues (coronary artery disease vs arrhythmias) might qualify as ‘heart disease’ but have different effects on stigma and health. Our list of possible health conditions, while extensive, was not exhaustive. Because the objective of this study was not to examine the prevalence of health conditions in PD, but rather their relation to stigma perception and QoL, this sampling issue was probably not of importance here, although it could be pertinent to other online studies. We did not evaluate cognition in this study, and hence we cannot comment on how stigma perception and QoL are related to cognitive problems that are associated with PD and PD-related dementia.30 We did not consider the duration or severity of the health conditions, nor whether they were past or current, which may have been related to perceived stigma and QoL. A further limitation is that our sample was mostly white; stigma and QoL may be experienced differently in non-white groups. Based on the results of this study, future research may consider the nuances of the relation of health conditions to the experience of stigma and QoL in PwPD and include a more diverse sample.
Implications
In conclusion, we found that additional health conditions in PwPD were associated with more perceived stigma and poorer QoL. When evaluating stigma and QoL in PD, it is important to consider the burden of health conditions and how they might be affecting PwPD. Individual health conditions, which may arise at different points in the ageing process, could have different effects at various stages of PD. Demographic variables such as age, sex, and race/ethnicity, and clinical variables such as disease severity, may also affect the relation between health conditions and stigma, as individuals from particular groups are at higher risk for having specific chronic conditions or more total health conditions, leading to more stigma perception and lower QoL. This study raises awareness of the complex interaction of other health-related conditions with demographic and PD clinical features that may complicate the lived experience of PwPD. This is information of potential importance to care partners, healthcare professionals, and individuals with PD themselves.
Data availability statement
Data are available on reasonable request to the corresponding author, subsequent to publication of data from the larger project.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Boston University Institutional Review Board, protocol #1204E. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to all of the participants in this study. We also thank the members of the BOSS-PD research team, especially Ryan Piers, Rini Kaplan, and Celina Pluim, for helpful discussions regarding this subproject, and Amie Larum and Luis Dominguez for survey and database development.
References
Samia Islam graduated from Boston University in the USA in 2020 with a BA and Honors in Psychology where she focused on studying cognition and its neural correlates in Parkinson’s and Alzheimer’s disease. She received her MA in Biotechnology from Columbia University in the USA in 2021 where she studied the mouse models of Alzheimer's disease. She is currently a Psychology PhD student at the University of Illinois-Urbana Champaign with a focus on Cognitive Neuroscience. Her main research interests include the cognitive aging and arterial stiffening associated with both healthy and diseased brain states using multiple neuroimaging modalities, including fMRI and optical imaging.

Footnotes
Twitter @ACroninGolomb
Contributors SSI: Research project—conception, organisation, execution; analysis—execution; manuscript—writing of the first draft.
SN: Research project—conception, organisation; analysis—design, review and critique; manuscript—review and critique.
SBK: Research project: conception, organisation; analysis—design; manuscript—review and critique.
JTF: Research project—conception; analysis—design, review and critique; manuscript—review and critique.
RDS: Research project—conception, organisation; analysis—review and critique; manuscript—review and critique.
ACG: Research project—conception, organisation; analysis—design, review and critique; manuscript—review and critique. ACG acts as guarantor.
Funding ACG was employed at Boston University, Boston, Massachusetts, USA. She has received funding on grants from the American Parkinson’s Disease Association, NIH U01 EB029856 (PIs Boas, Kiran), R01 AG063775 (PI Reinhart), NIH R01 AG050595 (PIs Lyons, Kremen), the Boston University Alzheimer’s Disease Center, and the Swiss National Science Foundation. She received compensation for editorial service for the journal Psychological Science.
Competing interests SSI was a student at Boston University, Boston, Massachusetts; Columbia University, New York, New York; and University of Illinois Urbana-Champaign, Champaign, Illinois. SN was employed at Bridgewater State University, Bridgewater, Massachusetts. SBK was a student at Boston University, Boston, Massachusetts. JTF was a student at Boston University, Boston, Massachusetts. He was funded on NIA research grant 1 F31AG062158. RDS was employed at Tewksbury Hospital, Tewksbury, Massachusetts.
Provenance and peer review Not commissioned; externally peer reviewed.