Article Text

Abstract
Initially, zolpidem, a non-benzodiazepine hypnotic agent, was considered to have fewer adverse reactions than traditional benzodiazepines. However, after zolpidem was approved for medical use, an increasing number of case reports have described abuse or dependence complications. We were especially interested in the cases of dependence that presented a paradoxical ‘euphoric’ effect of zolpidem. This article reports the case of a female zolpidem-dependent patient who presented with 6 years of daily use of 400–1400 mg of zolpidem. She reported subjective effects of euphoria, intense craving and the inability to stop drug ingestion. Her diagnoses were zolpidem dependence and a depressive episode induced by substance abuse. To explore the neural mechanisms of the euphoric effect caused by high-dose zolpidem, we performed repeated magnetoencephalography (MEG) recordings. Before undergoing detoxification, her MEG results indicated that cerebellar electrical signal activation increased when taking high zolpidem doses. However, the prefrontal and parietal lobes’ electrical signal activity showed a tendency to recover to a normal state as the withdrawal time progressed to completion. This case suggests that the cerebellum plays a role in the euphoria induced by high zolpidem doses and provides clues for further research.
- psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Zolpidem, a non-benzodiazepine hypnotic agent, is recommended in guidelines as a first-line treatment for insomnia: ‘We suggest that clinicians use zolpidem as a treatment for sleep onset and sleep maintenance of insomnia (vs no treatment) in adults’.1 Compared with traditional benzodiazepines, zolpidem is a powerful selective agonist of the ω1 receptor subtype of the γ-aminobutyric acid A (GABAA) receptor complex.2 Classical benzodiazepines have a non-specific affinity for the BZ1 (ω1) and BZ2 (ω2) receptors of the GABAA receptor.3 Thus, zolpidem is considered to have fewer adverse reactions than benzodiazepines. However, since zolpidem was approved for medical use, an ever-increasing number of case reports describe abuse or dependence complications. To our knowledge, 80 cases of zolpidem dependence have been reported in the literature thus far4; in these reports, zolpidem doses ranged from 10 to 2000 mg daily.5 Among the various reported effects of the drug, we were especially interested in the paradoxical ‘euphoric’ effect of zolpidem. This effect was also found with other benzodiazepines—occurring in less than 1% of the participants of large epidemiological studies who used this drug.6
Magnetoencephalography (MEG) performs non-invasive functional imaging by recording magnetic flux on the head’s surface associated with electrical currents in activated sets of neurons. Since MEG uses neuromagnetic signals that penetrate the skull and scalp without distortion, it provides a method to gain evidence for understanding the neural mechanisms of the euphoric effect caused by high-dose zolpidem. This article reports the case of a female zolpidem-dependent patient whose MEG was measured periodically throughout her drug withdrawal treatment. Our aim was to explore the phenomenology of the zolpidem stimulant effect and its underlying mechanisms.
Case report
Herein, we present the case of a 23-year-old woman hospitalised for zolpidem abuse with depression. We have organised our case report according to the CARE (for CAse REport) guidelines.7
Case presentation
The patient was a 23-year-old Han Chinese woman hospitalised twice to treat her addiction to zolpidem. Six years ago, when the patient had poor sleep due to the pressure of school examinations, her psychiatrist prescribed zolpidem (Stilnox) 5 mg/night for bedtime insomnia. The patient accidentally discovered that higher doses of zolpidem could induce a state of euphoria. Seeking more of the euphoric effects, she took the drug daily, increasing the dosage over time. While 30–40 mg of zolpidem triggered a feeling of pleasure, higher doses induced a sense of euphoria, which was more likely to occur if taken on an empty stomach. This feeling would appear approximately 20 min after ingestion and last for several hours. The patient felt joyfully wild during the euphoric period and experienced increased activity, incessant talking, reckless behaviour and grandiosity. Taken without self-control, the increasing amounts of zolpidem disrupted her circadian rhythm; she remained awake and ‘high’ throughout the night, carrying out various activities, boasting while calling her friends, playing online games and so forth. In addition, the patient experimented with other sleeping pills, such as zopiclone, alprazolam, lorazepam, diazepam and so on, but none of them induced similar euphoric feelings.
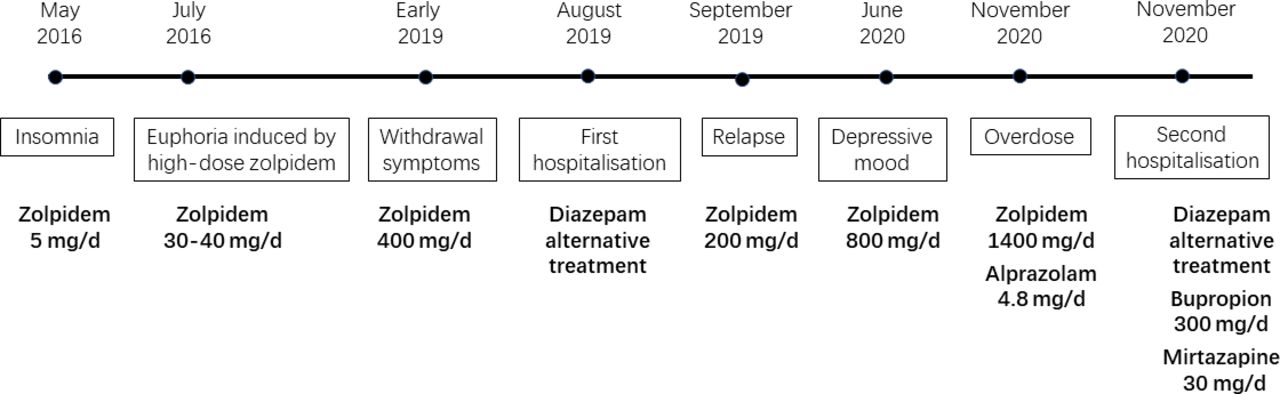
One year ago, the patient developed withdrawal symptoms and increased her zolpidem intake to 400 mg/day. At this point, she had to spend much time and money procuring the additional zolpidem drugs. Unable to get a sufficient supply from hospital pharmacies, the patient bought the medication at high prices online, often borrowing money from friends and stealing her parents’ credit cards. The patient was hospitalised for the first time in August 2019 to treat zolpidem addiction because of her impaired memory. During the 14-day hospitalisation, diazepam—the selected replacement drug for treatment—was progressively reduced from 30 mg/day to its discontinuation. Two weeks after hospital discharge, the patient again took zolpidem and rapidly increased the dose to 200 mg/day. By June 2020, the patient showed persistent depressive mood and had made some suicide attempts. She began smoking and soon consumed 40 cigarettes/day, simultaneously raising her zolpidem intake to 800 mg/day. Unable to obtain enough zolpidem, the patient substituted diazepam every 4 or 5 days, taking approximately 20 mg of diazepam three to four times per day but still manifesting withdrawal symptoms of zolpidem during this period. In November 2020, she was hospitalised for suicidal risk and massive zolpidem intake. Three days before admission, the patient had taken zolpidem 1400 mg and alprazolam 4.8 mg. The patient had no other substance abuse history, physical disease history or family history of mental illness or substance abuse (For timeline, see figure 1).

Case report timeline: patient’s zolpidem exposure, addiction and treatment process.
Investigation
During the initial evaluation, 12 hours post-drug intake, the patient presented obvious withdrawal symptoms—tremor, sweating, palpitation, nausea and dysphoria. Diazepam 10 mg was immediately administered for symptom reduction. One hour after treatment, the patient was evaluated with the Clinical Institute Withdrawal Assessment-Benzodiazepines (CIWA-B),8 receiving a score of 33, which meant moderate withdrawal. Her blood count, liver function, renal function, serum electrolytes, serum prolactin, hormones, thyroid function tests and urinalysis were normal. Her physical examination and electrocardiogram (ECG) were also normal. Laboratory tests were unable to detect zolpidem plasma. The patient was assessed with several psychiatric measures, including the Zung Self-Rating Depression Scale9 (SDS; score 65), the Zung Self-Rating Anxiety Scale10 (SAS; score 43) and the Mini-Mental State Examination11 (MMSE; score 29). Brain magnetic resonance imaging MRI was conducted without abnormal findings. Additionally, we used MEG to detect changes in the patient’s brain activity which was detailed in later sections.
Diagnosis
Based on our clinical judgement and investigation, which used the criteria of the International Classification of Diseases 10th Edition (ICD-10),12 we retained the patient’s original diagnosis of zolpidem dependence. A second carryover diagnosis was a depressive episode induced by substance abuse.
Treatment
During the 17-day hospitalisation, we selected diazepam for drug replacement treatment, progressively reducing its dose from 40 mg/day to discontinuation. The depressive episode was relieved by administering bupropion 300 mg/day and mirtazapine 30 mg/day.
Outcome and follow-up
After 5 days of treatment, the patient’s withdrawal symptoms had entirely disappeared. However, she still presented obvious depressive symptoms, suicidal ideation and insomnia. After 17 days of hospitalisation, the patient asked for discharge and agreed to continue bupropion 300 mg/day and mirtazapine 30 mg/day at home. For relapse prevention, follow-up appointments with a psychiatrist were scheduled; the patient insisted on having regular outpatient visits. Lithium carbonate was added to her medical regime to treat her depressed mood. Her depression was relieved 3 months after discharge. The patient relapsed twice in the ensuing year but was managed well in outpatient treatment.
Magnetoencephalography
The MEG procedure
The MEG recordings were acquired inside a magnetically shielded room by a total of 306 channels, using a helmet-shaped, whole-head system (VectorView, Elekta Neuromag Oy, Finland) comprising 102 locations in triplicate. The system included one magnetometer and two orthogonal planar gradiometers. Continuous data were recorded for this patient at a sampling rate of 1000 Hz for the MEG signal. Each recording consisted of 5-minute epochs while the patient sat in a resting state at a 60-degree position with eyes closed. A Polhemus three-dimensional digitiser system (Colchester, Vermont, USA) was used to determine the location based on anatomical fiducial points (nasion and bilateral preauricular points) for the following MRI-MEG co-registration. By checking the uniform distribution of points—to the extent possible—in an area covering the whole scalp, the head shape of each patient can be ascertained. We had ensured that our patient’s head did not move during the entire procedure. Finally, we used the FieldTrip toolkit13 to implement source localisation based on a frequency domain beamforming method called dynamic imaging of coherent sources (DICS).14 15
The research process
The patient’s baseline MEG (MEG_S1) was taken on the morning of the second day after admission. Her diazepam dose was 10 mg four times per day at that time. The patient still presented withdrawal symptoms, such as trembling, sweating, depression and palpitation. Her CIWA-B score was 23. After the MEG_S1, the patient was given zolpidem 30 mg. Twenty minutes later, the patient felt ‘tipsy’, happy and relaxed with no tremor. Then her CIWA-B score was 13. A second MEG (MEG_S2) was performed immediately. On the morning of the 15th day after admission, the final MEG scan (MEG_S3) was conducted. At that time, the patient was taking diazepam 5 mg/night, mirtazapine 15 mg/night and bupropion 150 mg twice per day. Her assessment scores were SDS=71, SAS=46 and CIWA-B=13 (see table 1).
Comparison of three MEG scans during clinical treatment
Data analysis
MEG signals with continuous data, divided into many 10-second segments, were filtered using a band-pass filter of 0.5–60 Hz, notch-filtered at 50 Hz, and detrended by removing the linear trend from the data. The noisy MEG channels were detected using the manual artefact rejection module, and the faulty channels were repaired automatically using a spline interpolation algorithm. Improving SNR (signal-to-noise ratio) as much as possible, independent component analysis was used to remove artefacts related to heartbeats and eye blinks. Time-frequency analysis was then used to explore the frequency band of interest, such as beta, with a centre frequency of about 18 Hz. The calculation procedure of the power difference of MEG sources between the S1 state and the S2 state followed. We first used the DICS method16 to run the analysis based on the MEG data of each state. Then, the values were calculated by using the powers of the S2 state minus the powers of the S1 state. If the values were mainly positive, source locations were displayed directly on MRI T1. Otherwise, source locations corresponding to the absolute values of those negative values were displayed on MRI T1.
Results
Comparing MEG_S2 to MEG_S1
Comparing the MEG data before and after zolpidem intake, increased activity was observed clearly in the left and right cerebellum (figure 2A) after the ingestion. Changes in the patient’s clinical presentation included the disappearance of withdrawal responses and the onset of euphoria. The patient felt happy, relaxed and no longer experienced tremors. The MEG results suggested that the cerebellum may be involved in these changes.

{kind=link}
{kind=link}
Comparison of three MEG scans. (A) MEG_S2–MEG_S1: Comparing the baseline MEG data before and after a high-dose intake of zolpidem, clear increased activity was observed in the left and right cerebellum. (B) MEG_S3–MEG_S1: Comparing the follow-up and baseline data of MEG, decreased activity was observed in the left frontoparietal junction. MEG, magnetoencephalography.
Comparing MEG_S3 to MEG_S1
The final MEG recording was taken on day 15 of hospitalisation. By then, the patient’s withdrawal symptoms had disappeared entirely. Comparing the data of the baseline and final results, the final MEG showed decreased activity in the prefrontal and parietal lobes (figure 2B). Many confounding factors influenced this change, including various treatment drugs, withdrawal reactions, mood changes and so forth, so the detoxification process can only be roughly understood.
Discussion
This article reported the clinical characteristics of a female zolpidem-dependent patient experiencing drug-induced euphoria, the course of her detoxification, and the results of MEG recordings during this treatment. The MEG results indicated that cerebellar electrical signal activation increased when taking high zolpidem doses during the addictive phase. In addition, the prefrontal and parietal lobes’ electrical signal activity showed a tendency to recover as the withdrawal time progressed to completion.
Our case described a rapid onset of zolpidem-induced euphoric effect within 20 min of drug ingestion and lasting several hours. In other case reports, patients described the rapid onset of zolpidem-induced euphoric effects within less than 15 min of drug ingestion, with duration ranging from 15 min to 3 hours.4 In addition, a few cases also reported a zolpidem-induced, manic-like effect.4 17 It is noteworthy that our patient had developed depressive symptoms and suicidal ideation after 6 years of zolpidem abuse. The confounding relationship between depression and zolpidem is worth considering. In data released by the Food and Drug Administration(FDA), modern hypnotics, including zolpidem, have been associated with an increased incidence of depression.18 However, some studies have demonstrated a significant association between zolpidem use and suicidal ideation or suicide attempt in people with or without comorbid psychiatric illness.19 20 However, a separate study demonstrated that zolpidem prescriptions did not contribute to an increased risk for suicide attempts.21 In summary, individuals with depressive disorders who experience anxiety and insomnia are susceptible to zolpidem abuse; this can progress to ever-increasing self-dosage and dependence on the drug. On the other hand, individuals who take zolpidem for long-term treatment of severe and chronic insomnia are prone to depression and potentially at a higher risk of suicide.
In this case, the patient’s continual search for a euphoric state led to her zolpidem abuse and eventual addiction. MEG assisted our understanding of the neural mechanisms of the euphoric effect caused by high-dose zolpidem by locating the affected brain areas. Our study demonstrated that the cerebellum electrical signal activation increased after the onset of zolpidem induced-euphoria. Zolpidem appears to have a selective action on the ω1 subtype of GABAA receptors22; these receptors are mainly distributed in the cerebellum, sensorimotor cortex, substantia nigra, cerebellar flocculus, olfactory bulb, ventral part of thalamus, pons and globus pallidus. In our case, the euphoria induced by high zolpidem doses was associated with abnormal activity in the cerebellum. This finding differs from the results of previous psychoactive drug-response studies. Acute doses of various abused drugs have produced relative increases of brain activation in specific regions, such as the anterior cingulate, thalamus, amygdala, basal ganglia, orbitofrontal cortex, basal forebrain and ventral tegmental area,23–25 but not in the cerebellum. One possibility for the disparity in findings is that our patient’s neuroplasticity may have changed after taking high doses of zolpidem over the extended time of 6 years. However, this could not explain why the patient presented with a euphoric effect upon receiving the first high dose of zolpidem during our observations. Another possibility may be a GABAergic dysfunction within the patient. The expression of GABAA α2, β1 and ε receptors has been found to be significantly altered in the lateral cerebellum of subjects with schizophrenia, major depression and bipolar disorder.26
Also, noteworthy, this patient’s development of zolpidem dependence reflected several failings: (1) a delay in recognising the self-administration of zolpidem without physician guidance, (2) easy access obtaining controlled medications from various doctors and other channels and (3) the lack of family supervision over the patient’s medication use. The above points should be heeded as warnings to prevent further zolpidem addiction. The International Narcotics Control Board lists zolpidem and most benzodiazepines as Schedule Ⅳ drugs. In China, sedative and hypnotic drugs belong to Category Ⅱ of Psychotropic Drugs and are subject to strict drug administration. Unfortunately, relying solely on the strict measures of medical control and management to prevent abuse and addiction of these drugs carries high financial costs. However, any change in guidelines to promote more rational use of these drugs demands additional scientific evidence and more effective clinical measures. MEG offers one means to define better the neural mechanisms of mental behaviour disorders caused by zolpidem, thereby potentially identifying those more vulnerable to addiction.
Results of the three MEG recordings detailed in this study reflected changing states of the patient. However, the major limitations of this study are that it involved only one patient and it lacked measures of cognitive performance. In addition, since MEG can only determine energetic increases or decreases and it is not clear whether the discovered activity was inhibitory or excitatory, the significance of the MEG results is difficult to explain. In addition, the study did not test zolpidem plasmatic concentration during the intervention, nor did we use a rating scale to measure the patient’s euphoria. Furthermore, the maximum zolpidem administered in our study was only 30 mg. This dose was much lower than usually needed to induce a euphoric effect—about 200–300 mg per dose. Nevertheless, the 30 mg dose of zolpidem still induced a ‘tipsy’ state for this patient, an opposite reaction to zolpidem’s claimed sedation effects. Therefore, we believe that the MEG findings attained after the small 30 mg dose of zolpidem mirror the stimulant effect induced by higher zolpidem doses. But also to be noted, the 30 mg of zolpidem administered for the second MEG scan replaced a single dose of diazepam—chosen for ethical reasons—that the patient was receiving at that time. Finally, the concomitant administration of benzodiazepines during the intervention could have impacted the results.
Conclusion
The use of zolpidem, which previously was considered relatively safe, can also lead to dependence and severe abuse. In addition, this case suggests that the cerebellum plays a role in the euphoric effect induced by high zolpidem doses, thus providing clues for further research.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Ethics Committee of Shanghai Mental Health Center(ref. no.: 2020-95). Participants gave informed consent to participate in the study before taking part.
References
Xuechan Lyu obtained a MD degree in psychiatry from Shanghai Jiao Tong University, China, in 2017. At present, she is working as a psychiatrist at Shanghai Mental Health Center in China. Her research interests include substance use disorder and behavioral addiction.

Footnotes
XL and YH contributed equally.
Contributors XL, YH, YZ, HW, JD and HJ contributed to study concept and design. XL and YH performed the data analyses and wrote the manuscript. JW and HJ contributed to study supervision. All authors have full access to all data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This work was supported by Clinical Research Center, Shanghai Jiao Tong University School of Medicine (DLY201818), National Natural Science Foundation of China (81901832), Program of Science and Technology Innovation Plan in Shanghai (18411961200, 19ZR1477800), Clinical Research Plan of SHDC (SHDC2020CR4066), Shanghai Key Laboratory of Psychotic Disorders (13DZ2260500), Shanghai Mental Health Center Foundation (2020-FX-01, 2021zd01). The sponsor did not have any influence on study design, collection, analysis and interpretation of data or in writing the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.