Article Text

Abstract
Introduction To examine the effectiveness of universal suicide prevention interventions on reducing suicide mortality in high-income Organisation for Economic Co-operation and Development (OECD) member countries.
Methods We implemented a comprehensive search strategy across three electronic databases: MEDLINE (Ovid), PsycINFO (Ovid) and Embase (Ovid). All studies using time-series, retrospective, prospective, pre–post or cross-sectional study designs were included. Studies were required to examine suicide mortality as the outcome of interest. To help organise the results, studies were grouped into six broad categories of universal interventions consistent with the World Health Organization (WHO) Comprehensive Mental Health Action Plan. A narrative synthesis of results was used to describe the findings.
Results Of the 15 641 studies identified through the search strategy, 100 studies were eligible in the following categories: law and regulation reforms (n=66), physical barriers (n=13), community-based interventions (n=9), communication strategies (n=4), mental health policies and strategies (n=7), and access to healthcare (n=1). Overall, 100% (13/13) of the included physical barrier interventions resulted in a significant reduction in suicide mortality. Although only 70% (46/66) of the law and regulation reform interventions had a significant impact on reducing suicide, they hold promise due to their extended reach. Universal suicide prevention interventions seem to be more effective at reducing suicide among males than females, identifying a need to stratify results by sex in future studies.
Conclusions These findings suggest that universal suicide prevention interventions hold promise in effectively reducing suicide mortality in high-income OECD countries.
- suicide/self?harm
- interventions
- systematic Review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Suicide is a significant public health concern globally, with an estimated 800 000 people dying by suicide worldwide every year.1 The causes of suicide are complex and result from a combination of individual, social and economic factors that vary substantially between countries. For instance, the methods used by those who die by suicide, and the risk factors that influence suicide, vary substantially between low-income and high-income countries.2–4 For example, the most common method of suicide in South Africa is hanging followed by poisoning with pesticides and medication; however, in the USA, suicide death most commonly occurs by firearm, followed by suffocation.3 5 As a result, interventions that work in some countries may not work in others. For this reason, it is important to look at groupings of countries with similar social and economic contexts, such as Organisation for Economic Co-operation and Development (OECD) member countries belonging to the high-income category. Rates of suicide mortality in high-income OECD countries varied substantially in 2016, from 4 deaths per 100 000 individuals in Greece to over 24.6 deaths per 100 000 people in Korea.6 The impact of suicide mortality in high-income OECD countries are generally highest among older adults (aged >65 years), adolescents (aged 10–14 years) and males when compared with females.1
In 2015, the United Nations Sustainable Development Goals (SDG) were released to foster peace and prosperity for people and the planet, including targets set for 2030.7 The SDGs included goal (#3.4) to reduce global premature mortality from non-communicable diseases by one-third; indicators for this goal include a reduction in suicide mortality rates (SDG Indicator 3.4.2).7 Among all OECD countries, suicide mortality rates have decreased steadily, falling by close to 30% between 1990 and 2015, with pronounced declines of over 40% in countries such as Hungary, Estonia and Finland.8 Despite these declines, no OECD country is on-track to meet the SDG goal,9 which may reflect that current efforts do not adequately include comprehensive, multisectoral strategies to reduce suicide mortality, and that addressing social determinants of health is often overlooked in suicide prevention efforts.10 Identifying well-designed and transferrable interventions could strengthen suicide prevention strategies among several countries and facilitate meeting the SDG target.
In 2014, World Health Organization (WHO) launched the first global Comprehensive Mental Health Action Plan, of which one goal was to reduce suicide rates worldwide through prevention initiatives.11 Comprehensive suicide prevention strategies include universal, selective and indicated interventions.12 Universal interventions are designed to reach an entire population regardless of risk, as described by Rose.13 Whereas, selective interventions target sub-populations with potentially high risk for suicide (eg, people who have experienced trauma or abuse, or who are affected by conflict or disaster). Indicated interventions target specific individuals at greater risk (eg, people living with a mental illness, people who abuse substances, those who have previously attempted suicide).11
To date, most systematic reviews on suicide prevention have examined the effectiveness of context-specific interventions in school, community or healthcare settings,14 primary care interventions,15 psychosocial interventions,16 pharmacological interventions,17 technology-enhanced interventions18 or workplace interventions.19 Recent systematic reviews have examined universal suicide prevention interventions combined with selective and indicated interventions, which does not allow for a focused examination of universal interventions’ characteristics and efficacy.20 21 Given the demonstrated effectiveness of universal interventions to address other health problems such as universal smoking policies aimed at reducing smoking rates and alcohol access and pricing on rates of harmful alcohol use,22 23 it is essential to examine universal suicide prevention interventions and their impact in similar contexts. Thus, this systematic review’s objective was to examine the effectiveness of universal prevention interventions on reducing suicide mortality, as measured by counts or rates of suicide deaths, among high-income OECD countries.
Methods
Protocol and registration
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement,24 and was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; #CRD42018086273).
Study inclusion criteria
We followed the Population, Intervention, Comparator, Outcome framework to plan the components of our systematic review.25
Population
This review included studies with large populations (ie, community, city, state/province, country or region) living in one or multiple of the 33 high-income OECD countries, as categorised by the World Bank. Lithuania was excluded from this study because it was added to the OECD after the original search strategy was conducted in 2018. A full list of high-income OECD countries can be found in online supplemental file 1. No limitations were placed on the age or sex of the population.
Supplemental material
Interventions
Candidate studies were required to have studied a universal intervention, targeted at a whole geographic population, with the intention or the impact of reducing suicide mortality as rates or counts (eg, country, state or province, or citywide).
Comparators
Because this review included studies using a range of study designs, both studies with and without comparator (control) populations, such as a neighbouring state or city where the intervention was not implemented, were included.
Outcomes
Studies were required to examine changes in suicide mortality in the presence of an intervention. Our primary outcome was the change in the number or rate of intentional self-harm (suicide) deaths, defined as deaths coded to the International Classification of Diseases (ICD) intentional self-harm codes (eg, code ICD-10: X60-X84, Y87) or determined to be due to intentional self-harm, using vital statistics or other death databases, or coroner’s or medical examiner’s records. Suicide death data could be expressed as counts, proportions or rates.
Study design
Cross-sectional, time series, retrospective, prospective, and pre–post study designs were included. This includes natural experiment designs, where the intervention is implemented outside of the control of the researcher.
Publication status and language
Studies were eligible if they were published in peer-reviewed journals in English or French as translation resources were limited to these two languages. We excluded non-peer-reviewed papers, theses, dissertations, government reports, conference proceedings and any other form of grey literature.
Search strategy
The search strategy was developed by a librarian experienced in systematic review searching. It was peer reviewed by a second librarian using the Peer Review of Electronic Search Strategies guideline. The searches were first conducted on 4 April 2018, across three databases: MEDLINE (Ovid), PsycINFO (Ovid) and Embase (Ovid). Date restrictions were placed on the search to include papers indexed from 1 January 1990 to 31 December 2017. An updated search was conducted on 12 February 2020 to extend the search to include articles from 1 January 2018 to 13 February 2020. The search used a combination of unique subject headings and keywords related to universal suicide prevention interventions. A filter was used to restrict articles to include only 33 high-income OECD countries. See online supplemental file 2 for the final search strategy. Additionally, studies were identified by searching the reference list of included studies and other relevant published reviews.
Supplemental material
Study selection
All of the database records were imported into RefWorks (V.2.0; ProQuest, Ann Arbor, Michigan, USA) to organise and deduplicate records. All records were then imported into Covidence (Veritas Health Innovation, Melbourne, Australia), with a second software deduplication performed before screening. At level one screening, at least two reviewers (JJL, BO and M-CI) independently screened titles and abstracts against the inclusion criteria, with consensus needed for level two inclusion. At level two screening, full texts of each record were obtained and independently screened by at least two reviewers (JJL, M-CI and HS-K), with consensus needed for final inclusion. A third reviewer (HO and JJL) helped resolve discrepancies when agreement was not attained during level one and two screening. Reviewers were not blinded to the authors of the studies.
Data extraction
Data from all included studies were extracted into a standardised spreadsheet that was peer reviewed by coauthors and pilot tested before use. All data were extracted by one reviewer (M-CI or HS-K) and verified by a second (HO or JJL). Disputes were resolved during research team meetings.
Extracted data included the following items: author, publication year, country, study design, estimated target population size, intervention description, intervention period (calendar years), level of intervention (national, regional, community), description of mortality outcome data, source of mortality data, intervention results (eg, preintervention and postintervention results or differences/changes in mortality), comparator details if available, method of statistical analysis and summary of findings.
Study quality assessment
The Effective Public Health Practice Project (EPHPP) Quality Assessment Tool was used to assess the quality of all included studies.26 One reviewer (M-CI and HS-K) independently evaluated each study for biases related to sample selection, study design, confounders, blinding, data collection, withdrawals, and dropouts. Each study received a global rating of ‘weak,’ ‘moderate’ or ‘strong’ based on the amount of potential bias incorporated into the study methods. A second assessor (JJL and M-CI) reviewed the evaluation for accuracy, with a third reviewer (HO) consulted to resolve conflicts. The EPHPP does not allow for grading the overall quality of the evidence for each intervention category. However, we highlight the range of global ratings for studies included in each intervention category.
Narrative synthesis of results
To help organise the results, studies were grouped into six broad categories of universal interventions derived from the WHO Comprehensive Mental Health Action Plan.11 The categories include access to healthcare (eg, suicide prevention centres), communication (eg, media reporting), community-based interventions (eg, school and community-based programmes and local suicide prevention projects/initiatives such as crisis phone lines), law and regulation reform (split into firearm laws and all other laws, such as alcohol policies, tobacco policies and access to all means, including domestic gas detoxification, catalytic converter legislation, analgesics and pesticides), mental health policies (eg, national programmes/strategies and mental health insurance policies), and physical barriers for transit and bridges (eg, bridge barriers, safety nets, blue lights on train stations, platform screen doors). Studies that included multiple interventions across several categories were included under the community-based interventions category. A narrative synthesis of results was conducted for each intervention category to describe the overall findings. The diversity of intervention types and settings within each category precluded our ability to perform a meta-analysis.
Results
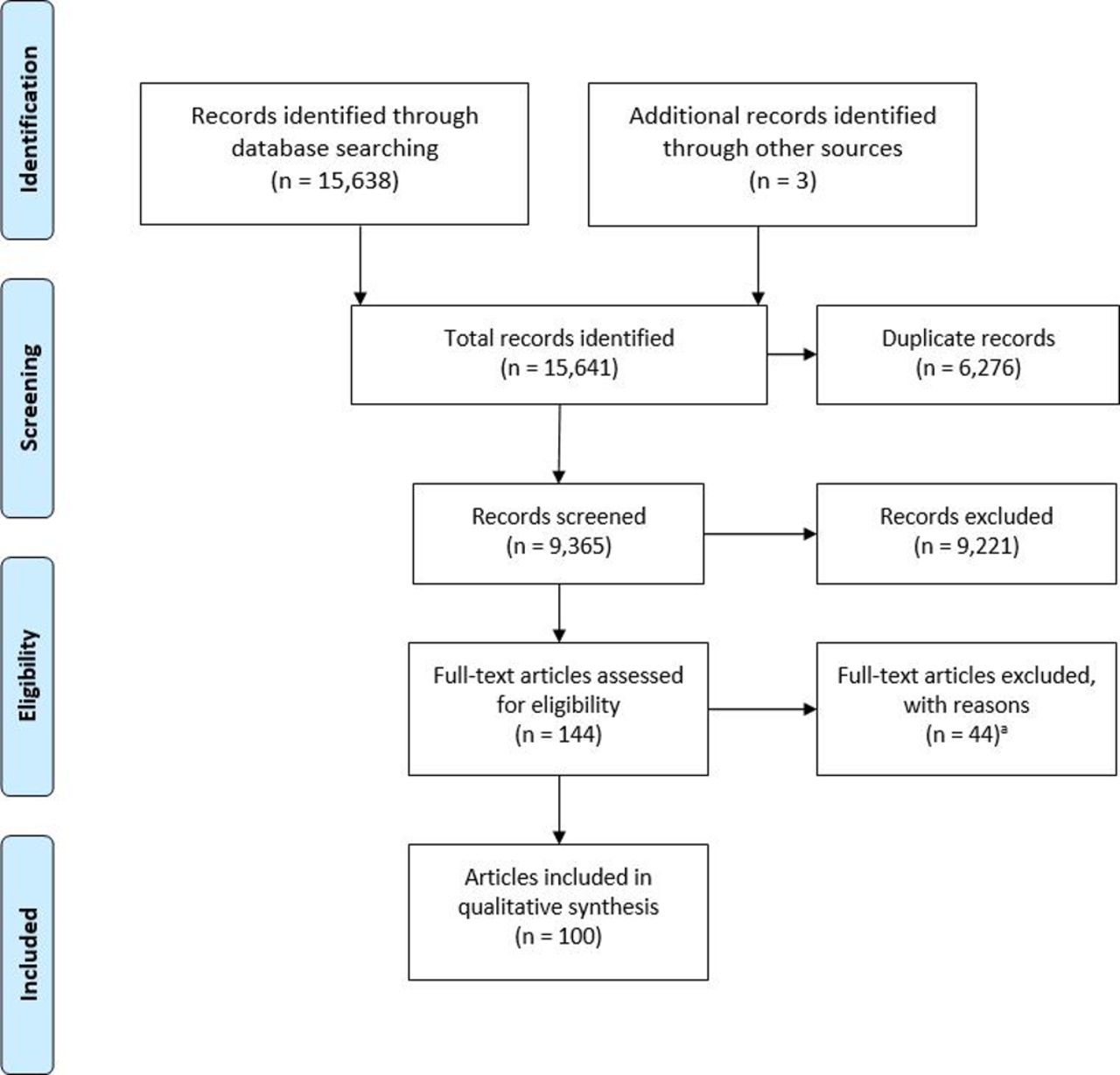
Figure 1 displays the PRISMA flow diagram for the literature search and screening process. A total of 15 641 records were identified through database searches and additional sources. After deduplication, 9365 records remained for level one screening. Following screening of titles and abstracts, 144 full-text articles were retained for level two screening, with 100 studies identified as eligible (see online supplemental file 3 for references).
Supplemental material

{kind=link}
PRISMA flow chart for the identification, screening, eligibility and inclusion of articles. aReasons for exclusion: 18 studies were not peer-reviewed articles; 9 studies did not evaluate a universal suicide prevention intervention; 11 studies did not use suicide mortality as an outcome; 2 studies were not conducted in a high-income OECD country and 4 studies did not have the full-text article available. OECD, Organisation for Economic Co-operation and Development; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The included studies were published from 1 January 1990 to 13 February 2020, with only 15% published in the past 5 years. Studies were conducted among 17 (47%) high-income OECD countries; the number of studies per country ranged from 1 (six countries) to 23 (one country). The most studied countries included the USA (23%), Australia (12%) and Canada (10%).
The majority of included studies (n=66) investigated law and legislation reform interventions (eg, alcohol and tobacco taxes, catalytic converter legislation, laws banning the use of pesticides, etc), with 45 out of the 66 studies investigating firearm-related law interventions. For firearm restriction laws, the most common topics of study were the US Brady Handgun Violence Prevention Act, the Australian National Firearms Agreement (NFA) and the Canadian Bills C-51 and C-17. Thirteen studies investigated physical barriers for suicide prevention (eg, installed on bridges or other jumping sites, train stations), nine investigated community-based interventions (eg, one intervention focused on improving the care of patients with depression by training family doctors, conducting media and general public campaigns, using community facilitators and fostering self-help activities), four investigated communication strategies (eg, media reporting and public awareness campaigns), seven reported on mental health policies and strategies (eg, a new suicide prevention policy) and one investigated access to healthcare as a method to prevent suicide. Tables 1–5 and online supplemental files 4–5 display details on all studies included in this review.
Supplemental material
Supplemental material
Access to healthcare
Communication strategies
Mental health policies and strategies
Physical barriers
Overall summary of findings
The overall summary of the findings is outlined in table 5. Thirteen (100%) physical barrier studies reported favourable results, as did two of four (50%) communication strategy studies, and three of nine (33%) community-based interventions. In total, 46 of 66 (70%) law and regulation reform studies reported favourable results, of which 30 of 45 (67%) firearm-related studies reported favourable results. Several specific interventions were the topic of multiple papers. The proportion of studies reporting a novel intervention was 75% for communication strategies, 78% for community-based interventions, 44% for law and regulation reform, 100% for mental health policies and strategies, and 85% for physical barriers. The study-specific quality assessment ranged from weak to strong, depending on the intervention category. Details on the study quality assessment scoring can be found in online supplemental file 6.
Supplemental material
Discussion
The WHO comprehensive framework launched in 2014 emphasised the importance of using a range of suicide prevention strategies (including universal, selective and indicated interventions),11 at different levels based on the unique situation and distribution of risk factors in each country. Relatively few studies have examined the effectiveness of universal suicide prevention interventions, with many doing this in combination with selective and indicated interventions. To the best of our knowledge, this is the first systematic review to examine the effectiveness of universal suicide prevention interventions with suicide mortality as the outcome.
Overall suicide mortality
This systematic review examined results from 100 studies conducted in 17 high-income OECD countries that investigated the association between specific universal suicide prevention interventions and changes in suicide mortality. Overall, we found that the relationship between universal suicide prevention interventions and reductions in suicide mortality varied largely depending on the type of intervention. We found that nearly all physical barriers interventions (100%) were effective at reducing suicide mortality at specific sites. The majority of the included studies in our study investigated law and legislation reform interventions, with roughly three-quarters (70%) of the included studies showing significant reductions in suicide mortality. Due to the reach of these interventions, they should be considered an important component of universal suicide prevention. Previous reviews have reported similar results by demonstrating that the most promising universal interventions were laws and legislative reforms restricting means to suicide (eg, guns, domestic gas, barbiturates, vehicle emissions, analgesics, pesticides, etc) and the control of locations frequently used for suicide by jumping (eg, physical barriers).20 21 Similar to other reviews, limited evidence demonstrated the effectiveness of communication strategies (eg, general public education and media guidelines) or community-based interventions (multilevel interventions) on suicide mortality. In our review, community-based interventions were often multi-level making it difficult to identify which specific components of the intervention had direct impacts on suicide mortality. Also, the evaluation of some of the community-based interventions combined suicide attempts and suicide deaths, further complicating the comparability of findings. In our review, we also included a broad range of interventions, such as healthcare access interventions and mental health policies (eg, national strategies, plans, health insurance policies). These types of interventions had limited impacts, except for mental health policies, which were significantly effective among specific age categories.
Sex-stratified results
Overall, there was more evidence supporting the effectiveness of universal suicide prevention interventions among males compared with females. Of the 27 studies that reported sex-specific effects, eleven (41%) found strong evidence of reductions in suicide mortality for males, but not for females (S1, S18, S29, S32, S33, S44, S79, S81, S83, S87, S100). While 12 (44%) reported equal effectiveness between males and females (S5, S11, S16, S17, S20, S23, S30, S43, S54, S55, S60, S85) and 4 (15%) reported effective results for females only (S7, S22, S42, S84). In Western contexts, more females attempt suicide, while more males die by suicide. This is known as the ‘gender paradox’ of suicide.27 The greater number of studies with positive results for males may be due, in part, to the significantly higher levels of suicide death among males and the greater power to detect significant effects. It is also possible that different types of interventions may be effective for females as compared with males, particularly as they relate to means restrictions. For example, while means restrictions interventions have been widely applied to more violent forms of suicide which are more common among men, including firearm suicide and jumping from heights, means restriction for some methods more common among women, such as poisoning by drugs,28 29 may be somewhat more challenging to implement. Finally, it is possible that the use of coroner or medical examiner data, which have been shown to have a lot of missing data, particularly for antecedents of suicide attempts and recent events that could have precipitated the suicide,30 31 explain at least in part the presence or absence of sex differences across studies. Future research using additional information, such as those collected from the psychology of death, is necessary to disentangle sex and gender differences in the universal suicide prevention interventions’ effectiveness. Regardless, research on universal suicide prevention interventions’ effectiveness should continue to apply a sex and gender lens.
Substitution hypothesis
In this review, 17 studies examined whether restricting suicide means from one method would result in an increase in suicide from other methods, described as the ‘substitution hypothesis’.32 However, findings from those studies are mixed, with eight studies providing evidence to supporting a substitution hypothesis (S19, S25, S26, S38, S54, S55, S90, S93), and nine studies not yielding such evidence (S36, S44, S48, S88, S89, S91, S96, S98, S100). For example, Klieve et al found that when the firearm suicide rate for Australian males declined following the introduction of restrictions on weapon purchases, the rate of suicide death by hanging increased simultaneously (S38). Similarly, Caron et al found that the firearm suicide rate decreased among males in Quebec (Canada) following the implementation of Bill C-17, while the rate of suicide death by hanging increased simultaneously (S55). Conversely, Lester and Leenaars (S50), Carrington et al (S51) and Leenaars and Lester rejected the substitution hypothesis (S52). They found that firearms were not replaced by other methods for suicide following passage and enforcement of Canadian Bill C-51. Several factors could explain these discrepancies, such as the availability of the method of suicide and study methodology. Duration of the follow-up may also explain these mixed findings across studies. For example, Sinyor et al demonstrated that by extending the follow-up period by seven additional years from a previous study (S90), the substitution hypothesis was no longer supported for suicide mortality by other means (S91). There is also the potential for individuals to switch from one method to another based on availability of means, and based on acceptability and country-specific sociocultural norms that may influence the use of other suicide methods.33 34
Years of follow-up
The historical period of our included studies ranges from 1907 to 2020, and consequentially, the length of follow-up across the studies, from less than 5 years (short term), to 20 years and longer (long term). In our review, six studies examined both the short-term and long-term association of the intervention and suicide mortality (S7, S14, S47, S56, S57, S91). Stack et al (S14), examined the short-term and long-term trends in suicide following a crisis phone line intervention to reduce suicide by jumping at the St.Petersburg (Florida) Skyway bridge. They found that over the short term (2 years), there was no impact of the intervention, while 13 years after the intervention, suicide mortality increased, suggesting the need for a more substantial intervention. Sinyor et al (S90), investigated the effectiveness of an intervention to reduce access to a jumping point in Toronto (Canada) with 3 years of follow-up, and found that the intervention, although effective, led to an increase in suicide mortality by other means in Toronto. However, in a 7-year follow-up, the authors found that the intervention was, in fact, more effective in the long term (S91). This suggests that some universal interventions might not be short-term solutions, as they may be more likely to be effective in the long-term period. The lower base rate of suicide mortality may also result in few events over short-term periods, with longer follow-up being needed to have adequate power to detect significant effects. Many of the studies that have used short-term follow-up period (eg, (S56) and (S57)) found no statistically significant changes in suicide mortality. In contrast, many studies with longer-term follow-up periods (eg, (S47)) showed that suicide mortality was significantly lower after the intervention and over time (~10 years after implementation).
Sustainable Development Goals
Our systematic review highlights a number of universal interventions that hold promise for reducing suicide mortality, such as law and legislation reforms and physical barriers. It is likely that to meet the SDGs to reduce suicide mortality rates, countries will need to take a multilevel approach that incorporates a variety of universal, selective and indicated interventions. Future research should focus on how universal interventions act in synergy with targeted and indicated approaches to reduce suicide mortality, identifying well-designed and transferrable interventions that can strengthen suicide prevention efforts within countries to meet the SDG target.
Strengths and limitations
The current systematic review has several strengths. First, we followed PRISMA guidelines to identify relevant studies, appraised the study-specific risk of bias (study quality assessment), and synthesised the results in a transparent, unbiased and reproducible manner. Second, the review captured a large number of studies on universal suicide prevention intervention published in English or French across 17 high-income OECD countries. Third, studies used a wide range of study designs with most of the primary data used in these studies being obtained from reliable sources (eg, vital statistics, coroners and medical examiners data). Fourth, we used the EPHPP Quality Assessment Tool to assess the quality of all included studies, this tool is widely used and designed to assess the quality of the evidence to support public health interventions and related research.26 Fifth, we ensured that studies evaluated the same interventions were identified to avoid ‘double-counting’ interventions. Sixth, while randomised controlled trials are considered the gold standard in intervention evaluation, this design would be regarded as unethical, not feasible politically, nor appropriate in the case of universal suicide prevention interventions.35 The natural experiments summarised in our study provide an excellent way to overcome the drawbacks of randomised controlled trials while still providing a way to study the impact of real-world interventions. Unfortunately, few studies evaluated concurrent universal interventions or interventions across multiple jurisdictions. Not all used a comparison group, but having a ‘control’ group without randomisation strengthened the study design in a number of cases. Finally, some studies used a repeated cross-sectional design, which is not as strong as longitudinal designs. There may be issues with internal validity because of unmeasured changes in the samples’ composition over time.
The quality of studies included impacts the confidence of the conclusions derived by a systematic review. The current systematic review included a large and diverse number of studies from around the world, providing more confidence to our findings. Second, due to heterogeneous data, we were unable to perform a meta-analysis to identify the pooled effects for each category of universal suicide prevention interventions. Third, the present systematic review did not identify any significant differences in intervention effectiveness by race, ethnicity, or immigration status, which represent important areas of future research. Fourth, we did not include studies published before 1 January 1990, and as a result, we may have missed some important studies published before this date. However, it is important to note that this study included many interventions implemented prior to 1990, but evaluated and published after 1990. Additionally, the policies enacted during these times may have less relevance in more recent contexts. We also may have missed important studies conducted in countries outside of the high-income OECD context. Finally, it is important to recognise the variability and incomplete nature of the information collected by coroners and medical examiners within and between countries,30 31 particularly on antecedents of suicide attempts and recent events, that could have precipitated the death by suicide.
Conclusions
This systematic review among high-income OECD countries found that universal suicide prevention interventions, especially those that include physical barriers and law and regulation reforms, were largely effective in reducing suicide mortality among the countries included in this study. While they are generally effective, their success widely varied by intervention type, follow-up period and sex. When investigating universal suicide prevention interventions, researchers should make an effort to stratify results by sex and to investigate the short-term and long-term impact of the interventions.
What is already known on the subject
Suicide continues to be a leading cause of death worldwide, and a significant public health concern.
What this study adds
Universal suicide prevention interventions provide an effective means to reduce suicide mortality in high-income OECD countries.
Physical barriers and law and regulation reform interventions seem to hold the most promise in preventing suicide.
Acknowledgments
We would like to thank the library staff at the Health Canada Health Library for their help with developing and carrying out the search strategy for this study. We would like to thank Emily Wolfe Phillips, Dakota Gillies, and Maulik Baxi who helped with this study. In long-lasting memory of Patrick R. Quinn (1989-2017).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
M-CI and HS-K are joint first authors.
Twitter @heatherorpana
Contributors JJL conceived the idea and designed the study. JJL, BO and HO drafted the protocol. M-CI, BO and JJL participated in the screening level 1. M-CI, JJL, HO and HS-K participated in level 2 screening. M-CI, JJL and HO completed data extraction. M-CI, HS-K and JJL completed the risk of bias assessment. M-CI, JJL and HS-K drafted the first version of the manuscript. All authors participated in the preparation of the submitted manuscript.
Funding MSK’s work on this study was partially supported by a grant from the Fulbright Specialist Programme (FSP-P005326).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.