Article Text

Abstract
Background Depression, one of the most frequent complications after stroke, increases the disease’s burden and physical disability. Poststroke depression (PSD) is a multifactorial disease with genetic, environmental and biological factors involved in its occurrence. Genetic studies on PSD to date have mainly focused on the monoamine system and brain-derived neurotrophic factors. However, understanding is still limited about the influence of the single nucleotide polymorphism (SNP) of other neurotrophic factors on PSD.
Aims The present study aimed to investigate the relationship between seven vascular endothelial growth factor (VEGF) family gene variants that occur with PSD.
Methods A multicentre candidate gene study from five hospitals in Jiangsu Province from June 2013 to December 2014 involved 121 patients with PSD and 131 patients with non-PSD. Demographic characteristics and neuropsychological assessments were collected. The χ2 test was used to evaluate categorical variables, while the independent t-test was applied to continuous variables. SNPs in seven genes (VEGFA, VEGFB, KDR, FLT-1, IGF-1, IGF-1R and PlGF) were genotyped. Single-marker association for PSD was analysed by χ2 tests and logistic regression using SPSS and PLINK software.
Results Patients with PSD included more women and those with lower education levels, lower body mass indexes, lower Mini-Mental State Examination scores, and higher scores on the 17-item Hamilton Depression Rating Scale than non-PSD patients. Ninety-two SNPs with seven genes were genotyped and passed quality control. The rs7692791 CC genotypes, the C allele of KDR and the rs9282715 T allele of IGF-1R increased the risk for PSD (χ2=7.881, p=0.019; χ2=4.259, p=0.039; χ2=4.222, p=0.040, respectively). In addition, the SNP rs7692791 of KDR was significantly associated with PSD by the logistic regression of an additive model (p=0.015, OR=9.584, 95% CI: 1.549 to 59.31).
Conclusions Patients with rs7692791 C allele carriers or the CC genotype of KDR and the rs9282715 T allele of IGF-1R may have PSD susceptibility. Findings such as these may help clinicians to identify the high-risk population for PSD earlier and, thus, enable them to provide more timely interventions.
Trial registration number ChiCTR-OCH-13003133.
- Depression
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Genetic studies on poststroke depression (PSD) have mainly focused on the monoamine system and brain-derived neurotrophic factors. However, the influence of the single nucleotide polymorphism of other neurotrophic factors on PSD remains unclear.
WHAT THIS STUDY ADDS
The present study suggests that PSD is more common among women and individuals with lower education levels, lower body mass indexes and lower Mini-Mental State Examination scores. In addition, patients with KDR C allele carriers or the CC genotype have a higher risk for PSD.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Findings such as these may help clinicians to identify the high-risk population for PSD earlier and, thus, enable them to provide more timely interventions.
Introduction
Depression is one of the most frequent complications after a stroke. Previous studies found that the cumulative incidence rate of poststroke depression (PSD) is higher than 30% within the first year after a stroke.1 It increases the disease’s burden, physical disability and, more seriously, mortality, thus, posing significant challenges to psychiatrists and neurologists.2 Although many scholars have researched the pathogenesis of PSD in biology, psychology and sociology, the aetiological mechanisms remain uncertain.3 The relatively high heritability of stroke and depression—approximately 37%—would indicate that genetic factors play a pivotal role in the pathogenesis of PSD.4 5
Previous studies focused on the relationship between PSD and the monoamine system gene polymorphisms, including the serotonin transporter–linked promoter region (5-HTTLPR), variable number of tandem repeats of serotonin transporter gene intron 2,6 serotonin receptor-α7 and catechol-O-methyltransferase.8 Furthermore, a meta-analysis including four studies found that the SS genotype of 5-HTTLPR may be a risk factor for PSD.9 In addition to the monoamine hypothesis, the neurotrophic factor hypothesis also suggests a means for understanding depression and PSD; the brain-derived neurotrophic factor (BDNF) is the core molecule of this hypothesis. The polymorphism rs6265 of BDNF (Val66Met) and two single nucleotide polymorphisms (SNPs) (rs1778929, rs1187323) of its receptor-neurotrophic tyrosine kinase receptor B have been associated with PSD.10 Moreover, gene–gene interactions with the P11 (S100A10)–tissue plasminogen activator–BDNF pathways also play a central role in regulating the underlying mechanism of PSD in Chinese samples.11 However, another meta-analysis recruiting 272 cases and 503 controls from five studies found no relationship between the BDNF Val66Met polymorphism and the risk of PSD.12 In addition, other factors such as the cytokine gene,13 N5, N10-methylenetetrahydrofolate reductase,14 oestrogen receptor,15 the cyclic AMP response element-binding protein and the membrane transporting organic anion polypeptide 1C1 were associated with PSD.16
Although genetic studies of PSD have yielded some evidence, each of these identified genes or loci has been supported by limited research and only explains a small proportion of the genetic variation in PSD. Therefore, common single-site or single-gene genetic variations might offer a different means for exploring the vulnerability for or resilience to developing complicated psychiatric illnesses. Recent high-throughput sequencing technological advances provide an opportunity to sequence multiple genetic regions and better explain the mechanisms of complex polygenic disease. Zhao and her colleagues17 conducted a two-stage candidate gene study by targeted sequencing. They identified two novel genes, 5-hydroxytryptamine receptor 3D (HTR3D, rs55674402) and neurogenin3 (rs144643855), associated with PSD. They also identified three risk SNPs (rs17406271, rs2271419, rs2271420) in one risk gene β-isoform in the class II phosphoinositide 3-kinase associated with non-PSD in Chinese populations. HTR3D and neurogenin3 were involved in serotonergic synapse function, central nervous system development and neural plasticity in the hippocampus. These findings support the hypotheses that monoamine neurotransmitters and neurotrophic factors are important aetiological mechanisms of PSD.
According to the neurotrophic factor hypothesis, a group of trophic and growth factors also contribute to protecting the nervous system and alleviating psychological stresses: BDNF, vascular endothelial growth factor (VEGF), vascular endothelial growth factor receptor (VEGFR), insulin-like growth factor 1 (IGF-1), insulin-like growth factor receptor 1 (IGF-1R) and placental growth factor (PlGF). VEGFR1 and VEGFR2 were the main VEGFs’ signalling activity, also known as Fms-like-tyrosine kinase (FLT-1) and kinase insert domain-containing receptor (KDR). Multifunctional trophic factors, such as VEGF and IGF, possessing both neurotrophic and angiogenic actions, are significant due to their ability to restore plasticity and repair structural deficits in vasculature and neurons.18 Expanding insight regarding the gene polymorphism and molecular actions of multifunctional trophic factors can expedite further understanding of PSD. Moreover, our previous study demonstrated that the levels of VEGFR2 and PlGF proteins in the PSD group were significantly different from the control group.19 However, the SNP of these neurotrophic factors in the pathogenesis of PSD remains unclear. Therefore, the present study aimed to investigate the relationship between seven VEGF family gene variants of neurotrophic factors, including vascular endothelial growth factor A (VEGFA), vascular endothelial growth factor B (VEGFB), KDR, FLT-1, IGF-1, IGF-1R and PlGF, with the occurrence of PSD.
Methods
Study design and study samples
This is a part of a multicentre study, ‘The standardisation strategy of diagnosis and treatment of post-stroke depression’. The present candidate gene study recruited 260 inpatients with ischaemic stroke from five hospitals (ZhongDa Hospital, affiliated with Southeast University; The Affiliated First Hospital of Soochow University; The Affiliated Hospital of Xuzhou Medical University; The Third People’s Hospital of Huai'an and Jiangsu Province Hospital) in Jiangsu Province, China, from June 2013 to December 2014. We conducted consistency training before the research. All recruited patients were screened and interviewed by qualified psychiatrists who received training to ensure standard PSD diagnosis. The patients were screened for depression in structured interviews with psychiatrists according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Ultimately, 121 patients with PSD and 131 non-PSD patients participated in our study. All subjects were ethnically Han Chinese and gave written informed consent at recruitment. The stroke diagnosis for patients was verified by computed tomography (CT) or magnetic resonance imaging (MRI) reports, along with some persistent poststroke somatic impairments. The eligibility criteria for patients with PSD were as follows: (1) willingness to participate in the study, (2) history of stroke or stroke sequela as determined by CT or MRI, followed by depressive symptoms, (3) fulfilled PSD diagnostic criteria proposed by Yuan et al 20 who put forward the idea that general PSD should include PSD symptom disorder and PSD disorder according to ZhongDa Diagnostic Criteria, First Edition (ZD-1) (see box 1) and also fulfilled the DSM-5 criteria for depression; (4) aged 35–85 years; (5) no other major psychiatric disorders or psychiatric history. The eligibility criteria for patients with non-PSD were as follows: (1) willingness to participate in the study, (2) history of ischaemic stroke as determined by CT or MRI, (3) aged 35–85 years, (4) did not fulfil PSD diagnostic criteria and (5) no other major psychiatric disorders or psychiatric history (figure 1).
PSDSD diagnostic criteria from ZhongDa (First Edition)
Three (or more) of the following symptoms have been present during the same 1-week period and represent a change from previous functioning:
Decreased speech (eg, does not want to speak) most of the day, daily or most of the week.
Fatigue or loss of energy daily or most of the week.
Depressed mood persisting through the day, daily or most of the week, as indicated by either self-report or observation made by others (eg, feels sad, easily cries).
Insomnia, waking up early or hypersomnia daily or most of the week.
Feelings of decreased capability and worthlessness most of the day, daily or most of the week.
Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, a suicide attempt or a specific suicide plan.
Feeling of hopelessness or despair (especially feeling recovery from the disease is difficult) most of the day, daily or most of the week.
More irritable than usual, daily or most of the week.
The symptoms cause clinically significant distress or impairment in social interaction, occupation or other important areas of functioning.
The occurrence, development and duration of these symptoms are closely related to cerebrovascular disease.
The occurrence of the major depressive episode could not be better explained by adjustment disorder with depressed mood, schizoaffective disorder, schizophrenia, schizophreniform disorder, delusional disorder or other specified and unspecified schizophrenia spectrum and other psychotic disorders.
No manic or hypomanic episode is reported.
PSDSD, poststroke depression symptom disorder.
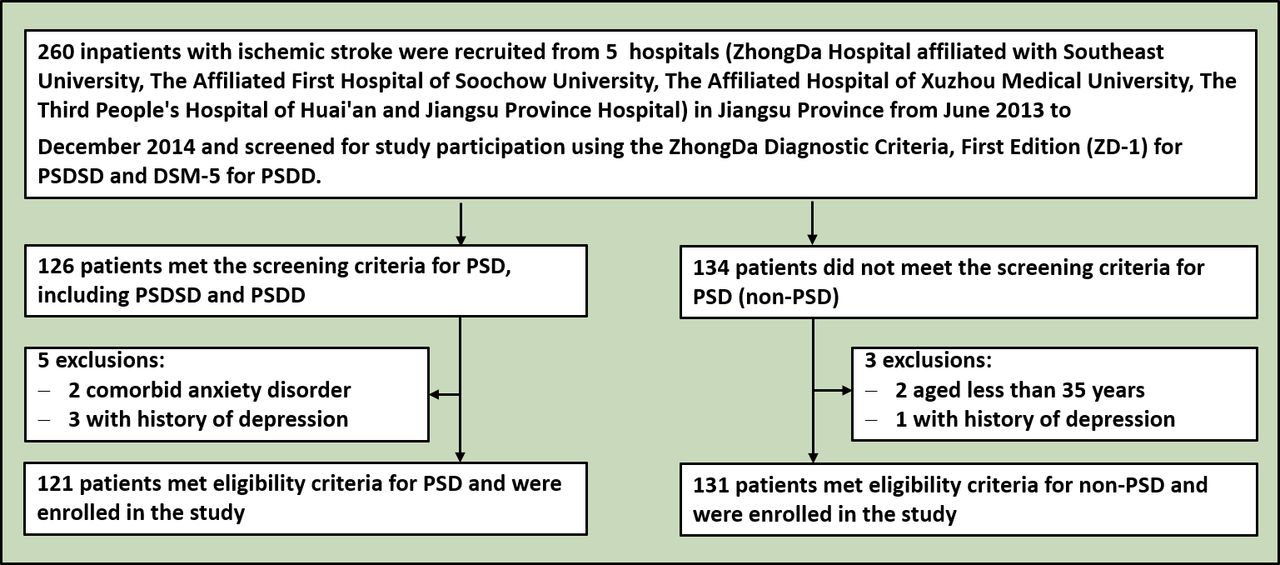
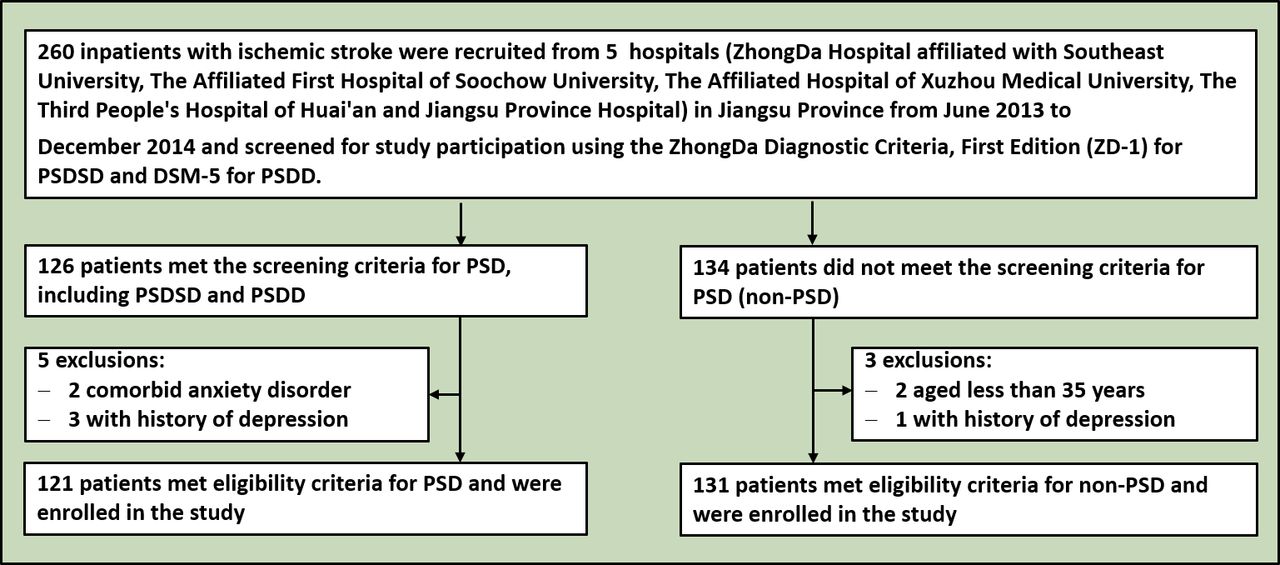{kind=link}
Flowchart of study enrolment. PSD, poststroke depression; PSDSD, PSD symptom disorder; PSDD, PSD disorder.
Demographic characteristics and neuropsychological assessment
Data regarding age, gender, educational level, body mass index (BMI) and vascular risk factors—including hypertension, coronary heart disease, diabetes mellitus, hypercholesterolaemia, active smoking and alcohol consumption—were collected from all participants. Depression severity and cognitive function were evaluated by the 17-item Hamilton Depression Rating scale (HDRS) and the Mini-Mental State Examination (MMSE). The neurological function was assessed by the National Institutes of Health Stroke Scale (NIHSS), the modified Rankin Scale (mRS) and the Barthel Index (BI).
Blood collection
Venous blood samples were drawn from the antecubital veins to ethylenediamine tetraacetic acid (EDTA)-anticoagulant tubes of all participants. Blood samples captured in anticoagulant were isolated and stored at −80°C until examined.
Gene array and genotyping
The sequencing was conducted by Illumina HiSeq2500 (Illumina, San Diego, California, USA). Then the variants calling and genotyping and the clustering of study sample genotypes were performed using Illumina’s GenTrain (V.1.0) clustering algorithm in Genome Studio (V.2011.1). The following factors were referred to when screening genes and polymorphic loci: (1) meaningful genes or SNPs identified in previous candidate gene association studies or genome-wide association studies and (2) the pathophysiological mechanisms involved in the development of depression or PSD. Finally, 92 polymorphic loci of seven genes related to neurotrophic and vascular regeneration were sequenced. Association analysis was restricted to SNPs via a sequencing strategy.
Quality controls
Gene polymorphisms were excluded for further measurement if they met the following criteria: (1) call rate <90% or a read depth <10×, (2) minor allele frequency (MAF) <0.05 and (3) significant deviation from Hardy-Weinberg equilibrium (HWE) in the controls (p<0.05).
Statistical analyses
The demographic characteristics and psychological assessment between the two groups were analysed by independent t-tests for continuous variables and Pearson’s χ2 tests for categorical variables using SPSS 26.0 (SSPS, Chicago, Illinois, USA), PLINK 2.0 (https://www.cog-genomics.org/plink/2.0/) and Haploview 4.1 (https://sourceforge.net/projects/haploview). Single-marker association analyses were performed to test for PSD associated with SNP by logistic regression of an additive model and a dominant model. A p value of 0.05 was set as the significant level.
Results
Demographic characteristics and psychological assessment of participants
Looking at demographic characteristics, gender (χ2=5.841, p=0.016), education level (t=3.391, p=0.001), BMI (t=2.650, p=0.009), MMSE score (t=1.993, p=0.047), hypertension rate (χ2=3.976, p=0.046) and HDRS score (t=−24.555, p<0.001) all had statistically significant differences. The patient group with PSD included more women and overall had lower education levels, BMI, MMSE scores and hypertension rates but higher HDRS scores than patients with non-PSD. There were no significant differences in age, neurological function (NIHSS, mRS and BI scores) or vascular risk factors, except hypertension between the two groups (all p>0.05; see table 1).
Clinical and demographic characteristics between patients with PSD and those with non-PSD
Gene characteristics of SNPs in VEGFA, VEGFB, KDR, FLT-1, IGF, IGF-1R and PlGF genes
Table 2 illustrates the quality control process. Ultimately, 92 SNPs of seven genes were detected and passed quality control. All of the SNPs were in HWE (p>0.05 in all subjects), and all MAF levels were more than 0.05. The gene information and the results of the linkage disequilibrium analyses of SNPs within each gene are listed in the online supplemental material.
Supplemental material
Quality control process of the genes
Genotypes and allele distributions of the VEGF family genes by χ2 tests
The SNP rs7692791 of the KDR gene showed a significant difference in patients with PSD compared with patients with non-PSD (χ2=7.881, p=0.019) (see table 3). The CC genotypes of the rs7692791 polymorphism were the risk factors for PSD. The allele frequencies of the KDR gene (rs7692791) and the IGF-1R gene (rs9282715) were significantly different between patients with PSD and those with non-PSD (χ2=4.259, p=0.039; χ2=4.222, p=0.040, respectively) (see table 3). The C allele of the rs7692791 polymorphism and the T allele of the rs9282715 polymorphism increase the risk of PSD. However, we did not find any differences in genotypes and allele distributions in VEGFA, VEGFB, FLT-1, IGF-1 and PlGF genes.
χ2 tests of genotype and allele frequencies for the VEGF gene family
Relationship between PSD and SNP of VEGF family genes by logistic analysis
The SNP rs7692791 of the KDR gene was significantly associated with PSD by the logistic regression of an additive model with the covariants of gender, education level and BMI (p=0.015, OR=9.584, 95% CI: 1.549 to 59.31). Two SNPs of the KDR gene and four SNPs of the IGF-1R gene were significantly associated with PSD by a corrected logistic regression of the dominant model (all p<0.05) (see table 4). However, we did not find any significant relationship between PSD and VEGFA, VEGFB, FLT-1, IGF-1 and PlGF genes.
Association results of VEGF family genes through logistic regression
Discussion
Main findings
In the present study, the KDR CC genotypes, the C allele of rs7692791 polymorphism and the IGF-1R T allele of rs9282715 polymorphism were the risk factors for PSD. The SNP rs7692791 of the KDR gene was significantly associated with PSD by the logistic regression of an additive model.
VEGFRs, receptors of VEGF, were cell surface receptor tyrosine kinases. VEGF signalling activity depends on its three known specific membrane receptors: VEGFR1, VEGFR2 and VEGRF3. VEGFR2 is one primary member of the VEGFR family, expressed on vascular and lymphatic endothelial cells and is encoded by the KDR gene.21 A previous study showed that five SNPs (rs7692791, rs2305948, rs13109660, rs6838752, rs2034965) in the VEGFR2 gene were associated with clinical outcomes, and particularly the rs7692791 TT genotype was related to both reduced overall survival and disease-free survival (DFS) of hepatocellular carcinoma.22 However, the TT genotype of rs7692791 was positively associated with longer DFS in patients with advanced gastric cancer.23 Another study also found that the distribution of the KDR polymorphisms rs18770377 and rs7667298 differs significantly in patients with a recurrent depressive disorder compared with healthy subjects.24 They illustrated that the +271 G/A polymorphism is related to mRNA expression, as the AA genotype is associated with a higher VEGFR2 mRNA level. VEGF or VEGF-Flk-1 signalling is also required for antidepressant-induced cell proliferation and sufficient for behavioural responses in chronic and subchronic antidepressant models.25 A study of patients with schizophrenia demonstrated that VEGFR2 was significantly lower in C carriers than in TT genotypes of rs7692791 in the prefrontal cortex and was inversely correlated with the positive symptom subscale of the Diagnostic Instrument for Brain Studies, showing that VEGF is potentially related to schizophrenia.26 It is consistent with our study that high frequency of C allele or CC genotypes of the rs7692791 polymorphism and decreased protein of VEGFR2 participate in the occurrence of PSD.19
IGF-1R, characterised by a heterodimer of α- and β-chains, is a transmembrane tyrosine kinase receptor activated by its ligand IGF. IGF is a neurotrophic factor that the immune system may regulate; activation of IGF-1R is associated with improved growth, proliferation, angiogenesis, tissue remodelling and neuroprotection.27 The study of IGF-1R polymorphisms found that the rs3743251 A/A genotype was negatively associated with hepatitis B virus–related hepatocellular carcinoma and the A/G genotype decreased the risk of portal vein thrombosis.28 In addition, the rs1815009 inside 3′ untranslated regions (UTR) of IGF-1R presented significant genotype distribution in patients with prostate cancer and hypertension.29 Five SNPs discovered in this study were all inside 3′ UTR and have not been reported in mental disorders. According to its mechanism in other diseases, it is speculated that rs1815009 in the IGF-1R gene may participate in these disorders by regulating the level of microRNAs.30
Limitations
This research has some limitations. First, our sample was relatively small, limiting further gene–gene interaction and stratification analyses. Second, patients who had a stroke were in different stages of the disease, including acute, subacute and chronic. We should pay attention to the stages of stroke on the results in future studies. Third, sample variables, including gender, educational level and BMI, were not matched for the two groups. Thus, gender, educational level and BMI were adjusted as covariates by logistic analysis to reduce the impact on statistical results.
Implications
PSD is one of the most prevalent and potentially fatal stroke complications. However, at present, there are few genetic mechanisms to explore subjects at high risk for PSD. The present study suggests PSD is more prevalent among women and those with low education levels, BMIs and MMSE scores. Patients with KDR C allele carriers or the CC genotype have a high risk for PSD. Findings such as these may help clinicians to identify the population at high risk for PSD earlier and enable more timely interventions.
Conclusions
In conclusion, our findings suggest that KDR and IGF-1R genetic polymorphisms are significantly associated with PSD. The rs7692791 CC genotypes or C allele may play important modulating roles in the genetic effects of KDR on PSD susceptibility. Moreover, five SNPs of the IGF-1R gene were also associated with PSD. Therefore, the molecular and pathway mechanisms behind genetic polymorphisms can be further explored.
Data availability statement
Data are available on reasonable request.
Ethics approval
This study involves human participants and was approved by the Medical Ethics Committee for Clinical Research of Zhongda Hospital affiliated to Southeast University (2013ZDSYLL011.0). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We wish to thank all the participants and their institutions in this study.
References
Yingying Yue obtained a doctor's degree from Southeast University, China in 2017. Currently, she is an attending physician in the Department of Psychosomatics and Psychiatry, Affiliated ZhongDa Hospital of Southeast University in China. Her main research interests include the pathogenesis and efficacy mechanism of depression and the diagnosis and treatment of post-stroke depression.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YYue: Data curation, formal analysis, writing and revision of the original draft. LY, FZ, KZ, YS, HT, JL, SL, JC, DG, AW: Data curation and clinical assessments. YYua: Study design, methodology, formal analysis and quality control. YG is responsible for the overall content as guarantor.
Funding This work was supported by the National Natural Science Foundation of China-Youth Foundation Projects (grant no: 81901375) and the Natural Science Foundation of Jiangsu Province (grant no: BK20180370).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.