Article Text

Abstract
Background Clinical high risk (CHR) of psychosis is a state in which positive symptoms cause the subjects distress but do not approach a severity level that fulfils the criteria for a psychotic episode. CHR exhibits cognitive deficits; however, the underlying neurobiological mechanisms remain unclear. This study aimed to investigate whether brain activation measured by the levels of oxygenated hemoglobin (oxy-Hb) in CHR subjects could be correlated with cognitive deficits.
Methods Fifty-eight CHR individuals who fulfilled the criteria for attenuated positive syndrome as specified in the Structured Interview for Prodromal Syndrome (SIPS) and the Scale of Prodromal Syndrome (SOPS) and 58 age- and sex-matched healthy participants were included in the study. All subjects completed the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) Consensus Cognitive Battery (MCCB) that includes tests measuring attention, verbal memory, verbal fluency, executive function, and general intelligence. Functional near-infrared spectroscopy (fNIRS) was used to measure the level of oxy-Hb in the dorsolateral prefrontal and frontotemporal cortices.
Results We observed significantly decreased oxy-Hb levels in channel 32 (located in the right superior temporal gyrus, rSTG)) within the CHR individuals compared with that in the healthy controls (HCs) (t=−3.44, Bonferroni-corrected p=0.002), indicating lower brain activity. A significant positive correlation was observed between task-related β values and working memory in the CHR group (r=0.35, p=0.008).
Conclusions The brain activation of rSTG is abnormal among subjects at clinicial high risk for psychosis. This abnormality is probably associated with the neural mechanisms of deficits in the working memory during the early stage of psychosis.
- cognition disorders
- schizophrenia
- psychiatry
Data availability statement
Data are available upon reasonable request. The data used in this study are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Cognitive deficits are a key feature of the early stages of psychosis. Findings to date strongly indicate that memory impairments are present during the premorbid phase of psychosis and, in particular, are predictive of future conversion to psychosis.
What this study adds
The current study investigated brain activation that was measured with functional near-infrared spectroscopy (fNIRS) in individuals with clinical high risk (CHR) and healthy controls(HCs). Compared with HCs, the CHR group showed reduced brain activation in the right superior temporal gyrus (rSTG) during the verbal fluency test (VFT). This reduced brain activation had a significant positive correlation with working memory.
How this study might affect research, practice or policy
The current study provides evidence that abnormal brain activation in the rSTG is probably associated with the neural mechanisms of working memory deficits in CHR.
Introduction
Clinical high risk (CHR) of psychosis is defined as a state in which subthreshold positive psychotic symptoms, such as perceptual abnormalities or overvalued ideas, occur, but their severity or duration fails to fulfil the criteria for a diagnosis of psychosis.1 2 Cognitive deficits are a key feature of CHR individuals and are associated with functional outcomes.3 A meta-analysis comparing CHR individuals with healthy controls (HCs) found extensive cognitive impairments in executive function, verbal and visual memory, verbal fluency, attention, working memory, and social cognition in the at-risk group.4 Findings to date strongly indicate that memory impairments are present during the premorbid phase of psychosis, and working memory impairments, in particular, are predictive of future conversion to psychosis.5 However, the underlying neurobiological mechanisms are not well understood.
Functional magnetic resonance imaging (fMRI) has been widely used to investigate neurobiological deficits in CHR. However, fMRI studies have reported inconsistent findings, with some studies reporting hyperactivation and others showing hypoactivation in the dorsal lateral prefrontal cortex (DLPFC) during working memory tasks.6 7 However, fMRI is inconvenient for many CHR subjects.
Functional near-infrared spectroscopy (fNIRS) is a recently developed, convenient, and non-invasive optical neuroimaging technology that uses changes in measured infrared light to make inferences regarding changes in the concentrations of cortical haemoglobin.8 Cortical tissue is interrogated using emitted light from either a light-emitting diode (LED) or a laser source and is measured using a light detector. The distance between each emitter and detector was fixed at 3 cm. Compared with fMRI, fNIRS is restricted to the measurement of shallow cortical activity and offers a low-cost, well-tolerated, convenient set-up and acquisition with reduced sensitivity to motion artefacts.8 More importantly, fNIRS provides a measurement of oxy-haemoglobin (oxy-Hb) and deoxy-haemoglobin (deoxy-Hb) concentrations, which are strongly correlated with fMRI signals.9 Previous research has shown that fNIRS is sensitive to differences in clinical diagnoses. Studies using fNIRS have indicated that during the verbal fluency test (VFT), patients with stable chronic schizophrenia show reduced activity and characteristic waveform patterns in the prefrontal cortex.10 A cross-sectional fNIRS study that focused on four different clinical stages of psychosis (healthy, CHR, first-episode, and chronic schizophrenia) indicated there are varying activity patterns among different prefrontal cortex (PFC) subregions.11 Brain activity in the superior temporal gyrus(STG), inferior frontal gyrus (IFG), and middle frontal gyrus (MFG) decreased with advancing clinical stages of psychosis,12 which was similar to the results of previous fMRI studies of the different clinical stages.13
In the present study, we measured brain activity in the prefrontal and temporal cortices using multichannel fNIRS measurements and assessed clinical symptoms and cognition. Our main hypotheses were that (1) CHR showed reduced brain activation compared with healthy individuals, and (2) reduced brain activity could be associated with cognitive function.
Materials and methods
Study participants
Eighty-seven CHR participants were recruited from the Shanghai Mental Health Center from January 2019 to November 2020. Inclusion criteria included no prior visits to mental health services and drug naivety for antipsychotic medication. The CHR evaluation was performed by a senior psychiatrist using the Structured Interview for Prodromal Symptoms (SIPS) and Scale of Prodromal Syndrome (SOPS)14 to exclude any other psychotic symptoms or mental disorders. Nineteen CHR participants were excluded during the screening process: 10 refused to sign the informed consent, 6 failed to finish the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) Consensus Cognitive Battery (MCCB) test, and 3 did not complete the clinical evaluation. Ninety-two healthy controls (HCs) were recruited from a local school and the community through an internet advertisement. Exclusion criteria included prodromal psychotic symptoms, other mental disorders, or a family history of mental disorders. The Mini-International Neuropsychiatric Interview (MINI)15 was administered by a senior psychiatrist for the HCs evaluation. Ten HCs were excluded during the screening process: 6 failed to meet the inclusion criteria, and 4 did not complete the MCCB test. An additional 10 CHRs and 6 HCs were excluded during the fNIRS data preprocessing step due to the low quality of fNIRS signals. Finally, 58 CHRs and 76 HCs were enrolled. To exclude the effects of demographic characteristics on the fNIRS results, we matched the groups according to age and sex16 and analysed outcomes for 58 CHRs and 58 HCs (figure 1). All subjects were right-handed, as assessed using the Edinburgh Handedness Inventory.17 All participants were provided with a detailed explanation of the study. In accordance with the Declaration of Helsinki, written informed consent was obtained from all participants prior to their participation in the study. The participants younger than 18 years submitted written informed consent forms signed by their parents. The study was approved by the Ethics Committee of the Shanghai Mental Health Center.

Flowchart of enrolment of the subjects. CHR, clinical high risk of psychosis; fNIRS, functional near-infrared spectroscopy; HC, healthy control; MCCB, Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) Consensus Cognitive Battery; NIRS, near-infrared spectroscopy.
Clinical and cognitive assessment
The SIPS/SOPS was used for clinical assessment of CHR participants on the day of the fNIRS measurements. The SIPS/SOPS comprises 19 items: positive symptoms (scales P1–P5), negative symptoms (scale N1–N6), disorganised symptoms (scale D1–D4) and general symptoms (scale G1–G4). The assessments were conducted by a senior psychiatrist. With the permission of Yale university, a Chinese version of the SIPS/SOPS was translated by our team and tested for reliability and validity in a Chinese population.18 19
The MCCB20 21 is a standardised method to measure the cognitive function of patients with schizophrenia. The MCCB has been translated into Chinese, and both co-norming and standardisation have been performed in China. It demonstrated sufficient clinical validity and reliability in controls and patients with schizophrenia, with the test–retest reliability of the subtests ranging from 0.73 to 0.94.22 Consistent with the original version of the MCCB, the Chinese version comprises nine tests covering seven cognitive domains: speed of processing, attention/vigilance, working memory, verbal learning, visual learning, reasoning and problem-solving, and social cognition.23 The social cognition test is not applicable to participants aged less than 18 years; therefore, we did not apply social cognition in this study. The raw data of the MCCB test were input twice (double data entry) into the MCCB computer program and converted to T-scores as well as a composite T-score.
Verbal fluency test
Participants completed a 160 s block-design letter version of the VFT. The VFT has been widely used in previous fNIRS studies.24 A 160 s block comprises three different time periods: a 30 s pretask period, a 60 s task period, and a 70 s post-task period. In the pretask and post-task periods, the participants were instructed to count numbers from one to five repeatedly. The 60 s task period comprised three 20 s subperiods. During each 20 s period, one of three Chinese syllables (‘中’, ‘日’ and ‘蓝’, which indicate middle, sun and blue) was audibly presented to the subjects; the subjects were then instructed to generate as many words as possible that began with the same syllable (figure 2A). The experiment was conducted in a quiet environment and the participants were asked to sit in a comfortable wooden chair with their eyes open. To reduce possible distractions, a screen was placed approximately 1 meter in front of each participant and the participants were asked to look at the red asterisk at the centre of the screen to minimise head movements. Before the experiment, each subject was provided with instructions on how to answer correctly and a practice trial was conducted to ensure that they understood the instructions. Task performance was evaluated by the total number of correct words generated during the 60 s task period.
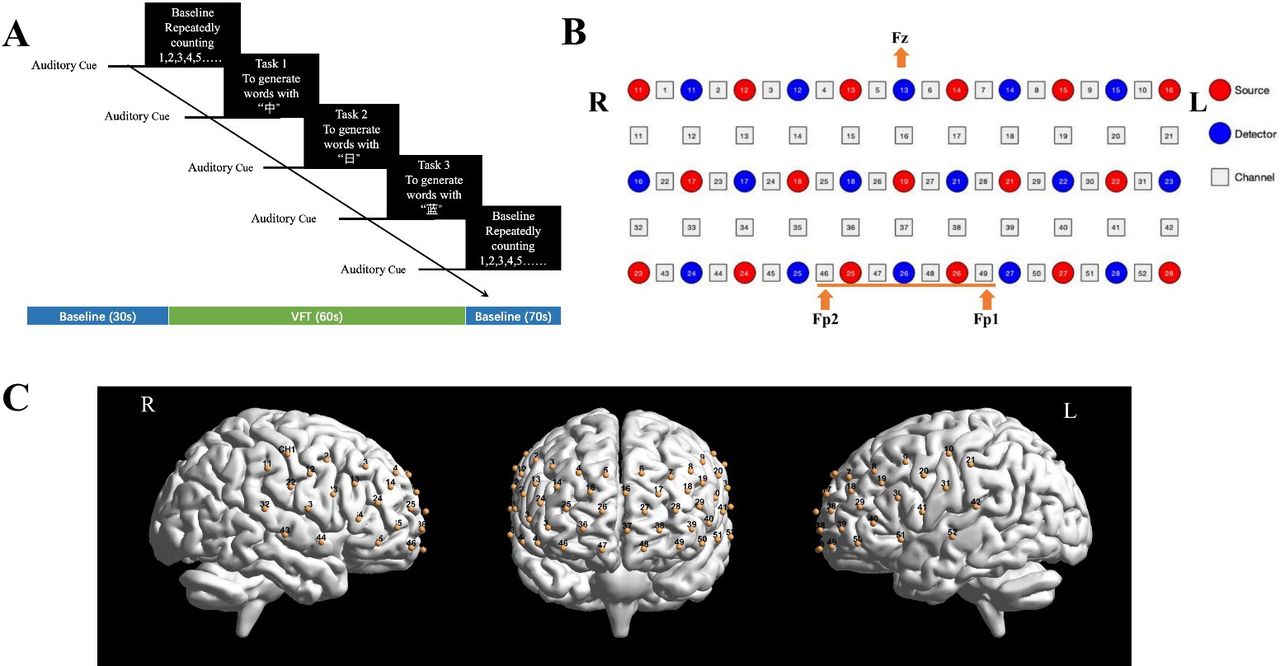
(A) The verbal fluency test (VFT). It consists of a 30 s pretask resting-state period and three 20 s word-generating tasks, followed by a 70 s post-task resting-state period. (B) 3*11 optode montage. Red circles represent light sources (emitter), blue circles indicate light detectors, and numbers 1–52 indicate the location of each optode pair (channel). When we positioned the patch according to the International 10–20 system, detector 13 was located at Fz, and channels 49 and 46 were placed in Fp1 and Fp2, respectively. (C) The optode was placed on the bilateral frontal and temporal cortex. L, left; R, right.
fNIRS instrument
We used a 52-channel fNIRS instrument (ETG-4000; Hitachi Medical, Tokyo, Japan) to measure changes in haemoglobin concentration. The fNIRS instrument uses two wavelengths of near-infrared light (695 nm and 830 nm) and calculates the amount of absorbed near-infrared light based on the modified Beer-Lambert law.25 Seventeen emitters and 16 detector probes were thermoplastically set in a 3 row × 11 column matrix within the 52 channels on the participant’s forehead. The lowest probe line was set along the Fp1–Fp2 line (figure 2B), as defined by the international 10–20 system. The distance between pairs of sources and detectors was set to 3.0 cm. The area between each probe set was defined as one ‘channel’, which was sufficient to obtain data from depths of 20–30 mm under the scalp. This arrangement allows imaging of the surface of both the bilateral prefrontal cortices as well as the bilateral temporal cortical areas (figure 2C). The fNIRS imaging data were collected at a constant sampling frequency of 10 Hz. Relative changes in haemoglobin concentration assessed using fNIRS were provided in units of mM.mm.
The spatial information for each channel was estimated using data from the Functional Brain Science Laboratory at the Jichi Medical University in Japan.26 As in previous studies,27 fNIRS channels were anatomically labelled only after the Laboratory of Neuro Imaging (LONI) Probabilistic Brain Atlas (LPBA) region when the highest probability was determined. As oxy-Hb has stronger correlations with blood oxygen level-dependent signals compared with deoxy-Hb when measured using fMRI,9 mean changes in oxy-Hb measured during the VFT were used as indices of brain cortical activity.
Statistical analysis
To test for group differences in terms of years of education, VFT performance, and neuropsychological scores, we analysed the data using paired t-test.
The two toolboxes Homer228 and NIRS-KIT29 were used in the quantitative analysis of fNIRS signals and to calculate the activation of oxy-Hb levels. The fNIRS signals contain two types of noise that contaminate underlying cerebral haemodynamics. To initially remove these confounding factors from the fNIRS signal and recover the underlying brain activation patterns, the noisy channels were identified and pruned from the measurement list using the Homer2 function hmrPruneChannels (dRange=10–3–10−7 and SNRthres=5). Next, the optical density (OD) was transferred from the optical intensity using the hmrintensity2OD function. OD is defined as the logarithmic intensity ratio of the light falling on the material to the light transmitted through the material.30 The HOMER2 function hmrMotionArtifactByChannel was used to detect channel-wise motion artefacts. Channels with too many artefacts were rejected. Subsequently, OD was converted into concentration changes of oxy-Hb using the modified Beer-Lambert law.31 Lastly, a haemodynamic response function filter was adopted for temporal smoothing and to swamp the intrinsic temporal correlations and attenuate the high-frequency components.32 All of these steps were used to assess the quality of the raw data. Subjects whose channels had artefacts above 10% were rejected.
Before statistical analysis, fNIRS data underwent a series of preprocessing steps aimed at removing artefacts using the NIRS-KIT toolbox. The main goal was to minimise the influence of data acquisition errors and physiological artefacts. First, we used a polynomial regression model to estimate a linear trend and then subtracted it from the raw haemoglobin concentration signals. Second, the temporal derivative distribution repair method was used to correct the motion.33 Third, an infinite impulse response filter was used to remove irrelevant low-frequency and high-frequency components with a bandpass of 0.001–0.1 Hz. A general linear model was used to analyse the fNIRS time series. Task-related β values were defined as word-generating β values minus (pre-task+post-task β values)/2.
Paired t-test with Bonferroni correction (corrected p<0.05) was conducted on task-related β values at each channel. Images were created using the results visualisation function, in which channel-wise statistical values were mapped onto the standard brain space using the nfri_mni_plot function in the NFRI toolbox.34 Finally, Pearson’s correlation coefficients were used to examine the relationship between clinical variables (Positive and Negative Symptom Scale (PANSS), VFT performance and cognition), and task-related β values.
Results
Demographic characteristics
The demographic characteristics of the participants are presented in table 1. They were matched in age and sex, but the HC group had more years of education than the CHR group. Moreover, the HC group showed significantly better VFT performance than the CHR group. Compared with the HC group, the CHR group showed cognitive deficits in the broad cognitive domain, including speed of processing, attention/vigilance, working memory, verbal learning, reasoning and problem-solving, and social cognition.
Demographic data of the participants
Brain activation during the VFT
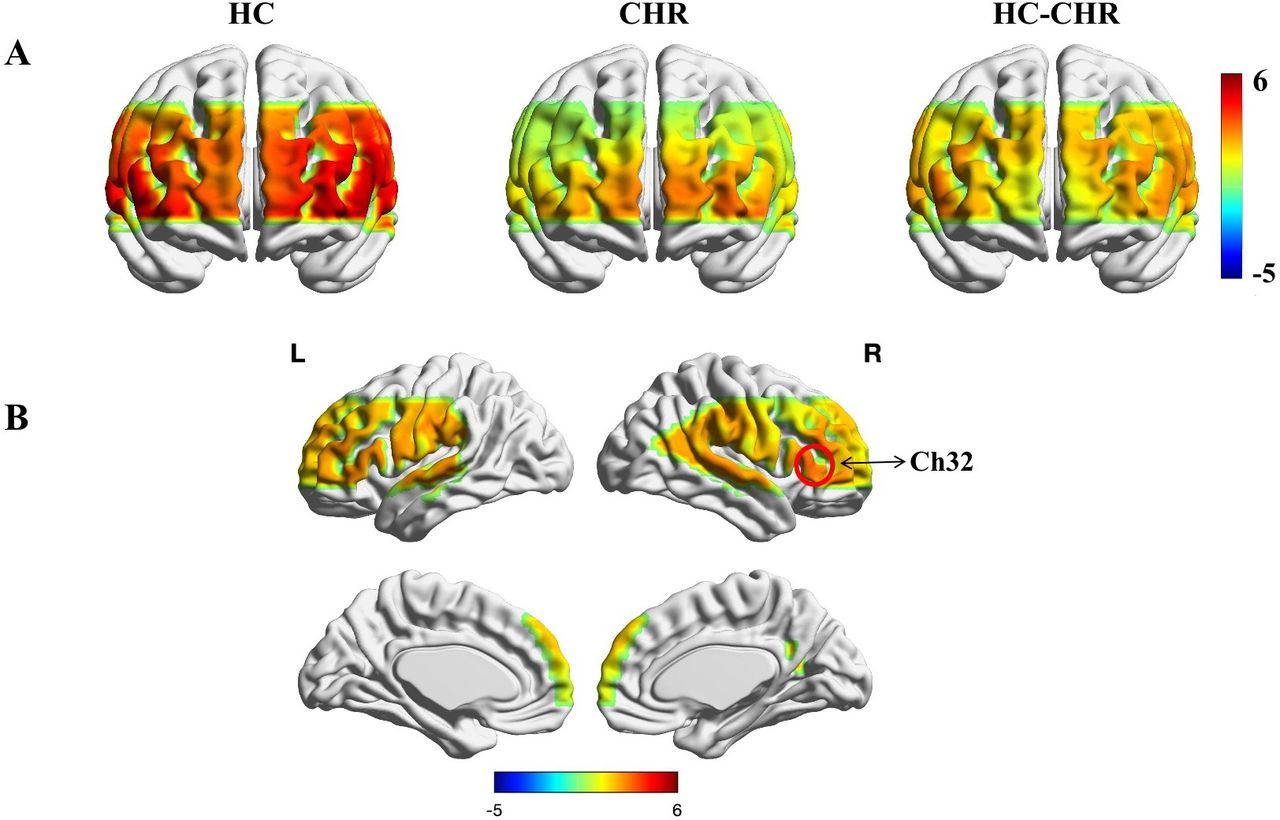
The changes in oxy-Hb levels during the VFT task significantly decreased in channel 32 in the CHR group (the right superior temporal gyrus, rSTG) compared with the HC group. Paired t-test showed that the task-related β values in the CHR group were lower than those in the HC group (Bonferroni correction, p=0.002) (figure 3). The activation map for oxy-Hb level changes during the VFT task is shown in figure 4.
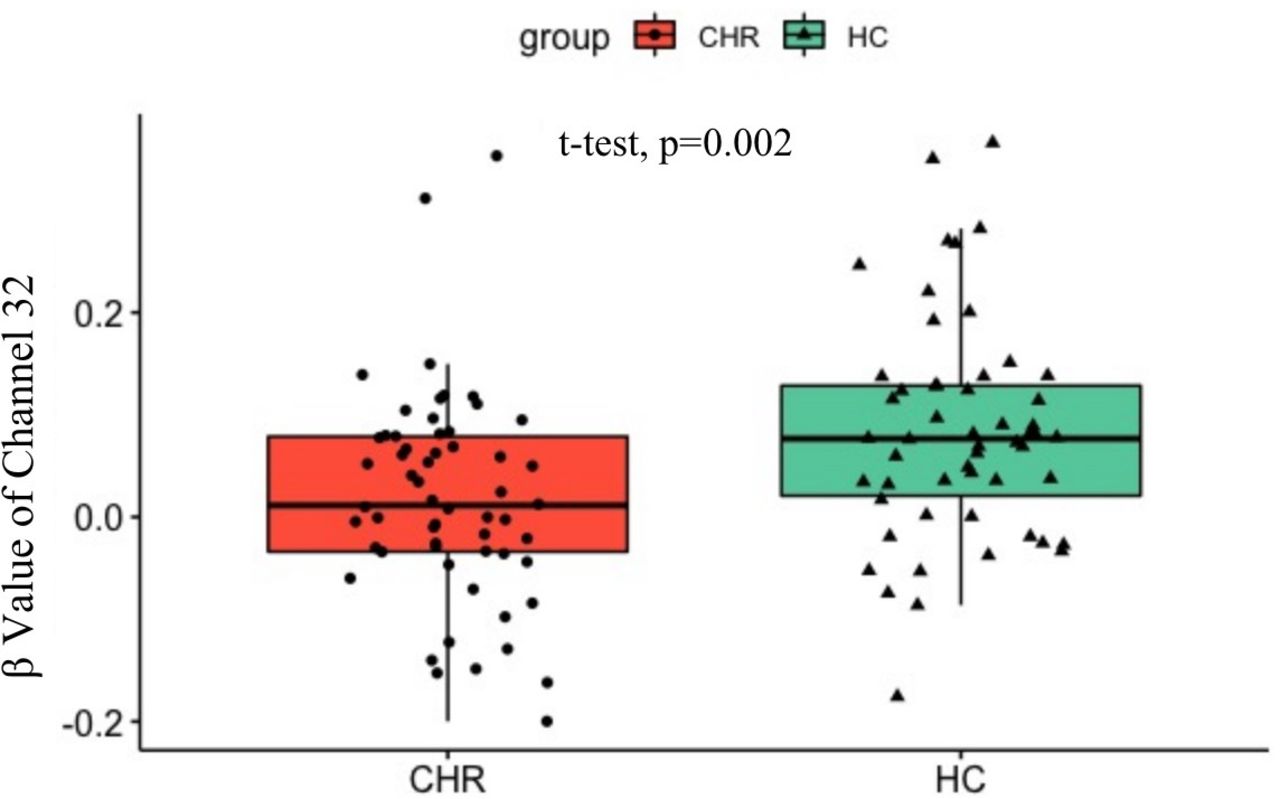
Task-related β value of channel 32 in the CHR and HC group. CHR, clinical high risk; HC, healthy control.
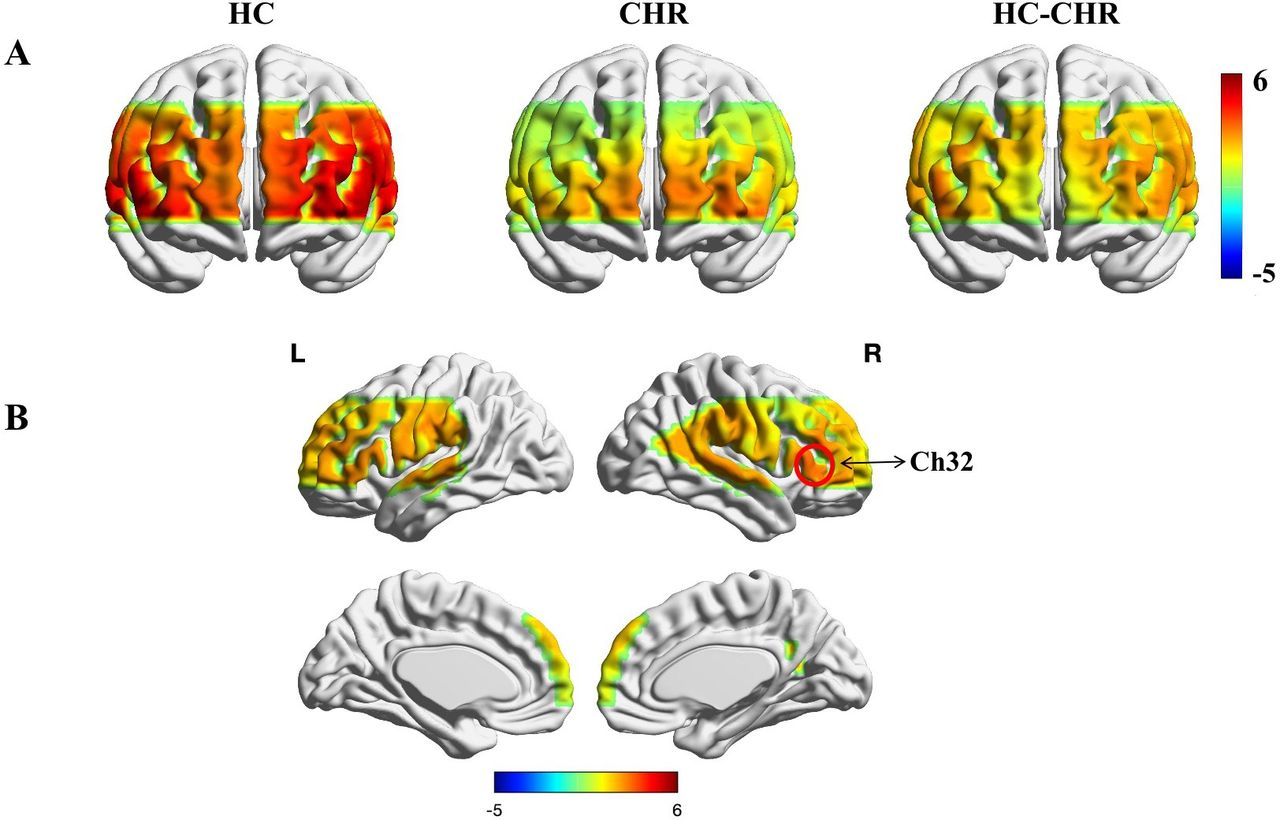
Cortical activation map of oxy-Hb level during the VFT in different groups. (A) Compared with the HC group, the CHR group showed significantly decreased activation in Ch32; (B) Ch32 was located in the right superior temporal gyrus. Ch, channel; CHR, clinical high risk; HC, healthy control; oxy-Hb, oxy-haemoglobin; VFT, verbal fluency test.
Correlation between cortical activation and clinical symptoms
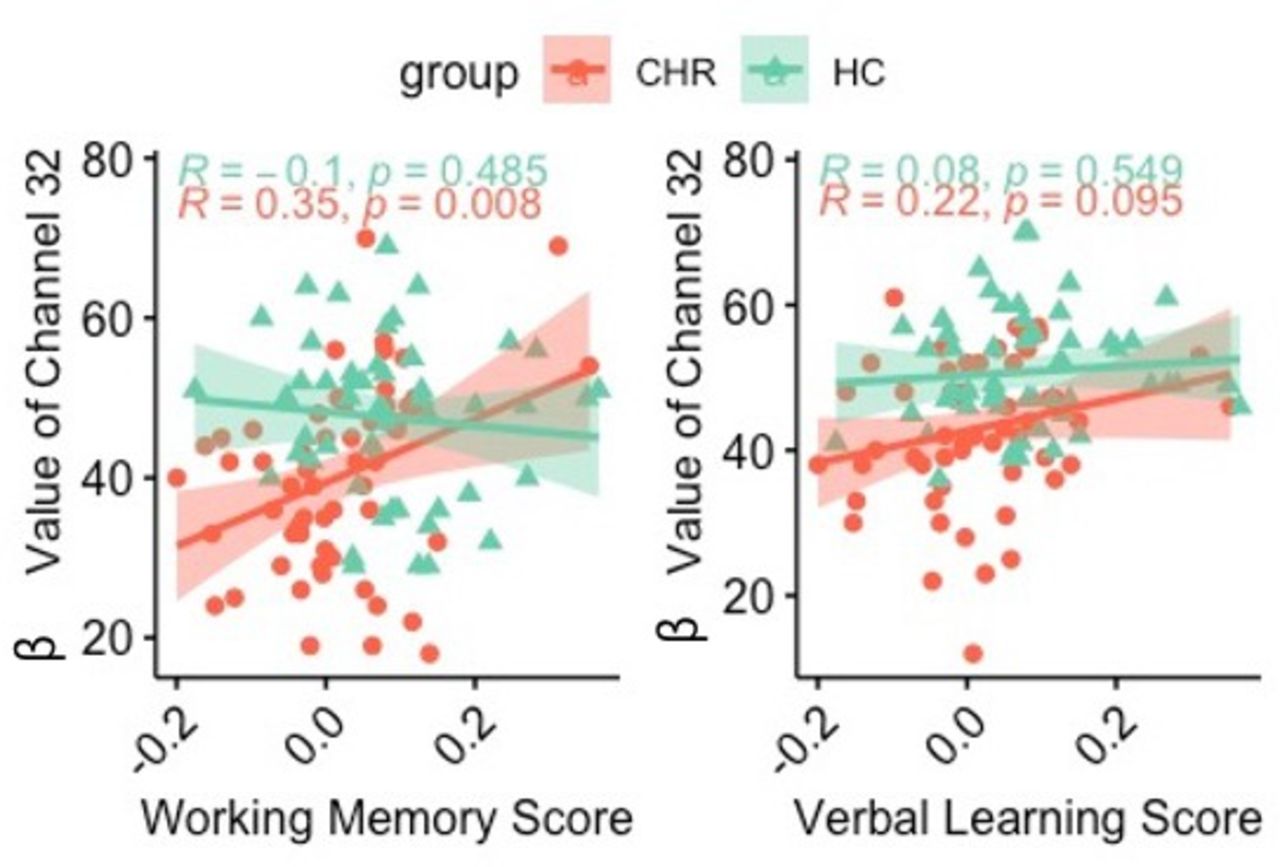
Pearson’s correlation analysis showed that task-related β values in channel 32 were positively correlated with working memory scores in the CHR group (r=0.35, p=0.008). The verbal learning scores were marginally significant (r=0.22, p=0.095; figure 5). However, there was no significant correlation in either working memory or verbal learning scores in the HC group.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation analysis between task-related β values of channel 32 and cognition (working memory and verbal learning). The results showed that the β value had a significant positive correlation with working memory and showed a marginally significant level with the score of verbal learning in the CHR group, while there was no significant correlation found in the HC group. CHR, clinical high risk; HC, healthy control.
Discussion
Main findings
The present study investigated brain activation changes during the VFT in CHR, as well as whether these brain activation changes were associated with clinical symptoms and cognition. The main findings were that the CHR group showed reduced brain activation in channel 32, located in the right STG. Moreover, task-related brain activation in channel 32 was positively correlated with working memory; however, there was no significant correlation between brain activation and VFT performance or clinical symptoms. There was no significant correlation between brain activation and cognition in the HC group. Generally, in the CHR group, a higher task-related β value indicated better working memory.
Our study is in line with previous studies that have provided evidence of decreased brain activity prior to the onset of psychosis. The VFT is a commonly applied cognitive task in fNIRS research,35 and we used the letter fluency task, which requires the generation of words based on phonemic cues. The performance of the VFT not only requires retrieval of items from long-term memory storage but also the working memory capacity to hold already-generated words.36 These task characteristics demand a wide variety of functions from the bilateral frontotemporal regions. The main decrease in activity was observed in the right STG. One of the functions of the STG is acoustic perception and comprehension for integrating meaningful verbal information in the dominant hemisphere.37 Moreover, task-related β values showed a marginal correlation with verbal learning. A previous study demonstrated that verbal fluency deficits are often present during the early stages of CHR and are a possible predictor of the transition to psychosis.38
Frontotemporal lobe dysfunction is a core feature of patients with schizophrenia.39 40 Many studies on fNIRS have used clinical variables to investigate symptom changes and their association with brain activity. They found a significant correlation between brain activation and PANSS total scores, as well as positive and negative scores.10 41 Chou et al42 43 found that in first-episode schizophrenia, there was a significant negative association between brain activity and PANSS negative scores in the bilateral inferior frontal gyrus and bilateral temporal regions. In another study conducted by Koike et al,12 the brain activity of the bilateral ventrolateral prefrontal cortex and the frontopolar and anterior parts of the temporal cortical regions in the CHR group was lower than those in the HCs.
Limitations
All findings must be interpreted with caution as this study has several limitations. First, in the current study, the CHR group only included 58 individuals and further studies with larger sample size are needed. Second, we only observed the cross-sectional outcome between the groups; the longitudinal outcomes of CHR and whether fNIRS can predict conversion to psychosis remain unclear. Future research will include a follow-up study investigating the various mechanisms of CHR progression in relation to cognition and brain activity. Finally, we divided the CHR patients into severe and mild groups but did not find any significant results. Most CHR cases were mild. Therefore, these results should be considered preliminary.
Implications
In conclusion, the brain activation of rSTG is abnormal among subjects at clinical high risk of psychosis when they perform VFT. This abnormality probably plays a key role in the neural mechanisms of deficits in working memory in the early stage of psychosis.
Data availability statement
Data are available upon reasonable request. The data used in this study are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of Shanghai Mental Health Center. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We are grateful to the patients, their families and the volunteers who gave their time to participate in this study.
References
Wei Yanyan obtained a master degree in Medical Psychology from the Second Military Medical University in Shanghai, China in 2016. After graduation, she became a member of Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine in China. At present, she is working towards a doctorate in psychiatry and mental health at the Shanghai Jiao Tong University School of Medicine. In addition, she is also an associate researcher in the EEG and neuroimaging department. Her main research interest includes early identification and intervention for mental disorders. She is also interested in the use of infrared functional brain imaging technology to explore brain activity in the cognitive process of patients with psychosis and towards the prediction of clinical intervention efficacy.

Footnotes
YW and XT contributed equally.
Contributors YW contributed to the fNIRS data analysis and writing of the manuscript. XT and TingZ contributed to the clinical data organisation and analysis. WS, LX, HC, ZQ contributed to the recruitment, clinical assessment and data acquisition. TianZ and JW designed the study and provided supervision for implementation of the study and interpretation of the results. JW was responsible for the overall content as the guarantor. All authors have contributed to and approved the final manuscript.
Funding This research was supported by grants from the National Natural Science Foundation of China (82001406, 81971251, 81671329, 81871050, 82171497, 82101582); Shanghai Science and Technology Committee Foundations (19ZR1445100, 19411950800, 16ZR1430500, 19411969100, 19410710800, 21ZR1481500, 20ZR1448600, 21S31903100); Foundation of Shanghai Mental Health Center (2020-FX-02); Clinical Research Center at Shanghai Mental Health Center (CRC2018ZD01, CRC2018ZD04, CRC2018YB01, CRC2019ZD02); Clinical Research Center at Shanghai Jiao Tong University School of Medicine (DLY201817, 20190102); Shanghai Clinical Research Center for Mental Health (19MC1911100); Project of the Key Discipline Construction, Shanghai 3-Year Public Health Action Plan (GWV-10.1-XK18); Shanghai Municipal Science and Technology Major Project (2018SHZDZX01, 2018SHZDZX05); and ZJLab.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.