Article Text

Abstract
Background Displaced persons in Nigeria experience various difficulties at different stages of their displacement, including mental and physical problems. These experiences have been associated with different types of mental disorders.
Aims This study sought to identify sociodemographic correlates and other factors associated with depression and anxiety among internally displaced adults in Ogoja, Cross River State, Nigeria.
Methods A cross-sectional study was conducted using non-probability and probability sampling techniques. Internally displaced adults (n=335) were identified in Ogoja locations with a high prevalence of internally displaced persons (IDPs). Their mental health symptoms were assessed using the Common Mental Disorder Questionnaire, and a semistructured questionnaire was employed to collect data on sociodemographic and displacement-related characteristics. Data were analysed using descriptive statistics, χ2 analysis and multivariable logistic regression.
Results The prevalence of subtypes was 66.0% for anxiety disorder and 73.4% for depression. Factors found to be significant in each bivariate χ2 analysis were modelled for each outcome. The multivariate analysis revealed that prolonged displacement (adjusted odds ratio (AOR)=3.64; p=0.048), reduced family size (AOR=0.28; p<0.001) and fears of reprisal attacks (AOR=4.19; p=0.004) were significantly associated with anxiety disorder. Male gender (AOR=2.09; p=0.015), prolonged displacement (AOR=3.55; p=0.020), reduced family size (AOR=0.55; p=0.049), financial strain (AOR=5.43; p=0.023) and loss of loved ones (AOR=1.92; p=0.040) were significantly associated with depression.
Conclusions The implications of the findings underline the complex aetiology of these two mental problems and the need to cater to the well-being of those at risk who have been exposed to trauma-related events. Accessible and affordable mental health services should be provided for these persons while also considering a social welfare scheme that covers their health expenses. Moreover, socioeconomic conditions targeting IDPs in the Ogoja Local Government Area should be improved by conducting large-scale mapping to identify this population.
- depression
- anxiety
- mental health
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Data are not publicly available but can be made available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
There is an increased prevalence of mental disorders among people in conflict-affected settings.
What this study adds
Prolonged displacement, reduced family size and fears of reprisal attacks are significantly associated with anxiety disorder. Male gender, prolonged displacement, reduced family size, financial strain and loss of loved ones are significantly associated with depression.
How this study might affect research, practice or policy
The implications of the findings underline the complex aetiology of these two mental problems and the need to cater to the well-being of those who are at risk and have been exposed to trauma-related events.
Introduction
Wars and natural disasters cause an upsurge in the displacement of individuals and communities within a larger society. Reports indicate over 33 million persons were displaced globally in 2019 due to them.1 This number is a follow-up to the 2018 data that revealed about 28 million persons were internally displaced for the said year globally. Internal displacement occurs in various forms. The Global Report on Internal Displacement suggests that armed conflicts, general violence, human rights violations, political wars, poverty, inequalities, poor governance and climate change are the main drivers of displacement globally.1 The report also holds that a single reason does not trigger displacement; a pile-up of occurrences that build up over an extended period can bring about unwanted circumstances leading to disruptions in everyday life, religious practices, cultural customs, occupation, means of livelihood, and so on. Terrorism, originating mainly in the northern enclaves of Nigeria, has led to the increased displacement of over two million persons and the deaths of over 350 000 persons.1 Consequently, Nigeria ranks among the top 10 most terrorised countries in the world. The outcomes of insurgency have led to massive migration to neighbouring countries in and around sub-Saharan Africa, magnifying socioeconomic displacement-related consequences.2 The ripple effects of massive migrations cannot be overemphasised.
The United Nations High Commissioner for Refugees (UNHCR) has suggested that many internally displaced persons (IDPs) in Nigeria have expressed their willingness to be re-integrated into their ancestral abodes. Still, they have met obstructions such as heightened insecurity, secondary displacements, and inaccessible healthcare, nutrition and shelter. These constraints are not limited to IDPs alone but also affect the United Nations staff who have been forcefully blocked from the most affected communities, such as those in north-eastern Nigeria. Consequently, rebuilding plans have been thwarted, supplies of palliatives are limited and the provision of healthcare is inadequate. By right of citizenship, IDPs are entitled to better legal protection from their country than that offered to refugees and asylum seekers who have fled their homeland.3 However, in most settings, refugees have attracted more support than IDPs over the years. This disparity has negatively affected the long-term psychological health of IDPs who reside in host communities because they have been deprived of essential healthcare.3
In addition, psychological ailments and mental disorders are more common among displaced persons exposed to the trauma of wars and disasters.3 This condition is further aggravated when these traumatised IDPs migrate to communities without social and healthcare facilities. Researchers in one study4 argued that global public health systems are slow to meet these vulnerable groups’ rapidly emerging psychological needs, particularly in poor-resource countries. Potential reoccurring effects of poorly treated psychological problems include exacerbated physical illnesses, social withdrawal and psychological distress.4 Migration triggers myriad social and cultural issues; inadequate responses from host communities and battles over scarce resources increase the population’s risk for diverse health problems.5
Generally, displaced persons are recognised as suffering from common mental disorders (CMDs), most notably depressive episodes and anxiety.6 Odusanya5 further stated that the solution to tackling the health problems of displaced persons lies in conflict resolutions through a multidimensional approach of good governance, provision of basic and social amenities, and diplomacy. Another method emphasises emergency preparedness, including an adequate health infrastructure, and providing financial and human resources to reach the gradually growing population of affected states and communities with essential healthcare needs. Women and children are the groups most severely affected by conflicts and disasters, making up the highest proportion of the displaced population in sub-Saharan Africa.7 The UNHCR further reported the undesirable rise in vulnerability among households in conflict-affected areas. Out of more than 32 000 vulnerable households and over 36 000 vulnerable individuals profiled by the UNHCR’s vulnerability screening in Nigeria, 18.68%, 33.28% and 48.66% were profiled as orphans, women-headed households and households headed by the elderly, respectively.7
Accordingly, this study was essential to bolster existing studies of the plights of IDPs in Nigeria. The study engaged a full-scale assessment of two mental health conditions commonly found among IDPs and sought to identify key predictors of these disorders. Operationally, two hypotheses were formulated to guide the study:
There is no statistically significant relationship between sociodemographic factors (age, gender, educational attainment, financial standing, occupation, family size and displacement duration) and depression and anxiety among internally displaced adults in Ogoja’s Cross River State displacement settlements.
There is no statistically significant relationship between displacement-associated factors (life events, socioeconomic factors) and depression and anxiety among internally displaced adults in Ogoja’s Cross River State displacement settlements.
Methods
Scope of the study
This study aimed to explore sociodemographic correlates of depression and anxiety with associated factors such as adverse life events among IDPs adults 18 years or older who had been displaced due to natural disasters (flooding, wind and hail storms, rock and landslides, and so on) or man-made disasters (communal conflicts, insurgency, and so on) in the hard-to-reach Ogoja Local Government Area (LGA) of Cross River State. The data for this research were collected only from indigenes of Nigeria who had attained displacement status and resided in host communities in Ogoja.
Study design
This cross-sectional descriptive study used a quantitative approach to determine the sociodemographic correlates and associated factors of anxiety and depression among IDPs in Ogoja LGA of Cross River State.
Study population
The study population comprised adults 18 years and older living in IDPs settlements in Ogoja LGA of Cross River State.
Sample size determination
The sample size for this study was determined using Fischer’s formula as cited in Kish8 for estimating the sample size for a cross-sectional study.

Where n is the sample size
Z is 1.96 (at 95% confidence interval (CI))
p=0.64 (previous proportion of IDPs with CMDs in Benue State, Nigeria)3
q or 1-p=0.36 (proportion of IDPs without CMDs)
d=0.05 (acceptable margin of error for proportion being estimated)
Therefore
With N=4600, applying finite population correction for population less than 10 000:

Where n=calculated sample size and N=study population.
Therefore

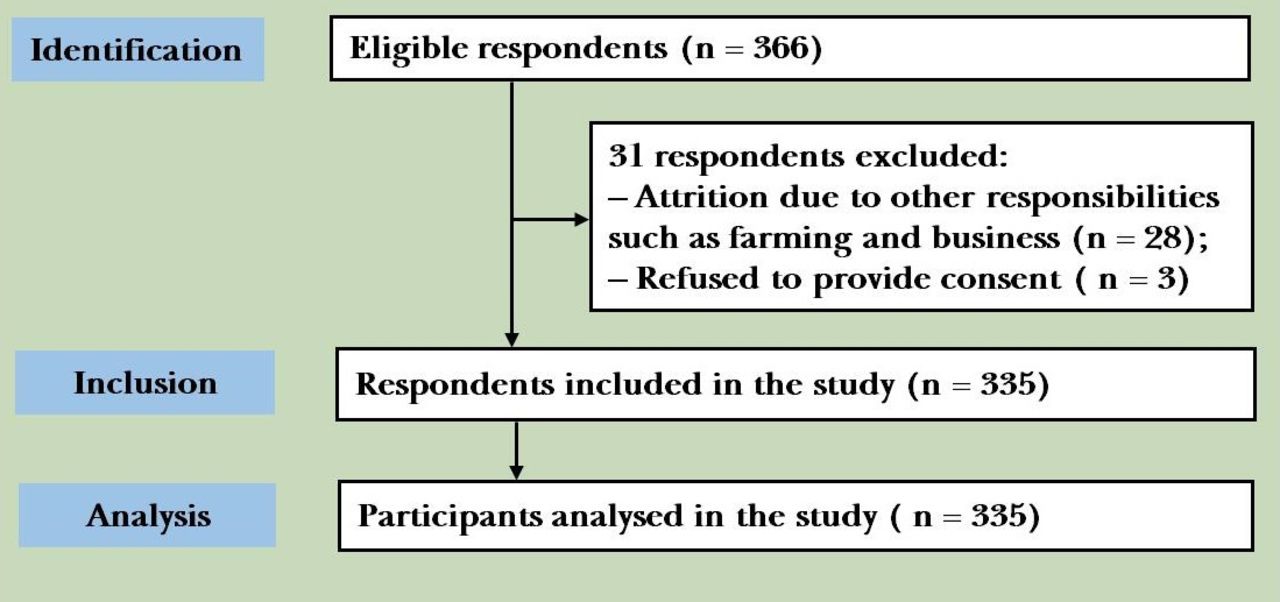
Adjusting for perceived non-response rate of 10%, 366 respondents were recruited to measure the study outcomes within 5% precision and a 95% CI (see figure 1).
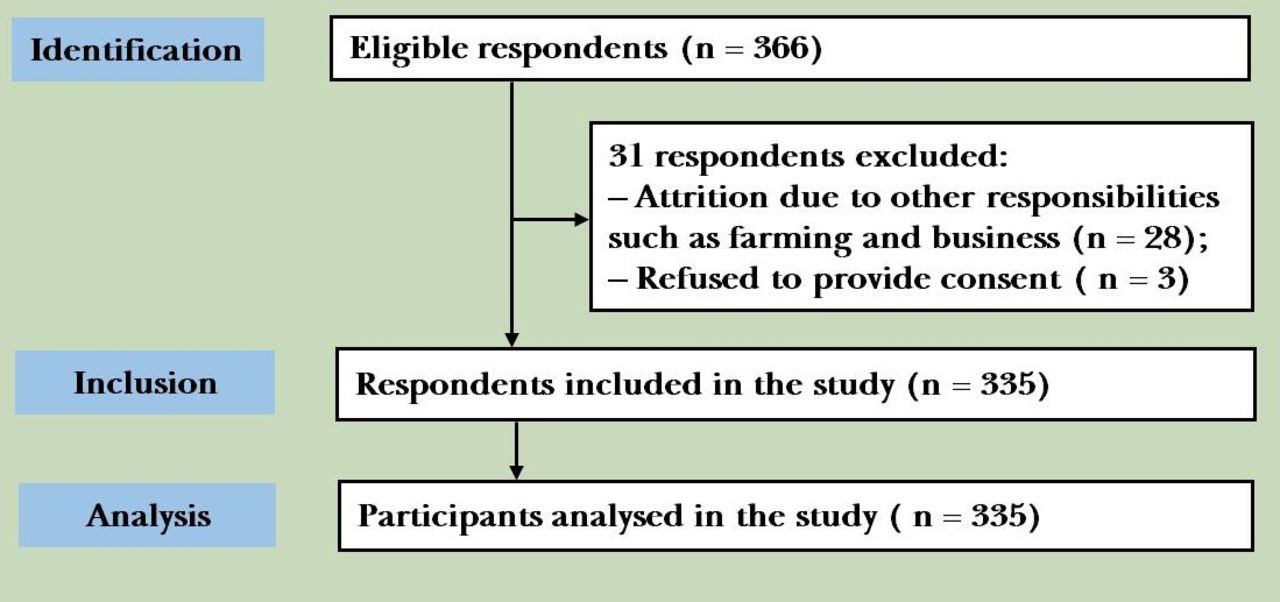
Selection of respondents for the study on sociodemogtaphic correlates and associated factors of depression and anxiety among internally displaced adults in Ogaja Local Government Area, Cross River state, Nigeria.
Sampling procedure
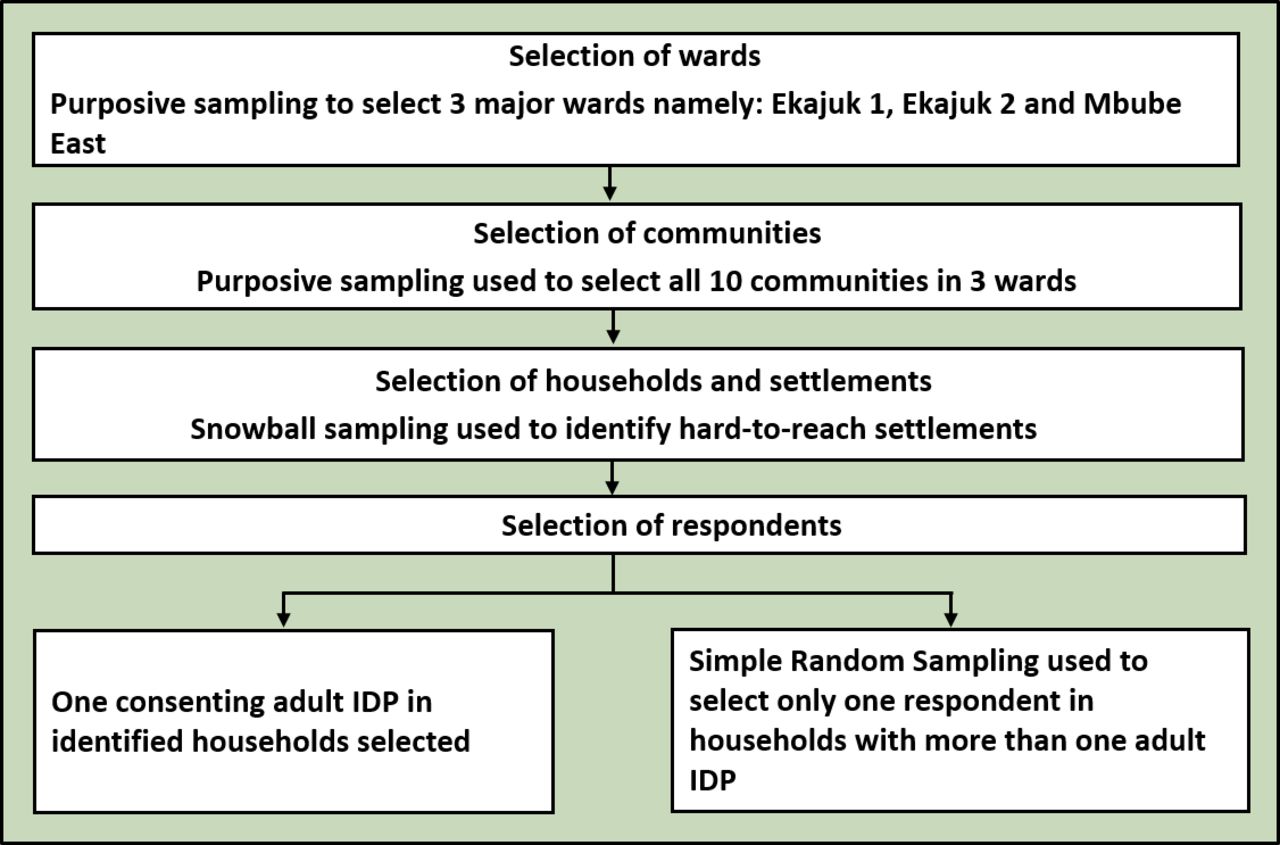
A multistage sampling technique was employed in the selection of study participants with the following procedures:
Stage 1: Selection of wards
With the displaced persons residing in host communities without a central settlement, purposive sampling was used to select three wards, primarily housing IDPs in Ogoja. Out of the 10 wards in Ogoja LGA, three wards, namely Ekajuk I, Ekajuk II and Mbube East have particularly had an influx of displaced persons and were selected for this study.
Stage 2: Selection of communities
Ekajuk I and II have seven communities between them while Mbube East has three major communities (Ogberia, Ojerim and Oboso).9 Purposive sampling was used to select all 10 communities of the three wards.
Stage 3: Selection of households and settlements
To identify households or settlements where IDPs reside, a snowball sampling technique was used.
Stage 4: Selection of respondents
Only one adult IDP in each household who consented to participate was recruited. Where there was more than one adult IDP in each household, a simple random sampling technique of balloting without replacement was used to select one adult IDP (see figure 2).

{kind=link}
{kind=link}
Flowchart for the study on sociodemographic correlates and associated factors of depression and anxiety among internally displaced adults in Ogoja Local Government Area, Cross River State, Nigeria. IDP, internally displaced person.
Instruments for data collection
A semistructured questionnaire was employed in the collection of sociodemographic information of respondents and factors associated with these disorders in the setting.
A Common Mental Disorder Questionnaire which has been identified by Christensen et al10 to have demonstrated good diagnostic accuracy and exceptional external validity in primary care settings is a 36-item questionnaire that covers signs and symptoms generally linked with five mental disorders. For the purpose of this research, the depression and anxiety subtype sections were adopted and used for diagnosis. Each question of the depression and anxiety section is rated on a five-point Likert Scale of distress with responses ranging from ‘not at all’ to ‘extremely’ (0–4).
Method of data collection
Data were collected with the aid of two trained research assistants who, due to the nature of this research, were health professionals. Their recruitment was also based on their knowledge of the local dialects and navigation within the study area. Semistructured questionnaires were used. All the questionnaires mentioned above were interviewer-administered using Open Data Kit (ODK) collect software. ODK is a mobile data collection tool linked with an electronic database for data collection and processing. The researchers used the Kobo toolbox online database for the needed linkage with ODK collect.
Method of data analysis
Data were extracted from ODK collect and downloaded into Microsoft Excel. All data were scanned for entry completeness and entered using Microsoft Excel. Data were then transferred to Statistical Package for the Social Sciences (SPSS) V.23 for analysis. All responses were dichotomised between ‘not at all’ and ‘a little’ as validated by Christensen et al.10 This entails that all positive responses between ‘a little’ and ‘extremely’ were recoded and counted as ‘1’ while ‘not at all’ remained ‘0’. Cut-off points for case identification in each subscale were determined by the use of standardised theoretical optimal cut-off points regarding sensitivity, specificity, positive predictive value and negative predictive value.10 A sum score of 3 or more in the depression subscale depicts a depression diagnosis with a sensitivity and a specificity of 78% and 86% respectively; a sum score of 3 or more in the anxiety subscale depicts an anxiety diagnosis with a sensitivity and a specificity of 77% and 85% respectively. Sociodemographic characteristics (‘reason for displacement’ was excluded from following analyses because at their discretion, the authors did not find it relevant to be included in the inferential analysis, however descriptive analysis was applied for this variable) of respondents and factors associated with depression and anxiety were analysed using descriptive statistics (frequencies and percentages). Descriptive statistics were also used to determine the general prevalence of the mental disorder and examine the distribution of specific symptoms for each. Pearson’s χ2 test of independence was used to test bivariate associations in the outcomes across sociodemographic characteristics. Multivariate logistic regression analysis was used to estimate the odds of developing the outcomes with displacement-related factors while controlling for statistically significant sociodemographic correlates. Adjusted odds ratios (AORs) were determined with a 95% CI. These associated factors were selected a priori based on evidence from relevant literature and our theoretical assumption that these factors will be relevant in studying depression and anxiety in the specified population. Only age, sex and other factors that were associated with the outcomes of interest in the χ2 procedures were included in the corresponding multivariable procedures to limit the probable risk of overadjusting without compromising the identification of the predictors for the outcome. ORs were used to determine the strength of association in the model. The significance threshold was set at α=0.05.
Results
The sociodemographic characteristics of the study respondents are presented in table 1. Slightly over half of the respondents (51.0%) were female. The average age of participants was 34.1 (11.1) years (with a range of 18–74). Most respondents (63.3%) were aged between 18 years and 35 years, while older adults aged 56 years and above comprised the least respondents (4.8%). Also, most respondents identified themselves as married (43.3%) or single (26.0%) and had attained either a primary (24.8%) or secondary education (36.4%). In terms of residence status, the majority of the respondents (51.9%) were indigenes of Ogoja LGA, Cross River State. Respondents were predominantly farmers (45.4%) and business owners (24.5%), while 22.3% were unemployed.
Sociodemographic characteristics of the study respondents
Furthermore, most respondents (60.3%) had less than four members living in their makeshift shelters or households. Almost a quarter of respondents (23.3%) earned no monthly income. Among the income earners, 57.9% earned between none and ₦30 000. Most of these respondents (40.3%) were displaced by natural disasters, while conflicts (32.2%) also led to displacements. Lastly, most respondents (48.3%) had been displaced for over 6–12 months.
There were 246 respondents who were positive for depression and 221 who were positive for anxiety disorder. The study found the prevalence of depression and anxiety disorders to be 73.4% and 66.0%, respectively.
Table 2 shows test results for statistically significant relationships between sociodemographic characteristics and anxiety and depression disorders. There was no significant relationship between the sex of respondents and anxiety in the study population (χ2=0.002, df=1, p=0.971). We, however, failed to reject the null hypothesis of no significant relationship between sex and anxiety disorder in the study population. There was also no significant relationship between age and anxiety disorder(χ2=2.11, df=2, p=0.354). We, therefore, failed to reject the null hypothesis of no statistically significant relationship between age and anxiety disorder. There was also no statistically significant relationship between marital status and anxiety disorder in the study population(χ2=7.46, df=4, p=0.112).
χ2 analysis of the relationship between sociodemographic characteristics and anxiety and depression disorders
There was no statistically significant relationship between participants’ level of education and anxiety disorder (χ2=4.40, df=3, p=0.223). We failed to reject the null hypothesis. There was also no statistically significant relationship between respondents’ residence status and anxiety disorder(χ2=0.76, df=1, p=0.381). We, however, failed to reject the null hypothesis. Furthermore, there was a statistically significant relationship between respondents’ occupation and anxiety disorder (χ2=9.34, df=3, p=0.030). We, therefore, rejected the null hypothesis. There was a statistically significant relationship between family size and anxiety disorder (χ2=28.7, df=1, p<0.001). Therefore, we rejected the null hypothesis of no significant relationship between family size and anxiety disorder in the study population. We also found a statistically significant relationship between respondents’ monthly income and anxiety disorder (χ2=25.1, df=4, p<0.001); hence, we rejected the null hypothesis of no statistically significant relationship between income and anxiety disorder in the study setting. Lastly, there was a statistically significant relationship between duration of displacement and anxiety disorder in the study setting (χ2=12.75, df=3, p=0.005).
Furthermore, there was a statistically significant relationship between sex of respondents and depression (χ2=6.66, df=1, p=0.010). We rejected the null hypothesis of no significant relationship between sex and depression in the study population. There was no statistically significant relationship between age and depression in the study population (χ2=3.08, df=2, p=0.221). We, therefore, failed to reject the null hypothesis. In terms of marriage, there was a statistically significant relationship between marital status and depression in the study population (χ2=12.7, df=4, p=0.013). Therefore, we rejected the null hypothesis of no statistically significant relationship between marital status and depression in the study population.
In addition, there was no statistically significant relationship between the level of education and depression (χ2=4.52, df=3, p=0.211). We, therefore, failed to reject the null hypothesis. The study also found that there was no statistically significant relationship between residence status and depression in the study population (χ2=0.87, df=1, p=0.353); hence we failed to reject the null hypothesis. Occupation had no significant relationship with depression in the study population (χ2=1.96, df=3, p=0.063); hence we failed to reject the null hypothesis. There was a statistically significant relationship between family size and depression in the study area (χ2=11.9, df=1, p=0.001); hence we rejected the null hypothesis. In terms of income, there was a statistically significant relationship between respondents’ monthly income and depression (χ2=11.5, df=4, p=0.021); hence we rejected the null hypothesis. Lastly, there was a statistically significant relationship between duration of displacement and depression in the study population (χ2=12.9, df=3, p=0.005); hence we rejected the null hypothesis.
Table 3 indicates the distribution of χ2 p values to establish the relationship between displacement-related factors with depressive and anxiety disorder in the study population. The displacement-related factors significantly associated with anxiety disorder in the study population include discrimination as a result of present status (χ2=17.5, df=1, p<0.001), financial strain (χ2=12.3, df=1, p<0.001), living in an overcrowded shelter (χ2=9.45, df=1, p=0.002), fears over reprisal attacks or natural disasters (χ2=9.67, df=1, p=0.002), being separated from family due to conflicts and/or disasters (χ2=9.65, df=1, p<0.001), and concern about health or safety (χ2=9.33, df=1, p=0.002). In each of the above scenarios, we, however, rejected the null hypothesis of no statistically significant relationship between displacement-related factors and anxiety disorder in the study population. The displacement-related factors significantly associated with depression in the study population include discrimination as a result of present status (χ2=19.04, df=1, p<0.001), financial strain (χ2=8.81, df=1, p=0.003), loss of loved ones due to crises or natural disaster (χ2=11.3, df=1, p=0.001), living in an overcrowded shelter (χ2=9.83, df=1, p=0.002), and fears over reprisal attacks or natural disasters (χ2=22.6, df=1, p<0.001). In each of the above scenarios, we however reject the null hypothesis of no statistically significant relationship between displacement-related factors and depression in the study population.
χ2 analysis of displacement-related factors associated with depression and anxiety disorders
Table 4 shows the multivariate logistic regression analysis of the sociodemographic correlates and displacement-related factors associated with anxiety disorder after adjusting for age, sex and all other potential covariates that were found significant in the bivariate χ2 analysis. Gender showed a negative relationship with anxiety disorder, meaning that men were less likely than women to develop an anxiety disorder in the study population (B=−0.49, p=0.113, AOR=0.62 (95% CI: 0.34 to 1.11)). This relationship was, however, non-significant. Age showed no significant relationship with the outcome. The displacement duration for 1 year and greater was also a positive and significant correlate of anxiety disorder in the study population (B=1.29, p=0.048, AOR=3.64 (95% CI: 1.01 to 13.10)). There was a negative and significant relationship between family size and anxiety disorder. The odds of anxiety disorder in ≥4 family size decreases by 0.28 compared with those who have smaller family size (B=−1.27, p<0.001, AOR=0.28 (95% CI: 0.15 to 0.51)). In other words, having a larger family size is protective. There was a positive and significant relationship between fears over reprisal attacks or natural disasters and the development of anxiety in the study population (B=1.43, p=0.004, AOR=4.19 (95% CI: 1.59 to 11.1)).
Multivariate analysis of sociodemographic correlates, displacement-related factors, and anxiety and depression disorder
Table 4 also shows the multivariate logistic regression analysis of the sociodemographic correlates and displacement-related factors associated with depression after adjusting for age, sex and all other potential covariates that were found significant in the bivariate χ2 analysis. Gender showed a positive relationship with depression. Men were more likely than women to develop depression in the study population (B=0.74, p=0.015, AOR=2.09 (95% CI: 1.15 to 3.82)). Age showed no significant relationship with this outcome. The displacement duration for greater than 6 months to 1 year was also a positive and significant correlate of depressive disorder in the study population (B=1.27, p=0.020, AOR=3.55 (95% CI: 1.23 to 10.31)) There was a negative and significant relationship between family size and depression in the study population. The odds of depression in ≥4 family size decreased by 0.55 compared with those who have smaller family size (B=−5.92, p=0.049, AOR=0.55 (95% CI: 0.29 to 0.97)). In other words, having a larger family size is protective against depression in the study population. There was a positive and significant relationship between financial strain and the development of depression in the study population (B=1.55, p=0.023, AOR=5.43 (95% CI: 1.62 to 18.2)).
A significant relationship was identified between loss of loved ones as a result of conflicts or disasters and depression (B=0.65, p=0.040, AOR=1.92 (95% CI: 1.03 to 3.56)), implying that displaced persons who reported the loss of a loved one were almost two times more likely to develop depression.
Discussion
Main findings
The current study explored the prevalence of mental disorders among internally displaced adults (18 years and above) in Ogoja LGA of Cross River State, Nigeria. This was the first study to assess the prevalence of depression and anxiety in this hard-to-reach IDPs population. Additionally, this study is one of a few to systematically assess sociodemographic correlates and other associated factors such as adverse life events and displacement-related factors among IDPs in Ogoja.
Overall, the study’s results showed a high incidence of depression and anxiety in the study population. A higher prevalence of mental health concerns was identified in this investigation compared with previous studies of displaced persons: the occurrence of anxiety disorder was found to be 66.0%. This is consistent with a discovery by Atsua et al3 who found anxiety disorder to be highly prevalent (99%) among IDPs in Benue State, Nigeria. Another study in Uganda found the prevalence of generalised anxiety disorders to be 73%.11 These findings support the notion that most displaced persons experience anxiety symptoms due to many displacement-related stressors. Displaced persons in this present study were also found to have depressive symptoms, with a prevalence of 73.4%. Similarly, a study in Benue state, Nigeria, found a very high prevalence of major depression (93%) among IDPs.3 Another study12 found a slightly lower prevalence of probable depression (59.7%) among persons displaced by postelection crises in Kaduna, Nigeria. Findings regarding depression from this study were found to be consistent with another study13 which found an equally high prevalence (96.1%) of depression among IDPs in Maiduguri, Nigeria.
Sociodemographic factors most significantly associated with anxiety symptoms were displacement duration for greater than 1 year and family size. Another study3 found similar trends in prolonged displacement and a high prevalence of anxiety in IDPs settings in Benue, Nigeria. More protracted displacements can lead to heightened worry about the unexpected. In terms of family size, a greater number of persons in a household was found to be more protective against anxiety when compared with a family with fewer persons. The reasoning for this protective factor of increased family size among IDPs could be that these persons require functional social support systems from which they draw mutual support. This nurturance may not be found within the general population, especially for those who have migrated from other locations. Social support is the perception or experience of being cherished and cared for while also being held in high esteem.14 However, this idea that more is better in families contrasts with a study15 that found that larger family size among IDPs led to a heightened risk of psychopathology.
Sociodemographic factors mainly associated with depression included male gender, prolonged displacement and smaller family size. Regarding the relationship between male gender and experiencing depressive symptoms, as the heads of the house, men are generally more likely than women to feel responsible for meeting their family’s needs. Thus, they may be under daily pressure to go far and wide to seek rare sources of livelihood to support their families. This finding is not consistent with the results of some other researchers11 12 16 17 who found a higher prevalence of depression among women than men. However, having a larger family size was found to be protective against depressive symptoms. This may be due to the mutual social support that a family unit provides for one another. To the best of the researcher’s knowledge, no previous research has found contrasting or conflicting results regarding depression and family size among displaced persons.
Discrimination and fear over reprisal attacks or natural disasters were identified as significant correlates of anxiety symptoms among Ogoja IDPs. The constant and mounting psychological and cultural efforts to adapt to a hostile or unsupportive environment could explain the links between discrimination and anxiety. This is consistent with findings from an African study18 that identified discrimination as one of the postmigration and displacement stressors among displaced persons. IDPs may suffer anxiety over fear of reprisals because of excessive worrying about things that may happen if the reprisals eventually occur. These fears are uncontrollable and can lead to increased swearing, complaining, hypervigilance and difficulty in thinking coherently.
Financial strain and loss of loved ones were factors found in this present study to be associated with depressive symptoms. The relationship with financial strain may be due to the daily need to secure individual and family necessities. However, the futility of searching for unavailable resources can lead to feelings of worthlessness and thoughts of suicide. This finding is consistent with that of Steel et al18 who found financial issues to be one of the postmigration and postdisplacement factors associated with depression. An earlier study12 also supports this finding. Loss of loved ones means loss of critical social support systems needed to cope in the face of displacement, hence its link with depression. A Haitian study also found that the injury or death of close family members in the aftermath of the massive 2010 Haitian earthquake were significant predictors of major depressive disorders among displaced persons.19
Limitations
Because this was a cross-sectional study, predictors of the study’s outcomes must be interpreted with caution because of the possibility of responder bias. Recall bias could have also occurred since the study was conducted a few years postconflict, but the nature of the psychological problems made it possible for the displaced persons to easily recollect their experiences.
Implications
In remedying the overarching effects of mental health problems among IDPs, a combined effort from all socioecological niches is needed to implement broad public health approaches. Re-integration efforts and fostering tolerance are necessary to ensure that the well-being of the respondents is an ultimate priority while also ensuring that other community members cease inflicting hostilities on these vulnerable groups.
Conclusion
This study highlights the sociodemographic and trauma-related factors associated with the co-occurrence of symptoms of CMDs among IDPs in Ogoja LGA, Nigeria. The findings suggest that the high prevalence of these CMDs in the study population may be related to many traumatic and adverse life events. In other words, the results suggest significantly elevated mental health symptoms—rates that are consistent with those of previous studies globally. Such a high impact of displacement is partially related to poor political will, leading to low access to needed mental health services for the most vulnerable. However, this study has broad implications for the mental health of populations affected due to conflicts and natural disasters. The impact of the findings underlines the complex aetiology of these two mental problems and the need to cater to the well-being of those at risk who have been exposed to trauma-related events. Accessible and affordable mental health services should be provided for these persons while also considering a social welfare scheme that covers their health expenses. Additionally, socioeconomic conditions targeting IDPs in Ogoja LGA should be improved by conducting large-scale mapping to identify this population. These persons are rarely recognised because they do not have a voice.
Data availability statement
Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available. Data are not publicly available but can be made available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics and Research Committee Ministry of Health, Calabar. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank Dr Ekpereonne B Esu through whose guidance this project was accomplished. The authors also thank their respondents who were the participants of this study.
References
Ugbe Maurice-Joel Ugbe is an Assistant Lecturer at the Department of Public Health, University of Calabar, Nigeria. He holds a Master of Public Health (MPH) specializing in Epidemiology and is currently undergoing training to obtain a PhD in Public Health. He has been trained in several USAID-sponsored programs including Orphans and Vulnerable Children Projects, Child Protection, Gender-based violence, and Mental health. While at the University, Maurice-Joel has been appointed as the Assistant Technical Officer for the National Collaborating Center for Excellence for Human Resource and Training where he has assisted in facilitating training for health workers over the years. He has previously served in the NKST School of Health as a teaching assistant at the department of Environmental Health where he gained valuable experience teaching finalists. He also facilitated lectures on the various aspects of Family Planning to Midwives at the NKST school of Nursing and Midwifery, Mkar for 2 months. Maurice-Joel’s research philosophy is to engage communities in ways that data collected and disseminated propel meaningful change among the grass-root population, most notably the most vulnerable.
Footnotes
Twitter @LordMarvin2
Contributors UM-JU conceived and carried out the study under the supervision of EBE who also planned the project, designed the instrument and proofread the manuscript. MMB and JAE collected data, OIE was involved in project planning and cleaning of the data. UM-JU analysed the data and developed the manuscript. TMA proofread the final submission and ensured all data were in order. UM-JU stands as guarantor and as an implication had access to every phase of this study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.