Article Text

Abstract
Background High blood pressure is a leading cardiovascular disease risk factor and considered to be associated with psychological factors. However, the causal relationships between blood pressure and anxiety, depressive symptoms, neuroticism and subjective well-being are not clear.
Aims The current study explored the genetic causal relationships between blood pressure and anxiety, depressive symptoms, neuroticism and subjective well-being.
Methods Mendelian randomisation (MR) analyses were performed using the generalised summary-data-based MR analysis method with eight large-scale genome-wide association study datasets for hypertension, systolic blood pressure (SBP), diastolic blood pressure (DBP), pulse pressure, anxiety, depressive symptoms, neuroticism and subjective well-being.
Results A causal effect of DBP on neuroticism was found, and 1074 independent instrumental single nucleotide polymorphisms were identified by the incorporated Heterogeneity in Dependent Instruments-outlier test among the bidirectional causal relationship between blood pressure and the four psychological states.
Conclusions DBP has a causal effect on neuroticism. Appropriate management of blood pressure may reduce neuroticism, neuroticism-inducing mood disorders and cardiovascular diseases.
- Anxiety
- Depression
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
As a leading risk factor for cardiovascular disease, increased blood pressure can appear in some psychological states, such as anxiety and neuroticism. Neuroticism is viewed as a key causative factor for anxiety and mood disorders.
WHAT THIS STUDY ADDS
Diastolic blood pressure has a genetic causal effect on neuroticism.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Appropriate surveillance and control of blood pressure can be beneficial for the reduction of neuroticism, neuroticism-inducing mood disorders and cardiovascular diseases.
Introduction
According to the concepts of fluid mechanics, flowing blood exerts pressure against the blood vessels, inducing blood pressure (BP). BP is measured in millimetres of mercury (mm Hg) and expressed in terms of systolic BP (SBP, maximum pressure) representing the pressure in blood vessels when the heart contracts, and diastolic BP (DBP, minimum pressure) representing the pressure in the vessels when the heart rests between two continuous contractions. The human body is said to be in a state of hypertension when the SBP is >140 mm Hg and/or the DBP readings are >90 mm Hg on 2 continuous days. Hypertension affects more than a quarter of the global population1 and is a crucial risk factor in the development of whole-body disorders, particularly heart and circulatory diseases.2 Although the aetiology of hypertension is not fully understood, the comorbidity between hypertension and psychosocial and mental disorders has been investigated by several research groups. Nevertheless, the relationship between hypertension and psychosocial disorders remains unclear and is sometimes controversial.3
Anxiety is a feeling of fear, dread and uneasiness, which is a reaction to stress. Depressive symptoms include pessimism, negative affect, low energy, anxiety and bodily pains.4 Neuroticism is a personality trait characterised as being prone to experiencing negative emotions such as anxiety, fear, distress, dissatisfaction, depression, anger and guilt. Subjective well-being is measured by survey questions on life satisfaction, positive affect and happiness. A recent controversial systematic review and meta-analysis suggested an association between anxiety and increased risk of hypertension, based on the evidence from cross-sectional and prospective studies.5 While there is growing evidence of a relationship between psychosocial states and altered BP, the pathophysiological mechanisms underlying these relationships are unclear or contradictory. The causal effects of BP on anxiety, depressive symptoms, neuroticism and subjective well-being have not yet been elucidated.
Genome-wide association studies (GWASs) are powerful resources for identifying genetic variants contributing to a trait. There are GWASs that consider anxiety, depressive symptoms, neuroticism and subjective well-being, which can provide human genomic information about these psychological states. Mendelian randomisation (MR) analysis is currently a popular method to examine the bidirectional genetic causal effects between two traits based on GWAS summary data.6 7 This method can be used to explore the causal effects of BP on psychological states at the genetic level.
Therefore, this study aimed to explore the causal relationships between BP and anxiety, depressive symptoms, neuroticism and subjective well-being based on large samples of GWAS data.
Methods and materials
Study design
Bidirectional two-sample MR analyses were performed to explore the causal association between the exposure (a risk factor) and the outcome (a phenotype). Genetic variants associated with the exposure were selected as instrumental variables. For one direction of the MR analysis, the four BP traits (SBP, DBP, pulse pressure (PP) and hypertension) were treated as the exposure, and the four psychological states (anxiety, depressive symptoms, neuroticism and subjective well-being) were treated as the outcome. For the other direction of the MR analysis, this assignment was reversed. The study had three phases: (1) collecting summary-level GWAS data for the eight traits, (2) exploring genetic variants to serve as instrumental variables, and (3) estimating the causal effects of the exposure on the outcome.
Data collection and extraction
The flowchart of the current study is described in figure 1. First, the GWAS datasets from European populations for the four psychological states were obtained. The anxiety GWAS dataset was obtained from the MR-base database.8 The depressive symptoms GWAS dataset was obtained from the UK Biobank (UKB), Genetic Epidemiology Research on Adult Health and Aging (GERA), and Psychiatric Genetics Consortium (PGC).9 The neuroticism GWAS dataset was obtained from the UKB and Genetics of Personality Consortium (GPC).10 All disorders were assessed using standard diagnostic criteria. The subjective well-being GWAS dataset was obtained from a meta-analysis on summary association statistics from 59 cohorts.4 Subjective well-being was classified into four phenotypical panels: primary subjective well-being, life satisfaction, positive affect and post hoc subjective well-being.

Study flowchart. GERA, Genetic Epidemiology Research on Adult Health and Aging; GPC, Genetics of Personality Consortium; GWAS, genome-wide association study; MR, Mendelian randomisation; PGC, Psychiatric Genetics Consortium; UKB, UK Biobank; ICBP, International Consortium for Blood Pressure; MRC-IEU, Medical Research Council-Integrative Epidemiology Unit.
GWAS data for DBP and SBP were retrieved from the study by Guo et al.11 The GWAS dataset for PP was included as PP has been proposed to describe the difference between SBP and DBP, and is viewed as an independent risk predictor for whole-body disorders (table 1).12 The hypertension GWAS dataset, with the largest sample size within the MR-base database, also included abnormal BP, defined as SBP >140 mm Hg and/or DBP >90 mm Hg on 2 continuous days.8 All participant samples in each GWAS were of European ancestry. Ethical approval had been obtained in all original studies.
Summary of European genome-wide association study data on various blood pressure, anxiety, depressive symptoms, neuroticism and subjective well-being traits
Detailed descriptions of participant characteristics can be found in each study. All participants were included in only one study. Genotyping was performed on genome DNA extracted from blood samples according to standard procedures from a range of commercially available genotyping arrays, as described in the original reports. Genotype imputation was performed using the 1000 Genomes Project reference panel and IMPUTE2 software.13 For each GWAS dataset, all biallelic single nucleotide polymorphisms (SNPs) and SNPs with an imputation score >0.9 were considered for the next analysis, while ambiguous SNPs were excluded. If an SNP was mapped to opposite strands in either dataset, its alleles in the second dataset were flipped.
MR analysis
MR analysis infers the credible causality of a relationship between the exposure and the outcome by leveraging instrumental variables, which are expected to be independent of confounding factors.14 In MR tests using GWAS data, genetic variants are treated as instrumental variables to test for causality. Due to the possibility of correlated or uncorrelated pleiotropy of genetic variants,15 exploiting GWAS data with large independent samples can greatly improve the power of an MR analysis. Genetic variants used as instrumental variables need to meet three assumptions; they should: (1) be associated with the exposure, (2) only affect an outcome via the exposure, and (3) be independent of confounders. The MR checklist for Strengthening the Reporting of Observational Study in Epidemiology is provided in the online supplemental materials.16
Supplemental material
The Genome-wide Complex Trait Analysis tool (V.1.93.3 beta2) was used to explore bidirectional causal links between each psychological state and each BP trait in the framework of Generalised Summary-data-based MR (GSMR).17 This method is based on summary-level data, using independent genome-wide significant SNPs as instrumental variables, that is, an index of the exposure to test for putative causal associations between a risk factor (exposure) and an outcome. Instrumental variants were selected based on the default GWAS threshold of p≤5×10−8. An LD (linkage disequilibrium) threshold of r2=0.05 was used to identify independent SNPs based on the European population as referenced within the 1000 Genomes Project (phase 3). Heterogeneity in Dependent Instruments (HEIDI)-outlier detection was used to filter genetic instruments that had obvious pleiotropic effects on the exposure and outcome. A threshold p value of 0.01 was used for the HEIDI analysis.18 We used an F-statistic >10 to define SNPs as valid instrumental variables. Ten was the minimum number of instrumental SNPs required. The power for the MR analysis was calculated using an online calculator (http://sb452.shinyapps.io/power/). P values were adjusted using the Bonferroni method, multiplying by 32 for multiple tests.
Results
The GWAS summary datasets obtained are listed in table 1. The maximum sample size of BP traits was 736 650 for SBP, DBP and PP, and the minimum was 463 010 for hypertension. The maximum sample size for psychological states was 463 010 for anxiety, and the minimum was 170 911 for neuroticism. There were no participants who appeared in both the BP and psychological state datasets.
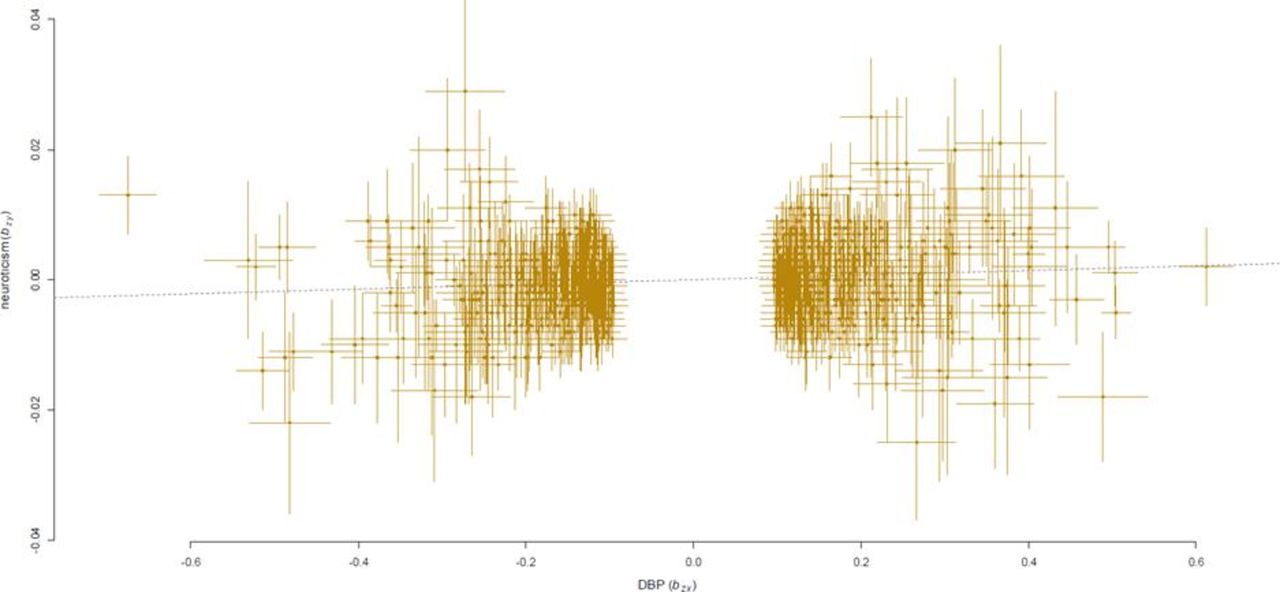
With BP traits as exposure and psychological states as outcome, hypertension and DBP had significant causal effects on neuroticism (p=8.8×10−6 and 0.026, respectively, table 2). After adjusting for multiple tests, only DBP was significantly associated with neuroticism (bxy=0.003 6, table 2; pbonferroni =0.000 28). There were 1074 independent instrumental SNPs, which were significantly associated with DBP but not with neuroticism (online supplemental table 1 and figure 2). These instrumental SNPs, with F-statistic >10, were independent with an LD r2 less than 0.05 and survived the HEIDI-outlier analysis that removes horizontal pleiotropic SNPs with p<0.01. No significant causal effects were found for other BP traits and each psychological state.
Supplemental material
Results of Generalised Summary-data-based Mendelian Randomisation analysis

{kind=link}
{kind=link}
The causal effects of DBP on neuroticism. The dotted lines denote effect sizes (bxy). DBP, diastolic blood pressure.
The reverse causal effects analysis indicated that after clumping and HEIDI-outlier filtering of SNPs, less than the default threshold of 10 independent instrumental variants were retained in the analysis. Since anxiety, depressive symptoms, neuroticism and subjective well-being are complex traits, limited independent instrumental variants may provide biased results. However, without the limit of this threshold, no significant causal association of each psychological state with any BP trait was found. The power of our MR analysis in all pairs of exposure and outcomes was >90%, given the sample size for the relevant variant-outcome associations, at an alpha of 5%.
Discussion
Main findings
As high BP is a leading risk factor for cardiovascular disease, the relationship between BP and psychological factors is undeniable. However, the causal effects between BP and anxiety, depressive symptoms, neuroticism and subjective well-being are not well distinguished. In this study, we have, for the first time, used GSMR analysis methods and found a causal effect of DBP on neuroticism.
In this study, MR use was based on the assumptions that genetic variants are associated with the exposure factor, are not related to confounding factors associated with the outcome, and must affect the outcome through the exposure factors. MR method is developed to infer the causal relationship between the exposure factors and outcome.14 Genetic variants from GWASs are usually treated as instrumental variants for their stability and randomness; however, they may cause horizontal pleiotropy where variants affect outcome and exposure traits via a shared heritable factor (correlated pleiotropy) or separate mechanisms (uncorrelated pleiotropy), other than a causal effect.15 The GSMR method is considered more powerful than other summary data-based MR approaches19 20 and incorporates the HEIDI-outlier test to identify loci that influence multiple phenotypes, such as pleiotropy effects on the exposure and outcome.21
Limitations
Current large-scale GSMR analysis reduces the biases caused by confounding factors in observational studies, using random genetic variants as instrumental variables, which may represent lifelong influences and increase the precision of the analysis results. However, there are potential limitations of the current analysis: first, the incorporated HEIDI-outlier test in GSMR can identify loci affecting multiple phenotypes, such as pleiotropy effects on the exposure and outcome21; nonetheless, the possibility of residual pleiotropy cannot be completely excluded. More methods are required to evaluate the independence of variants and analysis results. Second, current analyses were predominantly on populations of European ancestry, and therefore, the findings may not be generalisable to other populations. Third, a stringent Bonferroni correction was used to judge the positive MR findings, which may have caused false-negative findings and minimised the ratio of false-positive results.
Implications
BP is an important indicator of blood circulation and is one of the vital signs. BP has 30%–60% heritability, and over 1000 SNPs have been significantly associated with this complex trait by large-scale GWASs.22 Some psychological factors, such as mental stress and anxiety, may cause sudden high BP and increase blood fluidity by activating the sympathetic nervous system.23 Anxiety, anger and happiness increase BP, and emotional effects have greater variability in individuals with more labile BP.24 In pharmacological studies of hypertension, a reduction of BP in placebo groups is often found, which differs from spontaneous remission and regression to the mean effect of comparing placebo groups with untreated groups.25 26 The role of BP in psychosomatic medicine is implied as BP is a link between the brain and the heart, and thus may promote the development of personality traits. Individuals with neuroticism can be sensitive to the criticism of others, are often self-critical, and easily develop anxiety, anger, worry, hostility, self-consciousness, and depression. Neuroticism is viewed as a key causative factor for anxiety and mood disorders.27 Individuals with neuroticism more frequently experience high mental stress, which can lead to elevated BP and cardiovascular diseases.28 Thus, appropriate management of BP may reduce neuroticism, neuroticism-inducing mood disorders and cardiovascular diseases.
In conclusion, using GWAS datasets with large sample sizes, we found that, among the causal relationship between BP and psychological states, DBP had a causal effect on neuroticism but not on the other psychological states of anxiety, depressive symptoms, or subjective well-being. Since the independent instrumental SNPs for these four psychological states are limited, future studies are required to explore the causal relationship between psychological states and BP.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but the Bioethics Committee of Bio-X Institutes of Shanghai Jiao Tong University exempted this study. Participants gave informed consent to participate in the study before taking part.
References
Lei Cai is an associate professor of Bio-X Institutes, Shanghai Jiao Tong University in China, and a member of Shanghai Jiao Tong University Institutional Review Board (IRB) for Human Research Ethics. He obtained his PhD degree from Fudan University, China, and has worked as a research assistant at the Harvard School of Public Health, USA. He has published over 50 papers and four chapters for three books, and has had two invention patents authorised. He has been the PI on several projects and research tasks, such as the National Natural Science Foundation of China, Shanghai, the Ministry of Education (MOE) Scientific Research Foundation, and the Key Research and Development Program of the Ministry of Science and Technology. His main research interests include the molecular basis of mind-body interactions and big data analysis.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LC conceived and wrote the whole manuscript. LC and YL analysed the data. LC and LH proofread the manuscript. LC is the guarantor for the manuscript.
Funding This project was funded by the Natural Science Foundation of Shanghai (19ZR1427700).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.