Article Text

Abstract
Background The impact of the COVID-19 pandemic on the population’s mental health is vital for informing public health policy and decision-making. However, information on mental health-related healthcare service utilisation trends beyond the first year of the pandemic is limited.
Aims We examined mental health-related healthcare service utilisation patterns and psychotropic drug dispensations in British Columbia, Canada, during the COVID-19 pandemic compared with the prepandemic period.
Methods We conducted a retrospective population-based secondary analysis using administrative health data to capture outpatient physician visits, emergency department visits, hospital admissions and psychotropic drug dispensations. We examined time trends of mental health-related healthcare service utilisation and psychotropic drug dispensations between January to December 2019 (prepandemic period) and January 2020 to December 2021 (pandemic period). In addition, we calculated age-standardised rates and rate ratios to compare mental health-related healthcare service utilisation before and during the first two years of the COVID-19 pandemic, stratified by year, sex, age and condition.
Results By late 2020, except for emergency department visits, utilisation of healthcare services recovered to prepandemic levels. Between 2019 and 2021, the monthly average rate for overall mental health-related outpatient physician visits, emergency department visits and psychotropic drug dispensations increased significantly by 24%, 5% and 8%, respectively. Notable and statistically significant increases were observed among 10–14 year-olds (44% in outpatient physician visits, 30% in emergency department visits, 55% in hospital admissions and 35% in psychotropic drug dispensations) and 15–19 year-olds (45% in outpatient physician visits, 14% in emergency department visits, 18% in hospital admissions and 34% in psychotropic drug dispensations). Additionally, these increases were more prominent among females than males, with some variation for specific mental health-related conditions.
Conclusions The increase in mental health-related healthcare service utilisation and psychotropic drug dispensations during the pandemic likely reflects significant societal consequences of both the pandemic and pandemic management measures. Recovery efforts in British Columbia should consider these findings, especially among the most affected subpopulations, such as adolescents.
- mental health
- COVID-19
- depression
- anxiety
- population surveillance
Data availability statement
No data are available. The DAD and COVID-19 databases were made available through British Columbia COVID-19 Cohort (BCC19C), a public health surveillance platform integrating COVID-19 data sets (testing, cases, hospitalisations, vaccinations) with administrative data holdings for the BC population (eg, medical visits, hospitalisations, emergency room visits, prescription drugs, chronic conditions, vital statistics). We are not permitted to share these data. BCC19C data are only available to researchers who request and meet the criteria for access.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
An increase in worsening mental health outcomes during the first year of the COVID-19 pandemic (2020) has been previously described, however, information on longer-term mental health-related healthcare service utilisation in 2021 is limited.
WHAT THIS STUDY ADDS
By triangulating data from four administrative health sources in the Canadian province of British Columbia, our study demonstrates that increases in mental health-related healthcare service utilisation and psychotropic drug dispensations became apparent only in 2021, most notably among adolescents and particularly females.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Findings from our paper can help inform public health measures both during and after pandemics, targeting priority populations with heightened vulnerability to worsened mental health outcomes.
Introduction
While coronavirus disease 2019 (COVID-19) directly resulted in considerable morbidity and mortality in British Columbia (BC), Canada, like elsewhere in the world, the pandemic and the ensuing public health response to control the disease also resulted in broader indirect impacts on the population health and well-being. In BC, these include changes in health behaviours,1 disruption to healthcare services2 and deterioration of many social determinants of health.1 In particular, significant pandemic-related mental health impacts arose as the population grappled with uncertainty, stress, social isolation and disruptions to routine activities of daily living. According to global studies, self-reported social isolation experienced throughout the pandemic has been associated with an increased likelihood of loneliness and deteriorating mental health.3–6 Financial uncertainties experienced during the pandemic have been related to psychological distress and mental disorders.7 8 Pandemic control measures likely contributed to worsening mental health outcomes, especially among certain groups: frail older adults, clinically highly vulnerable individuals and their caretakers, adolescents, girls, children living with physical disabilities or neurodiversity and those with pre-existing mental illnesses.3–6
Before the COVID-19 pandemic, declared in March 2020, data indicated a worsening trend of self-reported mental health conditions among Canadians. Based on analyses of nationally representative data from the Canadian Community Health Survey, between the early 2000s and 2016, there was a moderate increase in the prevalence of anxiety, specifically 4% and 7% among employed and unemployed Canadians, respectively.9 The lived experiences of the COVID-19 pandemic may have exacerbated symptoms of deteriorating mental health among the overall population; however, these effects may be disproportionately distributed among subpopulations with pre-existing vulnerabilities.
According to World Health Organization (WHO), during the first year of the COVID-19 pandemic, the global prevalence of major depressive disorder and anxiety disorders (AD) increased by 28% and 26%, respectively.10 Canadians overall reported lower self-perceived mental health during the COVID-19 pandemic, with the rates of excellent or very good mental health among Canadians 15 years of age and older decreasing by 14% compared with 2018.11 Residents of BC also reported considerable mental health impacts during the pandemic. In the BC Survey on Population Experiences, Action and Knowledge (SPEAK), an extensive cross-sectional population health survey, 46% of adult participants reported worsening mental health since the beginning of the pandemic,1 with the greatest impact among younger adults. Canadian youth, particularly, were less likely to report excellent or very good mental health during the pandemic.12 Young Canadians aged 15–24 appeared more likely to experience poor mental health outcomes than other age groups.10 The proportion of younger adults who were screened positive for depression and anxiety increased between fall 2020 and spring 2021.13 Similar trends among children and youth in BC have been reported.13
In contrast with the trends for self-reported mental health, numerous studies reported a decrease in mental health-related healthcare service utilisation at the initial stages of the pandemic,14–17 often followed by a subsequent increase as the pandemic progressed. Saunders et al16 reported a decline in physician-based mental health services in Ontario as of April 2020, followed by a 10%–15% growth to above-expected levels in the first quarter of 2021.16
In the current study, we characterised patterns of mental health-related healthcare service utilisation and psychotropic drug dispensations in BC during the COVID-19 pandemic (January 2020 to December 2021) compared with a prepandemic period (January to December 2019) using multiple administrative data sources. We used (1) outpatient physician (OP) visits; (2) emergency department (ED) visits; (3) hospital admissions (HAs); and (4) psychotropic drug dispensations. We hypothesised an increase in mental health-related healthcare service utilisation during the pandemic period compared with the prepandemic period.
Methods
Study design and setting
We conducted a retrospective population-based secondary analysis study of mental health-related healthcare service utilisation among residents of BC, Canada’s third most populous province (5.2 million in 2021).18 People 0–105 years of age with valid information on sex and age were included if they lived in BC between 1 January 2019 and 31 December 2021. January to December 2019, and January 2020 to December 2021 were defined as the prepandemic and pandemic periods, respectively. Because of the Canadian universal healthcare system, data sets used in this study captured nearly all BC’s all health-related OP and ED visits, HAs and drug dispensations in community pharmacies.
Data sources and ethical considerations
Deidentified data, that is, data without any personal information, were obtained from the British Columbia COVID-19 Cohort. This public health surveillance platform was established under the British Columbia Centre for Disease Control’s (BCCDC) public health surveillance mandate that integrates various administrative data sets (see online supplemental table S1). We used data from four different health administrative data sources: (1) BC’s Medical Services Plan (MSP) identified mental health-related OP visits; (2) information systems in regional EDs captured mental health-related visits; (3) the Discharge Abstracts Database (DAD) data source captured mental health-related HAs; (4) PharmaNet, which records all outpatient dispensations for drugs and medical supplies in community pharmacies across BC, supplied psychotropic drug dispensations. This analysis was conducted under BCCDC’s public health surveillance mandate to monitor the unintended consequences of the COVID-19 pandemic. Therefore, approval from a research ethics board was not required.
Supplemental material
Exclusions
During the 2019–2021 study period, we excluded OP records with missing, unknown or unassigned postal codes (n=14 315 (0.15%)) and those with absent or unknown sex (n=21 322 (0.22%)). To capture MSP claims only, OP visits that originated directly from referrals by midwives and nurse practitioners were excluded (n=20 113 (0.21%)). For OP tabulations, multiple visits in a single day were included and counted individually. Hospital transfers and readmissions within the first 24 hours of admission were calculated as the same admission (n=56 728 (4.20%)) to avoid double counting HAs. This methodology is described further elsewhere.19 HA records with missing, unknown or unassigned postal codes (n=1 448 (0.11%)) and records with missing or unknown sex (n=67 (<0.01%)) were excluded. Due to delays in abstraction and quality assurance of DAD, HA data for the month of December 2021 were not included in our analyses. ED records with missing, unknown or unassigned postal codes (n=3 937 (1.32%)) or records with missing or unknown sex (n=140 (0.05%)) were excluded. In addition, records for psychotropic drug dispensations with unassigned or missing postal codes (n=40 270 (0.10%)), missing or unknown sex (n=400 (<0.01%)) and missing or unknown age (n=381 (<0.01%)) were excluded.
Outcomes and statistical analyses
The MSP, ED and DAD databases used the International Classification of Diseases 9th Revision (ICD-9),20 the Presenting Complaint List codes (v.5.1)21 and the ICD-10-CA (Canadian enhancement), respectively.22 We identified mental health-related healthcare service utilisation using diagnostic codes validated elsewhere using BC data (see online supplemental tables S2 and S3).23 24 Diagnostic codes for mental health-related healthcare service utilisation were applied to extract relevant records prior to our analyses. For our analyses, psychotropic drug medications included antidepressants, antipsychotics, anxiolytics and sedatives (see online supplemental table S4).
Our primary outcomes were age-standardised and age-specific rates for mental health-related healthcare service utilisation and psychotropic drug dispensations (per 100 000 population for ED visits and HAs; per 1 000 population for OP visits and psychotropic drug dispensations). As per standard reporting, we used per 100 000 population rates for ED visits and HAs, and per 1 000 population rates for OP visits and psychotropic drug dispensations, respectively. This approach also makes it possible to compare our data to prior publications. We calculated rates using population denominators. We also calculated the monthly average rate ratios (RR), comparing 2019 and 2021. We used Poisson regression models to calculate 95% confidence intervals (CIs) for RRs. Finally, we calculated the per cent change in the monthly average rate of mental health-related healthcare service utilisation by dividing the absolute rate in 2021 over the absolute rate in 2019. Small changes in the average number of mental health-related healthcare service utilisations can result in inflated per cent change estimates; as such, we excluded absolute rates <1 for OP visits and psychotropic drug dispensations and <5 for ED visits and HAs. Results were stratified by sex, age and type of mental health condition. We categorised age into 12 groups: <5, 5–9, 10–14, 15–19, 20–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80–89 and 90+. When results were stratified by condition, sex and age, we suppressed data for HAs among <10 year-olds due to small cell counts. We used BC’s 2019–2021 population as the denominator and BC’s 2016 population as the standard population. Population estimates were attained from BC Stats Population Extrapolation for Organization Planning with Less Error 2020 projections.25 P values were calculated using the χ2 test, and the statistical significance threshold was set at <0.05. All analyses were performed using R V.4.1.2.
Results
Overall differences: prepandemic and pandemic periods
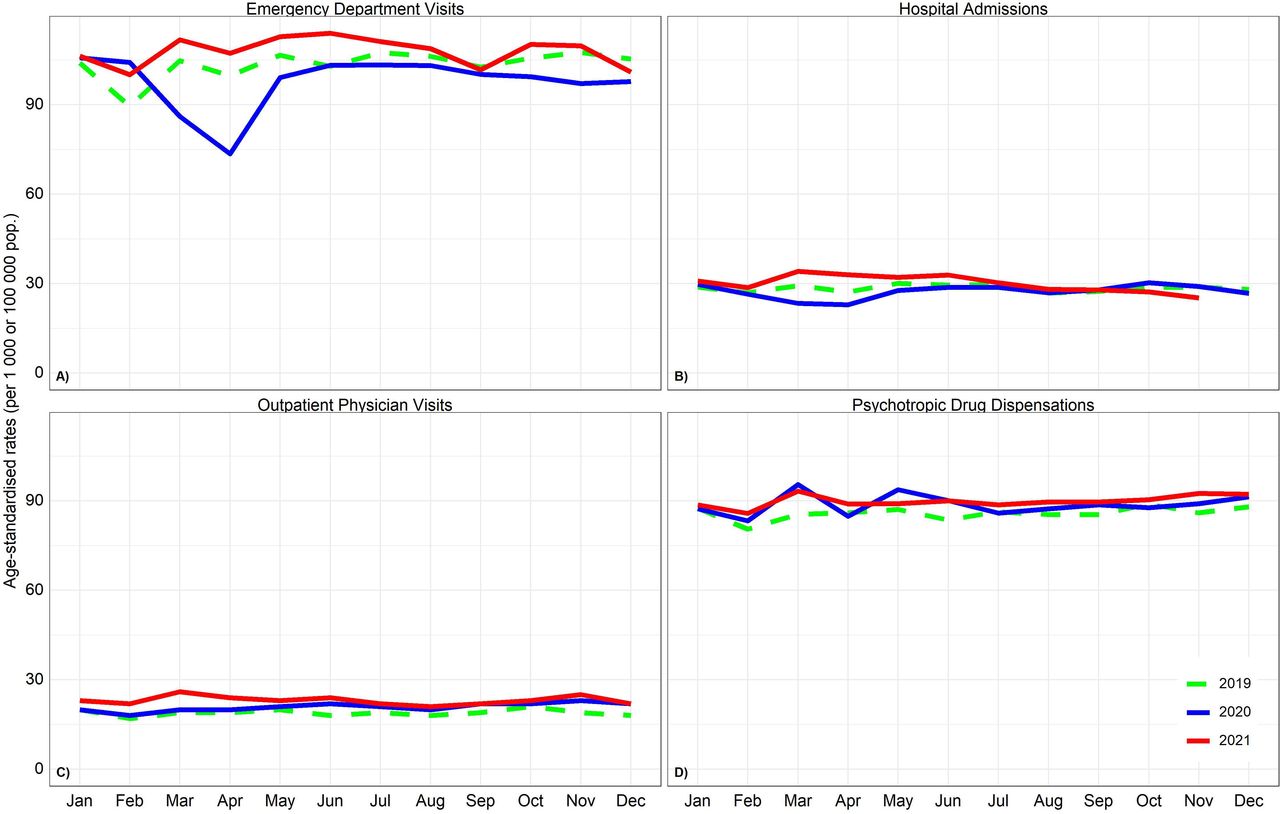
Figure 1 shows the selection of the study population. In April 2020, shortly after the onset of the pandemic, we observed a large and rapid decrease in acute mental health-related healthcare services such as ED visits and a slight decrease in HAs (figure 2). Figure 3 illustrates the relative change in the monthly rates of mental health-related healthcare service utilisation and psychotropic drug dispensations during the prepandemic period in 2019 and the pandemic period in 2020 and 2021. Between April 2019 and April 2020, statistically non-significant decreases in ED visits of 26% (99.8 to 73.5 visits per 100 000 population) and in HAs of 16% (27.2 to 22.9 admissions per 100 000 population) were found. By early 2021, the age-standardised monthly rate for mental health-related healthcare service utilisation and psychotropic drug dispensations surpassed 2019 rates. It remained elevated for the year’s first two quarters (figure 2).
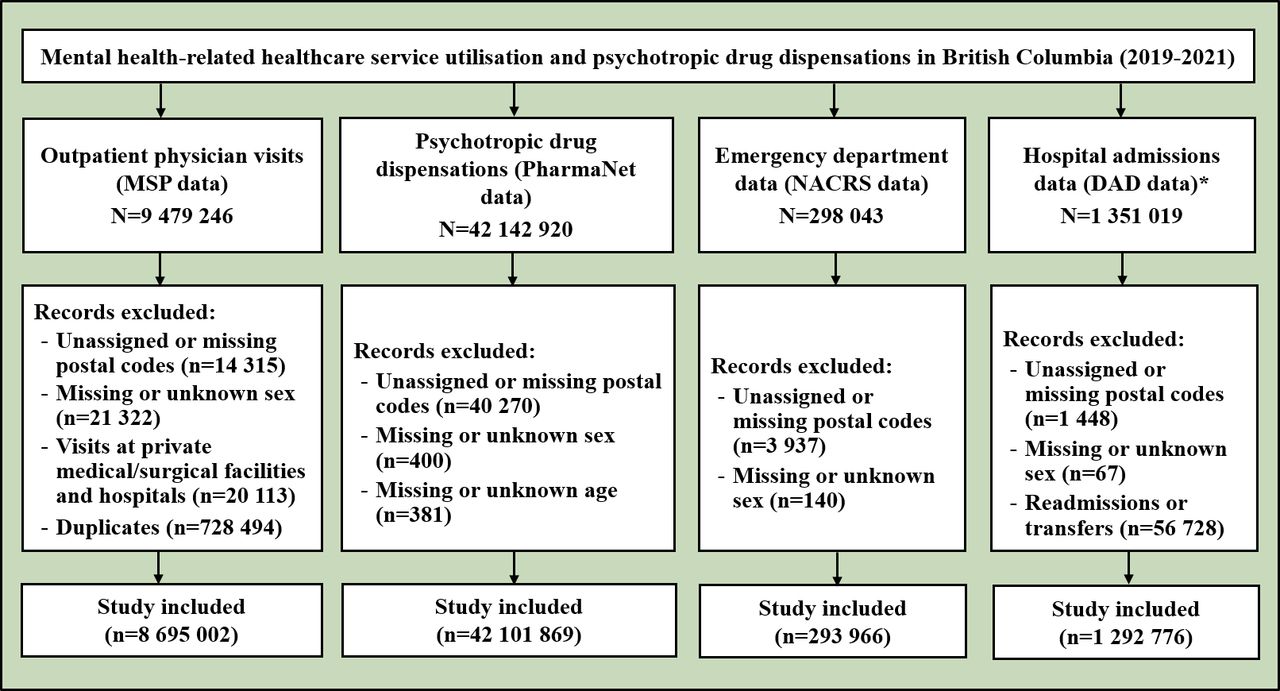
Flowchart for the selection of study population for mental health and psychotropic drug dispensations. *Hospital admission rates do no include December 2021 data. DAD, Discharge Abstracts Database; MSP, Medical Services Plan; NACRS, National Ambulatory Care Reporting System.

Age-standardised monthly average rates (per 1 000 or 100 000 population) for mental health-related healthcare service utilisation and psychotropic drug dispensations, by year (2019–2021), both sexes in British Columbia (BC). Quadrants A and B: emergency department visits and hospital admission rates expressed per 100 000 population. Quadrants C and D: outpatient physician visits and psychotropic drug dispensation rates expressed per 1 000 population.

Per cent change in monthly average age-standardised rates for mental health-related healthcare service utilisation and psychotropic drug dispensations, 2020 and 2021 vs 2019, both sexes in BC. The per cent change in the monthly average rate of mental health-related healthcare service utilisation was determined by deriving the monthly per cent change in 2020 and 2021 (pandemic periods) compared with 2019 (prepandemic period).
Online supplemental tables S5–S8 and online supplemental figures S1–S4 present the average monthly counts, rates and RRs for mental health-related ED visits, HAs, OP visits and psychotropic drug dispensations between 2019 and 2021, stratified by sex and age. Between 2019 and 2021, the overall average monthly rate for mental health-related OP visits, ED visits and psychotropic drug dispensations increased significantly by 24% (95% CI: 23% to 25%), 5% (95% CI: 2% to 9%) and 8% (95% CI: 7% to 9%), respectively. There were no significant increases in the average monthly rate of mental health-related HAs.
Sex and age differences
Comparing 2021 with 2019, mental health-related OP visits and psychotropic dispensations were significantly higher among females than their male counterparts (online supplemental tables S5 and S8). Figure 4 presents age-specific average monthly RRs in 2019 compared with 2021. Statistically significant increases in ED visit rates were observed among 10–14 and 15–19 year-olds at 30% (95% CI: 10% to 53%) and 14% (95% CI: 3% to 27%), respectively. Concurrently, HAs among 10–14 year-olds increased by 55% (95% CI: 11% to 117%). For OP visits, rates increased for every age group . Notably, there was a 44% (95% CI: 38% to 50%) and 45% (95% CI: 40% to 50%) increase in OP visits among 10–14 and 15–19 year-olds, respectively. For psychotropic drug dispensations, rate increases were also highest among youth, increasing by 35% (95% CI: 30% to 41%) for 10–14 year-olds and 34% (95% CI: 30% to 37%) for 15–19 year-olds.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Monthly average age-specific rate ratios for mental health-related healthcare service utilisation and psychotropic drug dispensations in British Columbia (BC) (2021 vs 2019). The rate ratios in the annual average rate of mental health-related healthcare service utilisation, by age group, were derived by calculating the annual per cent change in age-specific rates for January to December 2021 (pandemic period) compared with January to December 2019 (prepandemic period). Quadrant B: hospital admission data for December 2021 were not included. Quadrants A, C and D represent the emergency department visits, outpatient physician visits and psychotropic dispensation data, respectively; age-specific rates for January to December 2021 (pandemic period) were compared with January to December 2019 (prepandemic period).
Condition-specific differences
Online supplemental figures S5–S8 illustrate the relative change in the monthly average rates of mental health-related healthcare service utilisation and psychotropic drug dispensations from 2019 to 2021 stratified by sex, age and condition. For context, absolute rates are also provided in online supplemental figures S9–S12. Adolescent females aged 10–14 years had the highest relative increases, increasing 72% (95% CI: 62% to 85%) in OP visits, 56% (95% CI: 29% to 91%) in ED visits, 76% (95% CI: 20% to 161%) in HAs and 54% (95% CI: 46% to 64%) in psychotropic drug dispensations. Changes were less consistent for males aged 10–14 years than for females in the same age group, increasing 29% (95% CI: 23% to 36%) in OP visits, 12% (95% CI: −34% to 18%) in ED visits, 7% (95% CI: −45% to 110%) in HAs and 20% (95% CI: 13% to 27%) in psychotropic drug dispensations.
OP visits for depressive or anxiety disorder increased for both sexes across most age groups, with the most significant increase among females 10–19 years of age (see online supplemental figure S5). This finding is particularly notable because teenage females have the highest age-specific absolute rates (see online supplemental figure S9). Substantial relative increases were also seen in attention deficit hyperactivity disorder (ADHD)-related OP visits, with large relative increases across multiple age groups, particularly among adults (see online supplemental figure S5). Absolute rates should be considered, and relative changes in ADHD-related visits should be interpreted cautiously. Additionally, in 2021, OP visits for eating disorders among females 10–19 years of age almost doubled from 2019.
Comparing psychotropic drug dispensations in 2019 and 2021, the highest relative increase occurred among females aged 10–19 years (42%–60%) (see online supplemental figure S6). Less pronounced increases were seen among adolescent males (≤30%). There was a notable reduction in dispensations of sedatives across most age groups and both sexes. The highest relative increase in the rate of dispensations among females aged 10–14 years was for antidepressants (60%), while among females aged 15–19 years, it was for antipsychotics (47%). Less prominent relative increases in psychotropic drug dispensations were seen for males aged 10–39. Notably, youth still have some of the lowest age-specific absolute rates of psychotropic drug dispensations (see online supplemental figure S10).
Relative increases in ED visits for various mental health-related presenting complaints, including anxiety or situational crisis, depression, and suicidal or deliberate self-harm (see online supplemental figure S7), were highest among females aged 10–19. In addition, there was a notable reduction in ED visits among adults over 90, particularly men. As for HAs, relative increases were greatest for female adolescents, particularly those aged 10–14 years (see online supplemental figure S8).
Discussion
Main findings
Rates of acute mental health-related healthcare utilisation declined by about one-fifth in April 2020, immediately following the COVID-19 pandemic declaration in March 2020, and the implementation of broad public health pandemic control measures such as stay-at-home orders. However, no apparent concurrent drop was found for community-based mental health-related OP visits and psychotropic drug dispensations; instead, we observed a gradual and sustained increase from the summer of 2020 until the end of 2021. Between 2019 and 2021, there we significant increases in mental health-related OP and ED visits, and psychotropic drug dispensations. Across all four data sets, the relative increase in mental health-related healthcare service utilisation between 2019 and 2021 was highest among adolescents, particularly females. We identified sharp increases in visits and medications for depressive or anxiety disorders, along with increases in physician visits for eating disorders among youth and ADHD among adults under 50.
We found that during the COVID-19 pandemic, mental health-related healthcare service utilisation and psychotropic drug dispensations increased in BC, particularly among populations already experiencing a disproportionate burden of mental health conditions, such as adolescents.26 Our observations are consistent with previously published literature on the impact of the COVID-19 pandemic on mental health. Our study used administrative data sources, but our findings mirror the results of local population-based surveys. In the SPEAK survey, for instance, while 46% of all British Columbians reported worsening mental health conditions, 54% of 18–29 year-olds reported this deterioration.1 Mental health declines were also reported elsewhere among adolescents and young adult females in Canada. Between October 2020 and June 2021, the Canadian Institute for Health Information reported a 10% and 12% increase in self-harm-related ED visits and hospitalisations, respectively, among females 10–24 years old.27 A population-based study of children and adolescents in Ontario, Canada, reported a 10%–15% increase in the expected rate of mental health-related OP visits between July 2020 and February 2021.16 Similar to our results, their findings reported the greatest increase in visit rates (26%; 95% CI: 25% to 28%) among adolescent females.16 In Denmark, comparing prepandemic and postpandemic periods, Rømer et al28 reported an 11% (95% CI: 7% to 15%) increase in the rate of psychiatric admissions among those less than 18 years of age.28 Based on multicentre data in Ireland, McDonnell et al reported significant increases in HAs among female youth for anxiety (30%), anorexia nervosa (48%) and eating disorders (43%).29
It is important to interpret our findings in the context of the increasing incidence and prevalence of mental health-related disorders over the last decade. In BC, the overall incidence of mood and anxiety disorders increased by approximately 6% between 2010 and 2019.30 Within that period, females 1–19 years of age had the highest relative increase in the incidence of mood and anxiety disorders, followed by their male counterparts (83% vs 55% increase).30 Data from our study suggest that the COVID-19 pandemic likely exacerbated already worsening mental health, specifically among youth and adolescents, and particularly among young females.
Potential contributors to worsening mental health during the pandemic include anxiety about the unknown, changing information and guidance, reduced social connectedness, increased childcare burden and loss of employment. Another contributing factor could be the lack of or limited access to early intervention for mental health concerns prior to the COVID-19 pandemic, which worsened during the pandemic. In 2018, 18% (5.3 million) of Canadians reported a partial or entirely unmet need for mental health and addiction-related services in the previous year.31 Documented barriers to accessing mental health and addiction services in Canada include, but are not limited to, costs of services not being covered by public and private insurance plans, lack of knowledge about points of access, long wait times, particularly among children and youth, and shortage of mental health professionals.32 Youth and young adults may be more vulnerable to gaps in the healthcare system as they move from child and adolescent mental health services to adult services.
Limitations
Our study includes some limitations. First, our case definition for mental health is limited to broad diagnostic groupings used for billing purposes and may include some misdiagnoses, especially among children and youth. Standard coding may be applied differently to younger age groups; however, while the standard of coding may vary, diagnoses can provide an indication of the overall healthcare burden related to mental health-related outcomes, and within-age group changes would still be valid. Second, the ED data relied on presenting complaint codes, not discharge diagnosis based on ICD codes, because the presenting complaint information is available for almost the entire province. In contrast, discharge diagnosis data are primarily limited to large urban areas. However, despite these coding limitations, our study focused mainly on trends and signals, which are informative. Finally, our analyses did not capture substance use-related disorders, which should be investigated in the future.
Our analysis was strengthened by using four different administrative health data sources covering the entire BC population. The combined data sets collectively provided a comprehensive picture of changes in mental health-related healthcare service utilisation during the first 2 years of the pandemic across different healthcare service access points. By using administrative data sources, our study sheds light on mental health-related outcomes among youth and adolescents, a population often under-represented in population surveys. Furthermore, to our knowledge, published estimates of mental health-related healthcare service utilisation for the entire calendar year of 2021 are limited. However, these estimates are significant as the mental health consequences of the pandemic are likely to be cumulative.
Implications
Our results highlight the need for targeted mental health-related recovery efforts, whether due to a widespread pandemic or other national crises, focusing on subpopulations that experience disproportionate impacts, particularly female adolescents. These efforts should address pre-existing barriers to access to mental health and addiction services.
Data availability statement
No data are available. The DAD and COVID-19 databases were made available through British Columbia COVID-19 Cohort (BCC19C), a public health surveillance platform integrating COVID-19 data sets (testing, cases, hospitalisations, vaccinations) with administrative data holdings for the BC population (eg, medical visits, hospitalisations, emergency room visits, prescription drugs, chronic conditions, vital statistics). We are not permitted to share these data. BCC19C data are only available to researchers who request and meet the criteria for access.
Ethics statements
Patient consent for publication
Ethics approval
Our analyses were conducted under BCCDC’s mandate to perform population health surveillance and fall under the Behavioural Research Ethics Board at the University of British Columbia (approval number: H20-02097).
Acknowledgments
We acknowledge the assistance of the Provincial Health Services Authority, BC Ministry of Health and Regional Health Authority staff involved in data access, procurement and management. We gratefully acknowledge the residents of British Columbia whose data were integrated in the British Columbia COVID-19 Cohort (BCC19C). We also acknowledge the assistance of the Pharmaceutical Services Division at BC’s Ministry of Health with PharmaNet psychotropic prescription data.
References
Moe Zandy has been an epidemiologist in the public health field for approximately five years. In 2017, he graduated with a Master of Public Health in Epidemiology from the Dalla Lana School of Public Health at the University of Toronto in Canada. As an epidemiologist at British Columbia’s (BC) Observatory for Population and Public Health, a department within the Centre for Disease Control, Moe Zandy has led the mental health portfolio since 2020. Most of his work focuses on the unintended consequences of COVID-19 in BC, Canada, including the effects on mental health. He has utilised data from various administrative health sources to characterise the changes in the mental health-related healthcare service utilisation pattern.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MZ and KS were involved in the conception and design of the study. MZ and SEK accessed and verified the data. MZ was in charge of the study analysis. MZ wrote the first draft. All authors were involved in the interpretation, critically reviewed one or multiple drafts of the manuscript and approved the final version. MZ and KS are the guarantors.
Funding The BCC19C was established and maintained through operational support from Data Analytics, Reporting and Evaluation (DARE), and BC Centre for Disease Control (BCCDC) at the Provincial Health Services Authority (PHSA).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.