Article Text

Abstract
Background Patients who suffer comorbidity of major depressive disorder (MDD) and chronic pain (CP) maintain a complex interplay between maladaptive prospective memory (PM) and retrospective memory (RM) with physical pain, and their complications are still unknown.
Aims We aimed to focus on the full cognitive performance and memory complaints in patients with MDD and CP, patients with depression without CP, and control subjects, considering the possible influence of depressed affect and chronic pain severity.
Methods According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders and the criteria given by the International Association of Pain, a total of 124 participants were included in this cross-sectional cohort study. Among them, 82 depressed inpatients and outpatients from Anhui Mental Health centre were divided into two groups: a comorbidity group(patients with MDD and CP) (n=40) and a depression group (patients with depression without CP) (n=42). Meanwhile, 42 healthy controls were screened from the hospital’s physical examination centre from January 2019 to January 2022. The Hamilton Depression Rating Scale-24 (HAMD-24) and Beck Depression Inventory-II (BDI-II) were used to evaluate the severity of depression. The Pain Intensity Numerical Rating Scale (PI-NRS), Short-Form McGill Pain Questionnaire-2 Chinese version (SF-MPQ-2-CN), Montreal Cognitive Assessment-Basic Section (MoCA-BC), and Prospective and Retrospective Memory Questionnaire (PRMQ) were used to assess pain-related features and the global cognitive functioning of study participants.
Results The impairments in PM and RM differed remarkably among the three groups (F=7.221, p<0.001; F=7.408, p<0.001) and were severe in the comorbidity group. Spearman correlation analysis revealed the PM and RM were positively correlated with continuous pain and neuropathic pain (r=0.431, p<0.001; r=0.253, p=0.022 and r=0.415, p<0.001; r=0.247, p=0.025), respectively. Regression analysis indicated a significant positive relationship between affective descriptors and total BDI-II score (β=0.594, t=6.600, p<0.001). Examining the mediator pathways revealed the indirect role of PM and RM in patients with comorbid MDD and CP.
Conclusions Patients with comorbid MDD and CP presented more PM and RM impairments than patients with MDD without CP. PM and RM are possibly mediating factors that affect the aetiology of comorbid MDD and CP.
Trial registration number chiCTR2000029917.
- depressive disorder, major
- cognitive dysfunction
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Major depressive disorder (MDD) and chronic pain (CP) are highly comorbid among patients in clinical settings. Cognitive dysfunction is already known as one of the common symptoms in patients with MDD or CP, especially memory impairment, but few studies have focused on how memory impairment affects the patients’ emotions and pain experience.
WHAT THIS STUDY ADDS
We used the Prospective and Retrospective Memory Questionnaire (PRMQ) scale to evaluate prospective memory (PM) and retrospective memory (RM) in patients with MDD and CP. We comprehensively studied these areas by focusing on particular memory complaints in different samples of patients and control subjects.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings indicate that severe impairments of PM and RM may cause complex symptoms in patients with comorbid MDD and CP. However, more studies are needed to explore the long-term effects of the impairments of memory processes and other cognitive functions in this vulnerable population.
Introduction
Major depressive disorder (MDD) and chronic pain (CP) are well-documented comorbid conditions with a 30%–50% incidence rate.1 Generally, overlapping biological mechanisms between the two often coexist and exacerbate each other. Moreover, comorbidity reduces compliance to treatment2 and increases the risk of relapse after treatment.3 Long-term studies in clinical settings have shown that patients with MDD or CP have extensive cognitive impairments.4 High levels of pain perception seem to be associated with cognitive deficits in patients with depression.5 Furthermore, patients may experience persistent and severe cognitive impairments and fail to return to baseline functioning even after MDD symptoms are alleviated.6 Hence, systematic research is needed to explore the relationships between cognitive variables potentially mediating the association between depression and pain. Memory impairment is one of the most common cognitive dysfunctions. When memory-related deficits occur with comorbid conditions, the degree of impairment can significantly impact the quality of life, occupational and social role fulfilment, and even daily activities. Among individuals with primary psychotic illness, poor prospective memory (PM) and retrospective memory (RM) are related to impaired community living skills, financial management and medication management, suggesting that PM and RM are critical determinants of independent life.
PM is a type of memory that involves the ability to formulate intentions, make plans and promises, retain them, recollect and carry them out at appropriate times or contexts (eg, remembering to carry out an action). By contrast, RM can be defined as the ability to remember past information (eg, remembering past actions or events).7 In comparison to healthy people, individuals with schizophrenia have deficits that prevent them from performing PM and RM memory tasks and generally lack awareness of these deficits. Neither medication effects nor the duration of illness is linked to these deficits.8 Several depression-relevant impairments related to PM and RM have been reported.9 One study found that depression was negatively correlated with PM task performance in 40 first-year psychology students,10 and the memory of time and events in PM were substantially affected by depression. Especially, impaired time memory of PM in depression required self-initiation without specific external cues to elicit intention.11 This finding suggests that motivational instructions impact the controlled processes underlying PM. This relationship may be one of the critical factors affecting the severity of clinical symptoms. A considerable number of studies have shown that pain exerts a deleterious effect on cognitive functioning,12 and pain intensity and pain duration are positively correlated with RM impairment in patients suffering from chronic pain.13 14 Despite the growing interest in these issues, relatively few studies on PM and RM have focused on comorbid MDD and CP.
The performance of memory tasks was determined by the type of internal processing operation required by the task, and individuals with persistent pain or depression have limited memory resources to engage in complex processing tasks; thus, memory biases have been documented in those patients.15 To further investigate the relationship between different memory tasks and the comorbidity of depression and chronic pain, the purpose of the present study was to test whether PM and RM would mediate the association between depression, pain severity and the interference pain causes in their lives. Hence, we hypothesised that individuals with comorbid chronic pain and depression will have impaired PM and RM associated with depressive mood, pain severity and pain interference. In summary, we aimed to focus on complete cognitive performance and memory complaints in patients with MDD and CP, patients with depression without CP, and control subjects, considering the possible influence of depressed clinical symptoms and chronic pain severity.
Materials and methods
Participants
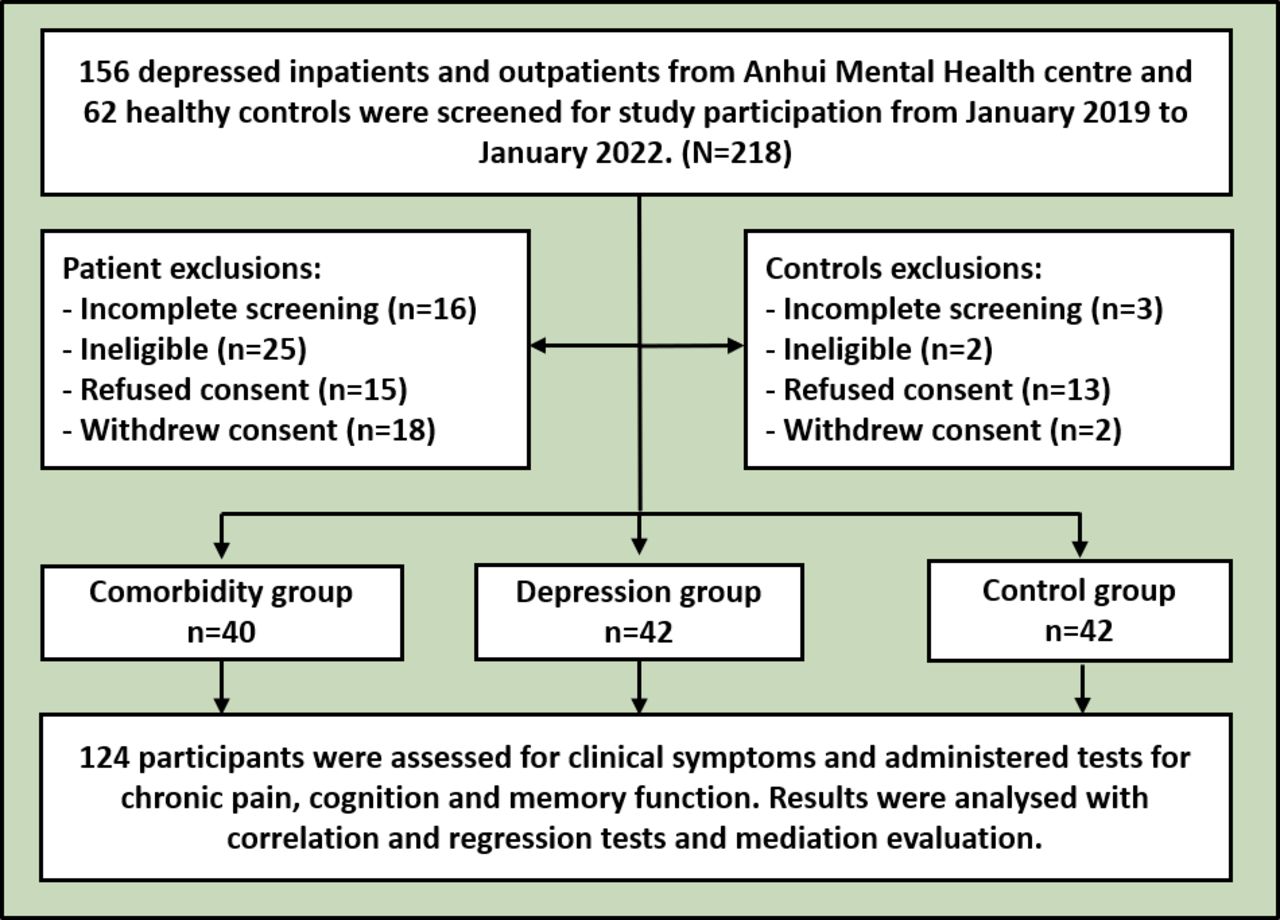
This cross-sectional cohort study was conducted at Anhui Mental Health Center (AMHC) from January 2019 to January 2022. The medical ethics committee of AMHC approved the study. In accordance with the Helsinki declaration, all participants provided written consent before participating in this study. Two professional psychiatrists used the Chinese version of the Mini International Neuropsychiatric Interview (C-MINI) 5.0.0 to evaluate participants. A total of 218 participants were initially screened: 156 depressed inpatients and outpatients were screened from AMHC and 62 healthy individuals were screened from the hospital’s physical examination centre. Among the depressed inpatients/outpatients, 16 failed to complete the assessment, 15 declined to provide written informed consent, 25 did not meet the study criteria and 18 withdrew consent. Meanwhile, among healthy controls, 3 failed to complete the assessment, 13 declined to provide written informed consent, 2 did not meet the study criteria and 2 withdrew consent. Ultimately, 124 participants were included and divided into the following groups: a comorbidity group (patients with MDD and CP, n=40), a depression group (patients with depression without CP, n=42) and a control group (healthy controls, n=42) (figure 1).
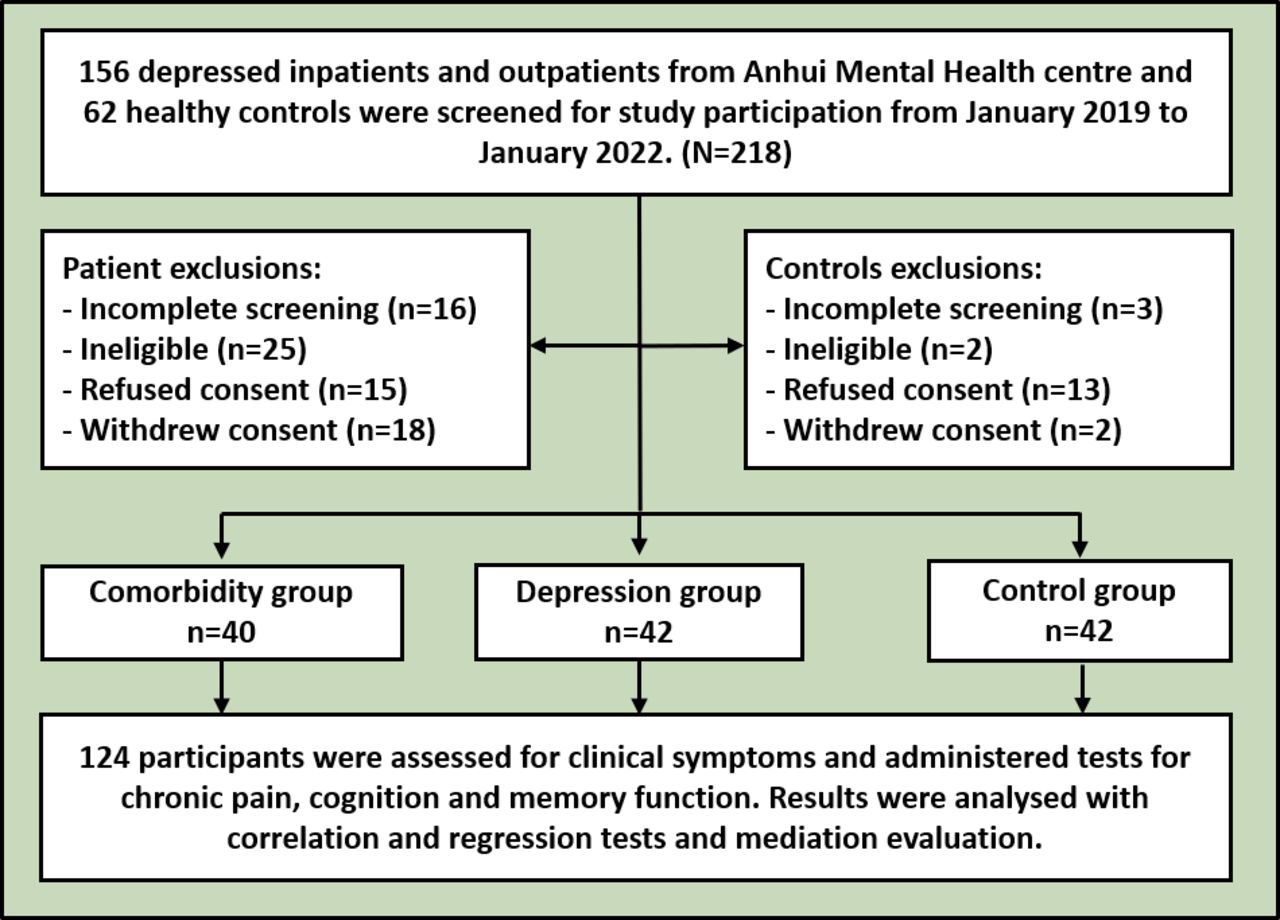
Flowchart of study enrolment.
Inclusion criteria for patients in the comorbidity group were as follows: (1) met the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria for MDD and the CP standards defined by the International Association for the Study of Pain, as assessed by two independent senior psychiatrists; (2) aged between 18 and 65 years; (3) chronic pain was not due to traumatic physical injury, serious somatic disease or inflammatory disease; (4) pain intensity numerical rating scale (PI-NRS) ≥3. The inclusion criteria for the depression group were as follows: (1) met the DSM-5 criteria for MDD as assessed by two independent senior psychiatrists; (2) aged between 18 and 65 years; (3) PI-NRS <3. The inclusion criteria for the control group were as follows: healthy people screened from the physical examination centre of AMHC. Exclusion criteria for all participants were as follows: (1) history of severe craniocerebral trauma or somatic trauma; (2) history of severe tumour-related, neurological or inflammatory diseases; (3) history of substance use or other mental disorders; (4) history of serious physical disease; (5) pregnant or lactating women; (6) administration of modified electroconvulsive therapy within three months before enrolment.
Assessment instruments
Chinese version of the Mini International Neuropsychiatric Interview (C-MINI) 5.0.0
The C-MINI demonstrates good psychometric properties16 and is valid and reliable. Inter-rater and test-retest reliabilities are excellent, with kappa values above 0.80 and 0.90, respectively. The C-MINI is the gold standard for diagnosing depressive disorders in China.
Demographic characteristics
A self-reported questionnaire was used to collect information about age, gender, educational level, family patterns, marital status, medication, income level, employment status and disease duration.
Hamilton Depression Rating Scale 24 (HAMD-24)
The HAMD-24 is the most commonly used depression scale worldwide due to its high specificity for assessing depression symptom severity.17 The HAMD-24 score may be used in defining clinically relevant symptom levels: <8=no depression, 8–19=mild depression, 20–34=moderate depression and ≥35=severe depression. The Cronbach’s alpha of HAMD-24 is 0.88, and the κ score is 0.92.18
Beck Depression Inventory (BDI)-II
The BDI-II is a 21-item self-report scale designed to investigate the severity of depression symptoms. Each item is rated from 0 to 3 according to general guidelines, and the total score ranges from 0 to 63. A high score indicates severe depressive symptoms. The BDI-II has good internal consistency (Cronbach’s alpha=0.83) and excellent criterion validity (κ=0.94) compared with other depression measures.19
Montreal Cognitive Assessment-Basic Section (MoCA-BC)
Global cognitive functioning was assessed by the Chinese version of the MoCA-BC. It is a 30-point scale that assesses nine cognitive domains: executive function, language, orientation, calculation, conceptual thinking, memory, visual perception, naming and attention. It is freely available for clinical use (www.mocatest.org, visit Basic section). The cut-off scores of the MoCA-BC were 19 in the low-level education group (≤6 years), 22 in the mid-level education group (7–12 years) and 24 in the high-level education group (>12 years).20
Prospective and Retrospective Memory Questionnaire
The Prospective and Retrospective memory questionnaire (PRMQ) is a 16-item questionnaire evaluating memory failure in everyday life. Half of the PRMQ items enquire about PM and the other half about RM. The Chinese version of the PRMQ is a valid tool for evaluating PM and RM impairments in gender and adjacent age groups.21
Pain Intensity Numerical Rating Scale (PI-NRS)
The Pain Intensity Numerical Rating Scale (PI-NRS) is an 11 point numerical rating scale that assesses pain intensity and demonstrates strong construct validity and stability, where 0 means no pain and 10 is the worst possible pain. Due to its simplicity, it is widely used clinically to evaluate chronic pain.22
Short-Form McGill Pain Questionnaire-2-Chinese version
The Short-Form McGill Pain Questionnaire-2-Chinese version (SF-MPQ-2-CN) is a self-rated scale, rating pain intensity from 0 to 10 (0=no pain and 10=the worst pain) and is composed of 22 pain descriptors and four subscales. It has excellent reliability and validity, and Cronbach’s alpha for the subscales ranges from 0.896 to 0.916. The test-retest results indicated excellent reliability, with values of 0.909, 0.973, 0.988, 0.952 and 0.927 for the continuous, intermittent, predominantly neuropathic, and affective subscales and total scale, respectively.23
Statistical analysis
SPSS V.22.0 was used for statistical analyses. Values conforming to a normal distribution were presented as mean and standard deviation (SD), otherwise, as median and interquartile spacing (IQR: 25%, 75% percentiles). Student’s t-tests, χ2 test and ANOVA were performed to compare differences in continuous or categorical parameters among the three groups. We used one-way ANOVA to evaluate the symptoms among the three groups and the Least-Significant Difference (LSD) (homogeneous variances) method for intergroup comparison. As for non-homogeneous variables, we used the Games-Howell test to estimate the intergroup comparison. We adopted Spearman correlation to assess the correlations among cognitive, memory, clinical symptoms, symptom intensity and pain perception. Stepwise regression analysis demonstrated that the independent determinants of pain-related factors were the main influential factors for patients with comorbidity. Finally, mediation analysis was performed to test further whether the relationship between pain and depressive symptoms was mediated by PM and RM. This analysis was performed by quantifying the direct and indirect relationships among the independent variable (pain), mediators (PM and RM) and dependent variables (symptoms of depression). In the mediation models, all paths were reported as unstandardised ordinary least-squares regression coefficients. Significance analysis was based on 5 000 bootstrap realisations, and a significant indirect effect was indicated when the bootstrap 95% confidence interval (CI) was not zero. All tests were two-tailed, and differences were considered statistically significant at a p value of <0.05.
Results
Demographic, depression psychometric properties and pain intensity of the comorbidity, depression and control groups
The demographic data, psychometric properties of depression and pain intensity of the three groups are shown in table 1. A total of 124 individuals were included in the final analyses. We recruited 40 patients with comorbid MDD and CP (27 males and 13 females), 42 patients with MDD but without CP (24 males and 18 females) and 42 healthy controls (18 males and 24 females). No remarkable differences in age, years of education, employment status, family patterns, marital status, income level and the number of outpatients/inpatients were found among the groups (p>0.05). The clinical properties of depression were comprehensively assessed by a self-rated BDI-II scale and a psychiatrist-evaluated HAMD scale. Scores from the two scales in the comorbidity group were significantly higher than those in the depression group, regardless of whether the depression was self-evaluated by patients or evaluated by a psychiatrist (t=2.519, p=0.014; t=2.378, p=0.020). Pain intensity was also found to be more severe in the comorbidity group than in the depression group (t=9.343; p<0.001).
Demographic characteristics, clinical symptoms and cognitive function assessments among the comorbidity, depression and control groups
Characteristics of cognition, prospective memory, retrospective memory and pain-related features in the comorbidity, depression and control groups
The MoCA-BC and PRMQ were used to evaluate the multidimensional characteristics of cognition and memory. Results for the seven factors of the MoCA-BC (visuospatial/executive functions, naming, attention, language, abstraction, delayed recall and orientation) can be seen in table 1. The delayed recall score varied among the groups (F=5.764, p=0.004), and the depression and comorbidity groups were more seriously impaired than the control group (p=0.016 and p=0.002, respectively). Meanwhile, the total MoCA-BC score differed among the three groups (F=3.486, p=0.034), and the impairment of the comorbidity group was more severe than the control group (p=0.011).
Furthermore, we used the PRMQ to evaluate memory functioning. Two components of the PRMQ (PM and RM) were evaluated, and distinguishable divergence was observed in the three groups (F=7.221, p<0.001; F=7.408, p<0.001). We also found that impairment of PM and RM in the comorbidity group was more severe than in the depression group (p=0.002 and p=0.014, respectively) and the control group (p<0.001 and p<0.001, respectively). Finally, we used the SF-MPQ-2-CN to assess pain-related features in the three groups, including continuous, intermittent, and neuropathic pain, and then examined affective descriptors. All the components of the SF-MPQ-2-CN differed among the groups (F=32.186, p<0.001; F=20.268, p<0.001; F=27.394, p<0.001; F=55.836, p<0.001). The comorbidity group had significantly higher scores in all SF-MPQ-2-CN factors than the depression and control groups (all p<0.05).
Factors relevant to impaired cognition and memory with depressive symptoms and pain-related features
To address potential risk factors for impairments of cognition and memory with depressive symptoms and CP, we performed correlation analysis to determine whether the factors with impairments of PM and RM are associated with MDD and CP. The total score of the patient self-rated BDI-II scale was positively correlated with neuropathic pain, affective descriptors and the total SF-MPQ-2-CN score (r=0.317, p=0.004; r=0.565, p<0.001; r=0.466, p<0.001). The total HAMD score was positively correlated with neuropathic pain, affective descriptors and the total SF-MPQ-2-CN score (r=0.262, p=0.018; r=0.249, p=0.024; r=0.269, p=0.015). We discovered that prospective memory was positively associated with continuous pain, neuropathic pain and the total SF-MPQ-2-CN score (r=0.431, p<0.001; r=0.253, p=0.022; r=0.320, p=0.003). Retrospective memory was positively correlated with continuous pain, neuropathic pain and the total SF-MPQ-2-CN score (r=0.415, p<0.001; r=0.247, p=0.025; r=0.314, p=0.004). In addition, we found that impairment in PM was positively correlated with the total BDI-II score and the total HAMD score (r=0.293, p=0.007; r=0.234, p=0.034). Impairment of RM was positively correlated with the total BDI-II score (r=0.355, p<0.001). We also found that marital status was negatively correlated with continuous pain and neuropathic pain (r=−0.233, p=0.035; r=−0.275, p=0.012). The results are shown in table 2 and online supplemental table 1.
Supplemental material
Correlation of the total SF-MPQ-2CN (subscale) score with demographic characteristics, BDI-II, HAMD -24, MoCA-BC and PRMQ scales
Independent predictors of chronic pain and depression symptoms
We performed stepwise regression analyses of sociodemographic characteristics, depression symptoms and memory impairment to predict pain-related factors. As shown in table 3, the final model from forward regression indicated that remarkable explanatory variables accounted for 28.8% (R2=0.288) of the variance in the total SF-MPQ-2-CN scores. A significant positive effect was found between the total SF-MPQ-2-CN score and total BDI-II score (β=0.397, t=4.009, p<0.001), and a negative effect on marital status was found as well (β=−0.297, t=−2.976, p=0.004). Furthermore, the regression model accounted for 21.8% (R2=0.218) of the variation in neuropathic pain. A significant positive effect was found between total neuropathic pain and the total BDI-II score (β=0.300, t=2.889, p=0.005), and a negative effect on marital status was also found (β=−0.312, t=−2.977, p=0.004). The regression model accounted for 35.3% of the variation in affective descriptors. A significant positive relationship was found between affective descriptors and the total BDI-II score (β=0.594, t=6.600, p<0.001). Finally, an examination of the mediator pathways revealed the indirect role of PM and RM in CP. Bootstrapping results indicated that the indirect effect was significant (indirect effect: 0.144 and 0.186, respectively) and the 95% CI had no zero values, confirming the significant mediating effect of PM and RM for CP prediction in patients with depression (figure 2).

{kind=link}
{kind=link}
Mediation analysis of the role of prospective and retrospective memory between depression and chronic pain. Mediation analysis of the role of prospective and retrospective memory between total scores of BDI-II and total scores of SF-MPQ-2-CN. BDI-II, Beck Depression Inventory-II; SF-MPQ-2-CN, Short-Form McGill Pain Questionnaire-2-Chinese. *p<0.05; **p<0.01.
Regression analysis of SF-MPQ-2-CN score (total score and subscores) with BDI-II and demographic characteristics
Discussion
Main findings
The objective of this study was to investigate the predictive role of self-reported PM and RM in patients with comorbid MDD and CP. The results verified our hypotheses that patients with comorbid MDD and CP suffer more severe clinical symptoms than patients with MDD without CP and also have more obvious PM and RM impairments. Moreover, we found that deficiencies in PM and RM were positively associated with the severity of MDD, continuous pain, neuropathic pain and the total SF-MPQ-2-CN score. Furthermore, we found support for our hypothesis that PM and RM have mediating effects on the association between depression and pain outcomes. The results showed that impairments in PM and RM could be potential prognostic factors for comorbid MDD and CP, which should be considered in treatment and intervention.
Evidence of comorbid MDD and CP indicates that high levels of chronic pain are associated with high levels of severity in depressive symptoms and lack of remission from depressive disorders.24 Some studies have shown that this comorbid state can be stressful, lead to catastrophising, rumination and helplessness, and have deleterious effects on daily activities and workplace productivity.25 Patients with comorbid MDD and CP had more severe pain-related and MDD symptoms than patients in the depression and control groups. Currently, studies have focused on identifying predictive factors for the risk of recurrence, course of the disease, residual symptoms or therapeutic resistance. Several predisposing factors may be associated, and one or more may be present in patients with comorbidity. Unmarried patients or patients with low education had lower tolerance to CP. Moreover, developmental deprivation and early loss of a parent are vulnerabilities for MDD or CP.26 In these psychologically or physically distressed circumstances, persistent pain interacting with MDD can be one of the mechanisms that may cause comorbidity symptoms.
Patients with CP display altered brain structures and functions,27 and many of the altered brain regions and networks are involved in pain perception, attitude and beliefs. Cognitive and emotional factors have a surprisingly significant effect on the disease course.28 Consistently, we found that the total MoCA-BC scores and delayed memory in the comorbid group were significantly impaired compared with those in the healthy control group, especially the ability of delayed recall. Meanwhile, deficient cognitive function seemed to have a positive relationship with neuropathic pain. Moreover, the patients in the comorbid group suffered a higher degree of pain intensity than those in the other two groups and also suffered more severe pain-related clinical symptoms, such as persistent pain, intermittent pain, neuropathic pain and difficulties with emotional description. The severity of depression exhibited a positive correlation with pain intensity, neuropathic pain and difficulties with affective descriptors. These outcomes further confirmed the complex mechanism underlying psychological pain modulation, which incorporates emotional and cognitive factors and may alter how an individual feels pain. Thus, insights into the interactive mechanism of pain perception modulation and emotional states with comorbid depression and chronic pain are relevant.
The information-processing mechanisms indicated that patients with chronic pain recalled more pain words than the controls at immediate and delayed recall, suggesting a memory bias in chronic pain. The nodes of interaction between depression and chronic pain accumulate memories of pain experiences, even their sensory attributes, over time, as well as emotions associated with them and behavioural responses.29 PM refers to the ability to remember to carry out actions at some future point in time and is an important aspect of day-to-day memory function. By contrast, RM reflects how much information is retained from a prior episode.30 The successful implementation of a PM task entails taking action when correct circumstances are encountered (prospective component) and remembering the correct action to take (retrospective component). Multiple cognitive abilities associated with PM and RM, including attention, maintenance, working memory, executive functions, information processing speed and visuospatial ability, have high integrity.31 In this present study, the results showed that the impairments of PM and RM in the comorbid group with depression and chronic pain were more severe than those in the other two groups, and impaired PM and RM were positively correlated with persistent pain, pain intensity and neuropathic pain. These results indicate that psychological cognitive processes, such as memory impairment, are involved in the clinical symptoms of depression and chronic pain, which is consistent with previous studies.32 Moreover, deficits in PM and RM potentially exerted an indirect mediating effect on patients with the comorbidity. These findings provide new insights into memory dysfunction in people with chronic pain.
Limitations
The results of the current study should be interpreted with caution because of several of its limitations. First, the intensity and features of CP were evaluated through self-assessment; thus, in future studies, we should use laboratory-based pain-measuring instruments to evaluate the characteristics of CP. Furthermore, the study had a moderate sample size, which may have limited statistical power for detecting small effects. Further studies with larger sample sizes are needed to show the impact of PM and RM impairments in comorbid MDD and CP. In addition, this study had a cross-section design, and thus we were unable to determine the causal relationship between potential risk predictors and comorbid MDD and CP. Thus, longitudinal research on this topic is needed.
Implications
In summary, our findings indicated that the severe impairments of PM and RM may cause complex symptoms in patients with comorbid MDD and CP. However, more studies are needed to explore the long-term effects of the impairments of memory processes and other cognitive functions in this vulnerable population. Determining whether alleviating deficiencies in PM and RM can reduce the burden of pain and depression for pain management is crucial.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the medical ethics committee of Anhui Mental Health Center (AMHC), ID:HSY-IRB-PJ-YN2019023. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors give special thanks to the patients for their participation, as well as the support and help from all the people who participated in this study.
References
Cuizhen Zhu is currently an associate chief physician and clinical supervisor for graduate students. She is working in the Department of Science and Education at Anhui Mental Health Center in China. She obtained a master's degree in psychiatry from the West China Medical College of Sichuan University in China in 2011 and a doctorate in psychiatry from Shanghai Jiao Tong University School of Medicine in China in 2018. Her main research interests include pain, depression, and intestinal flora.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
HG, QX and XZ contributed equally.
PJ and CZ contributed equally.
Contributors CZ and PJ were responsible for study design and manuscript editing. HG, QX, XZ, YC, JY and JG were responsible for literature searches, statistical analyses and manuscript writing. LZ, JZ, KW and CL were responsible for clinical-scale assessment data collection. CZ is responsible for the overall content as guarantor.
Funding This study was supported by funding of key research and development projects of Anhui Province (grant number: 2022e07020002), Applied medicine research project of Anhui Health Committee (grant number: AHWJ2021a036), hospital project of Hefei Fourth People’s Hospital (grant number: HFSY2020YB21), Shanghai Key Laboratory of Psychotic Disorders Open Grant (grant number: 13dz2260500 and 21-K04), Natural science research projects in Anhui Universities (grant number: KJ2020A0218), Projects supported by public welfare scientific research institutes (grant number: GY2020G-3) and the Applied medicine research project of Hefei Health Committee (grant number: Hwk2020zd0016 and Hwk2021zd011).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.