Article Text

Abstract
The biomedical model, which limits itself to finding the attributions of organic disease, is challenged by gastrointestinal (GI) symptoms. Simultaneously, physicians' attribution of GI symptoms to underlying psychological issues is not readily accepted by patients and can negatively affect the clinical rapport between doctor and patient. In reality, psychosocial aspects are involved in many functional disorders and organic diseases, not just in mental disorders. Time is overdue for gastroenterologists to recognise the inadequacy and limitations of conventional gastroenterology and consider the role of psychological, social and biological variables throughout the entire clinical course of the illness, as is shown in George Engel’s model. This review discusses the following: (1) the current challenges of using the conventional clinical model for both functional and organic GI illness, (2) the inadequacy and limitations of explaining GI symptoms simply as psychological disorders, (3) the exploration of the symptom-centred, stepped reattribution clinical model, (4) the clarification of psychosomatic medical concepts for use in gastroenterology, and (5) the significance of a systematic and interdisciplinary framework for a comprehensive psychosomatic model in gastroenterology.
- psychosomatic medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Current medicine often uses a disease-centred model that reduces or attributes all symptoms to certain diseases.1 2 Assessment systems for making diagnoses are limited primarily to biological measurements3 4 such as laboratory examination, gastrointestinal (GI) endoscopy, intestinal microbiota5 and medical imaging techniques, such as computerized tomography (CT) scanning, that are used in conventional gastroenterology. However, many clinical phenomena cannot be measured using biological methods or even psychological scales.6 7 When these methods are used, the findings may overlook important data or lack clinical clarity.8 Against this background, three main challenges continue to confound gastroenterologists: (1) no biological aetiology can be found to explain so-called functional GI symptoms, (2) symptoms co-existing with certain organic diseases are difficult to treat and explain solely by the primary diagnosed disorder, and (3) iatrogenic stresses contribute to emotional and physical symptoms in gastroenterology. This review discusses how gastroenterologists can confront these challenges without the restrictions of the biomedical model. A better understanding of the holistic medical model as posited by Engel4 and its application to the practice of psychosomatic medicine may aid in solving some clinical issues found in gastroenterology that cannot be explained biologically. Finally, a completely new systematic framework of psychosomatic gastroenterology will be established.
Challenges in the conventional clinical model
Biomedical assessments in conventional gastroenterology are limited to the assumption that all symptoms can be reduced to certain diseases.1 2 This model only works in the diagnosis and treatment of some medical conditions. For instance, when a patient complains that he is suffering from a pain that shifts from the epigastric area to the right lower quadrant of the abdomen, the physician can diagnose acute appendicitis based on the stable tenderness and rebounding pain that was found on physical examination. In that case, surgery would solve the problem. However, most clinical problems cannot be solved in this way. One of the diagnostic problems gastroenterologists face is that many patients with numerous GI symptoms have no disease that can be detected, even after a thorough examination that includes endoscopy and medical imaging. Sometimes, organic diseases can be found, such as GI polyposis, chronic gastritis and intestinal metaplasia. However, they are inadequate to explain the symptoms that the patient is experiencing. These GI diseases can be treated according to the guidelines of various advanced endoscopic techniques, but this often does not result in relief from symptoms. Since 2016, gastroenterology has described these symptoms as functional gastrointestinal diseases (FGIDs) and gut-brain interaction disorders.9 Pure functional GI problems have attracted the interest and attention of all gastroenterologists. The Rome Foundation for Functional Gastrointestinal Disorders, established in the late 1980s, is the most influential academic organisation for functional GI disorders in the world and has made many important contributions10 to the field. Another issue that puzzles gastroenterologists is that some patients with organic diseases have symptoms that do not correlate to disease aetiology or severity. All standard treatments for these organic diseases are ineffective. For example, the Disease Activity Index of patients with inflammatory bowel diseases (IBD), such as ulcerative colitis (UC)11 or Crohn’s disease, shows that intestinal inflammation has been controlled well through standardised treatment strategies. However, there are still many GI symptoms that cannot be explained, labeled as 'functional symptoms complicated with IBD'12, 'residual symptoms of IBD', or IBD-irritable bowel syndrome (IBD-IBS).13 14 Fortunately, recent integration of interventions utilizing a psychosomatic model involving psychosocial variables offers a promise that a new dawn of approaches for gastroenterologists has arrived.
Clinicians should recognise the contributions that biological science and biotechnology have made to the medical field and continue to use evidence-based methods in clinical practice. But some medical issues should be considered more holistically, such as the gastroenterology issues that cannot be solved using conventional methods. In the past, some clinicians resorted to unconventional methods that were considered unscientific because scientists had not yet studied those particular problems or approaches. The actions of many of these early forerunners, however, were not contrary to the scientific spirit and, in fact, provided new evidence for later research, thereby accelerating the development of the field. Keeping this in mind, it is unreasonable to view and treat clinical problems that have multidimensional facets from a single biological disease dimension.10
The inadequacy of a simple psychological explanation
The explanation and attribution of functional symptoms is troublesome for clinical medicine. Clinicians first need to convince themselves regarding an explanation before they are able to offer patients acceptable medical interventions. What they especially must bear in mind is that patients require an understandable and acceptable explanation, otherwise no subsequent intervention can be made. Under the current biomedical model, it is not feasible, and is even considered wrong for doctors to offer psychological explanations for unexplainable symptoms. Patients do not accept such explanations. Understanding, explaining and treating functional symptoms from the perspective of psychiatry is a great leap in the process of the physicians’ cognition. The Rome Foundation for Functional Gastrointestinal Disorders put forward the basic framework and principles of psychological interventions in FGID more than 15 years ago.15 Three consecutive meta-analyses on IBS conducted by Ford et al 14 16 17 over the course of 13 years showed psychotherapy and antidepressants were effective at improving the symptoms of FGID and the overall quality of life. However, if clinicians too readily attribute functional symptoms to psychiatric disorders, such as anxiety or the somatisation found in depressive disorders, they are simply moving to the other extreme of causation in which all of these symptoms are attributed to psychiatric problems without consideration of organic causes. By determining a psychological origin for these symptoms, clinicians may emphasize the use of antidepressants or psychotherapy while ignoring the patient's thoughts and behaviours (eg, various types of food avoidance)18 that are related to GI beliefs. Although the psychosocial background of patients is complex, a commonality among these patients is an irrational understanding and interpretation of their disease and symptoms. Hence, to solve the psychological problems of these patients, we should first find and resolve the health-related or GI-specific psychological misperceptions. Then it would be possible to expand interventions to address more general psychological problems in the patients' lives. The symptom-centred, stepped reattribution model, based on the above views, has gradually developed over time and achieved good clinical efficacy.19 20 Microbiologists, for example, cannot deal with all the infectious diseases encountered in clinical practice. Likewise, it is impractical for psychiatrists or psychologists to handle all the functional symptoms complicated by FGID or IBD. Moreover, most patients with digestive symptoms would not consider visiting these specialists for their issues and if a gastroenterologist should refer a patient to a psychiatrist, his relationship with the patient may become strained.
Exploration of symptom-centred, stepped reattribution clinical model
The symptom-centred, stepped reattribution model19 20 that fits within the holistic psychosomatic approach to medicine has been applied to the practice of gastroenterology. The reattribution model for functional somatic symptoms was first proposed by Morriss et al.21 Using short-term training, it promoted the clinical skills of physicians, especially, non-psychiatrists and general practitioners, to diagnose and intervene in cases with medically unexplained symptoms (MUS). The Danish physician Fink et al 22 modified the model and then formed a national training programme in Denmark to enable more physicians to learn how to make mental reattribution of MUS clinically, which helped non-psychiatrists deal with these clinical dilemmas. However, this reattribution was basically only one step forward. Because of fears of stigma (especially among those with an Asian cultural background),23–26 it is difficult for patients to easily accept the psychological reattribution of the cause of their symptoms and the related interventions, such as psychotherapy--due to low motivation27--or the use of central neuromodulators, such as antidepressants, antipsychotics and other central nervous system-targeted medications. Therefore, a symptom-centred, stepped reattribution model has been developed specifically for patients with FGID by drawing upon principles from cognitive-behavioural therapy (CBT), Ellis’s rational emotive therapy (RET), and the core content of the reattribution model training for non-psychiatrists proposed by Fink et al.22 The specified steps and key points of operation are as follows:
Establish a psychosomatic link for symptoms, namely symptom-centred reattribution, as the first step of reattribution. Focus the centre of attention on the somatic symptoms of patients with FGID, instead of their psychological issues. Use the techniques of CBT and RET flexibly according to the patient’s gender, age, occupation and other personal characteristics. Then, appropriately dialogue with the patient about the attribution of FGID symptoms. The goal is to alleviate or even eliminate the symbolic significance of the symptoms, that is, the patient’s improper conceptualization and cognitions regarding their bodily symptoms. Finally, help them establish a new cognitive structure for FGID. Meanwhile, avoid groundless biological attribution of somatic symptoms of FGID and premature negative attribution of general psychosocial aspects.
Establish three diatheses (confidence, determination and patience) by discussing drug therapy with patients. The details are as follows: give the reasons for using antidepressants and eliminate the bias patients may have to increase confidence in drug therapy. Also, actively and objectively discuss the side effects of psychotropic medications. Explain the slow-acting nature of antidepressants to manage patients’ expectations and stress their need for patience with treatment. Any foreseeable side effects from antidepressants should not be exaggerated or ignored. Patients or their family members should read the drug instructions carefully and then ask questions. They are encouraged to discuss any drug-related concerns with physicians.
Work with patients to modify any distorted thinking surrounding symptoms. Additionally, any behaviours such as food avoidance, should be dealt with through psychotherapy and dietary training, which is similar to exposure therapy28 under the guidance of gastroenterologists, to modify health cognitions and behaviours.
Strengthen the therapeutic relationship so that patients can recognise the psychosomatic connection of symptoms more clearly. This is usually brought up in subsequent clinical sessions, especially after antidepressants become effective.
Perform a psychosocial reattribution for areas unrelated to GI symptoms. This is also considered the second step of reattribution and usually performed after the establishment of a good therapeutic relationship and the alleviation of somatic symptoms. This step helps patients modify their maladaptive beliefs and behaviours in daily life. At this stage, their negative perceptions of digestive tract symptoms are significantly improved, the resistance to psychological interventions is usually reduced, and the motivation for psychotherapy is enhanced. It is also easier at this point for a gastroenterologist to refer patients to counsellors for psychotherapy and further treatment to enhance their overall well-being.
The cornerstone of the model is integration rather than separation of mind and body. This embodies the holistic medical approach of mind-body monism. The three key concepts of the model are symptom-centred, stepped, and reattribution. The first concept, symptom-centred, has a double meaning. First, the symptom-centred approach takes the pathological significance of symptoms into consideration.2 Comprehensive evaluation using the biomedical model will prevent misdiagnosis of organic diseases. Second, when the results of a biomedical assessment cannot be properly explained, a psychosomatic assessment and intervention will be taken into consideration. Symptom-centred means that physicians should focus on symptoms together with patients instead of becoming impatient with symptoms that lack pathological significance. This helps patients feel that their symptoms are accepted and understood by physicians and facilitates strong clinical rapport. Reattribution in a stepped manner helps reduce conflict that can occur with hasty reattribution. It is not difficult to see that the symptom-centred, stepped reattribution model is also suitable for other areas of clinical work.
Finally, it should be noted that according to the mental health laws of China, gastroenterologists are not able to diagnose mental disorders. Therefore, for these Chinese physicians to make a successful referral to psychiatry, the following conditions should be screened when conducting a clinical interview9 19: (1) warning signs for suicide; (2) difficulties in communication between the physician and patient; (3) irrational and clinically significant strong beliefs in certain organic diseases; (4) persistent pain; (5) severe impairment in social functioning; (6) malingering; and (7) other identifiable and severe mental disorders.
Clarification of psychosomatic medicine in gastroenterology
Psychosomatic medicine has no universal definition. Due to the uncertainty of definition and connotation, psychosomatic medicine is not always well distinguished from psychogenic and holistic medicine and is often misidentified with them.29 30 It is, therefore, necessary to clarify what psychosomatic medicine is in order to ensure its effective use in the real world of clinical practice. Currently, psychosomatic medicine has three general models29 31:
(1) Psychosomatic medicine is a special field or subspecialty of psychiatry, basically a synonym for consultation-liaison psychiatry, whose practitioners are mainly psychiatrists. Its purpose is to identify, diagnose and treat complicated psychiatric disorders in non-psychiatric medical settings. The target of identification and treatment is psychiatric disorders instead of the physical symptoms and other diseases of patients. In the USA, psychosomatic medicine was officially approved as a subspecialty of psychiatry in 2003. Therefore, it is also a mainstream model of psychosomatic medicine in the USA.
(2) Psychosomatic medicine is a primary discipline independent of psychiatry, internal medicine, and surgery; it is a branch of medicine that is mainly used in Germany and Japan. It is difficult to define the scope of its application as its acceptance and application by non-psychiatric specialties continues to be challenged, although the concept differs from consultation-liaison psychiatry.
(3) Psychosomatic medicine utilizes the method or means of holistic medicine to work with patients. The concept has been under development for nearly 40 years. It originated from the biopsychosocial model of Engel in the late 1970s,32 33 which comprehensively considers biological, psychological and social factors throughout the entire process of assessment, diagnosis and treatment. The model can be applied to all clinical specialties, including psychiatry.
Summarizing the above, the comprehensive psychosomatic model can be considered as a third method of medical intervention for gastroenterology patients, in addition to medication and surgery. Because of the differences in understanding psychosomatic medicine, its practice in gastroenterology takes many different forms. Presently, the three main forms are as follows34:
(1) Biomedically oriented psychosomatic gastroenterology belongs to ‘brain-body’ medicine rather than ‘mind-body’ medicine as the brain itself is a part of the body.
(2) Psychiatry-oriented psychosomatic gastroenterology belongs to a subspecialty of psychiatry.
(3) Holistic medicine-oriented gastroenterology is an application of the biopsychosocial medical model in gastroenterology.
From this point of view, the psychosomatic model in gastroenterology is an interdisciplinary framework, which includes:35 36 the assessment of psychosocial factors affecting individual vulnerability, clinical course and outcome for any type of GI diseases; holistic consideration of patient care in clinical practice; and integration of psychotherapy, psychopharmacological and GI pharmacological treatment in the prevention, treatment and rehabilitation of various GI diseases, whether organic or functional.
Psychosomatic gastroenterology as a systematic and interdisciplinary framework
Psychosomatic gastroenterology originated from the clinical diagnosis and treatment of FGID. From the publication of the first document on diagnostic criteria for IBS in 1989 to the publication of Rome Ⅳ in 2016,9 it has been clear that psychosocial aspects are widely involved in the development of FGID.37 At the same time, it has also been suggested that psychological interventions, tricyclic antidepressants and selective serotonin reuptake inhibitors can be added to the treatment strategies of FGID, according to the condition of the patient, and making an active psychiatric referral when needed has been seen as a wise clinical principle.15 IBD-IBS have been mentioned in cases within the Rome Ⅳ Multidimensional Clinical Profile for Functional Gastrointestinal Disorders.10 This means that the treatment strategies for GI symptoms are moving from being considered for a primary functional disorder to those secondary to organic diseases. The conventional psychiatric-oriented psychosomatic model is obviously inadequate. Psychosomatic gastroenterology should have a broader scope as well as a systematic and interdisciplinary framework.
The author believes that the domain of the psychosomatic model in gastroenterology includes: (1) abnormal beliefs and health-seeking behaviours like doctor shopping and cyberchondria38; (2) functional GI symptoms related to general psychological factors; (3) GI symptoms associated with psychiatric disorders and side effects of psychotropic drugs; (4) psychiatric symptoms complicated with such organic GI diseases, that is, hepatic encephalopathy; (5) unexplained symptoms in organic GI diseases, such as residual symptoms of IBD or IBD-IBS 13 39 40; (6) iatrogenic stress induced by biological markers and medical terminologies, such as tumor markers, Helicobacter pylori, intestinal metaplasia; (7) excessive GI surgeries without adequate evidence of symptoms attribution; and (8) psychosomatic rehabilitation.
In patients with IBD, for example, evaluation for rehabilitation should include measures for at least these four aspects : (1) mucosal healing by endoscopy; (2) active level of inflammation by scales like Ulcerative Colitis Activity Index12; (3) symptom dimension; and (4) psychological well-being. Current gastroenterology is focused primarily on the former two aspects and inadequately or totally fails to address the latter two aspects. Psychosomatic medicine can be of great help in addressing these aspects. The systematic and interdisciplinary framework for psychosomatic gastroenterology that we are advocating should cover the entire clinical course from interview and assessment to intervention, intragenic stress prevention and rehabilitation of patients with both functional illness and organic disease in a manner illustrated by the steps of the psychosomatic process as shown in figure 1.34 41
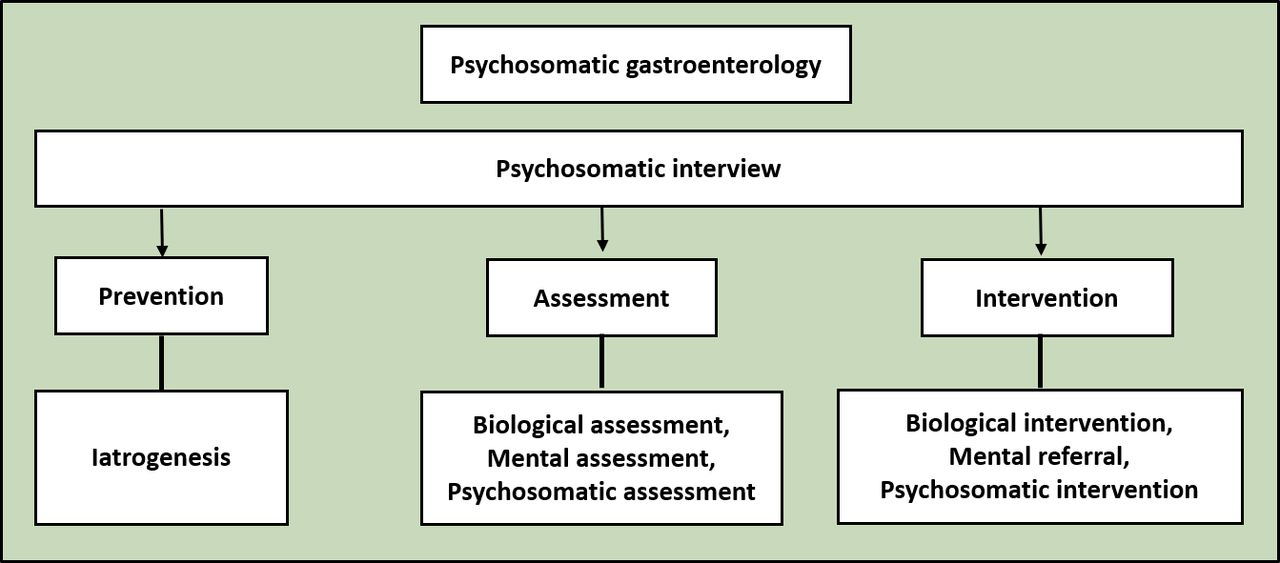
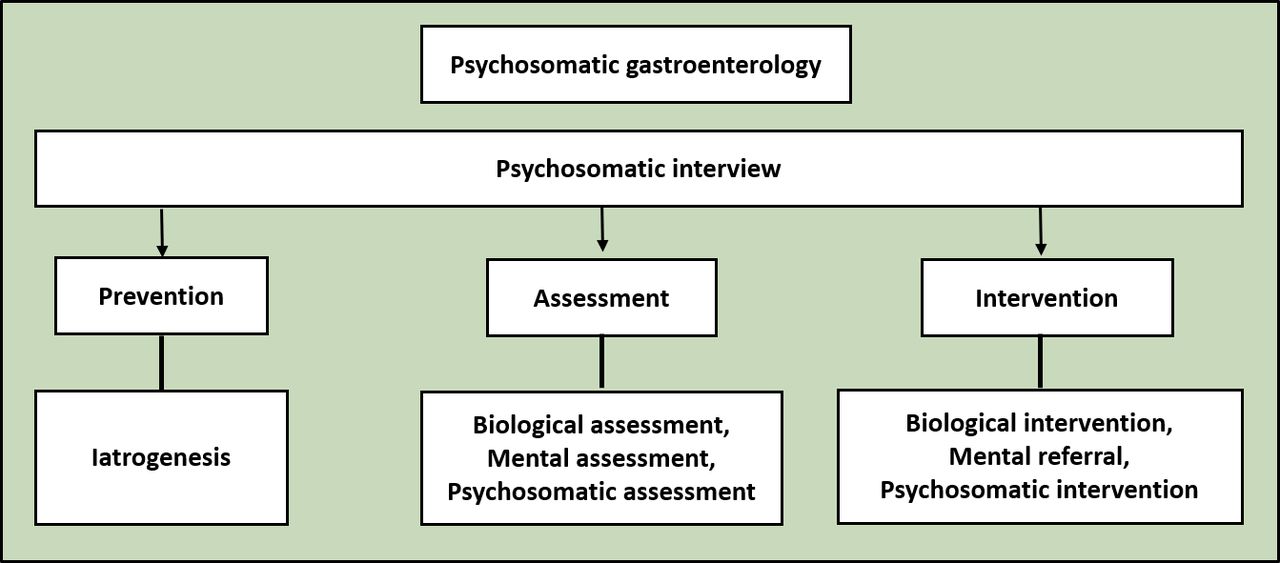{kind=link}
The comprehensive framework of psychosomatic gastroenterology.
Conclusion
A large number of clinical problems in gastroenterology involve psychosocial aspects. Besides affecting the prognosis of patients, they are an important source of tension in the doctor–patient relationship. Psychosomatic gastroenterology does not mean that gastroenterologists should offer psychological counselling, or become professional psychotherapists or psychiatrists. Rather, it encourages gastroenterologists to shed the limitations or inadequacies of relying solely upon the biomedical model or the conventional psychiatric model, while simultaneously learning more about psychology and psychiatry; this knowledge could be applied to clinical practice and promote better strategies for gastroenterology. There is an urgent need to move away from the strictly biological model and incorporate biological, social and psychological factors into the clinical practice of gastroenterology.42 A comprehensive, systematic and interdisciplinary psychosomatic framework of gastroenterology with multiple dimensions is urgently needed.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Qiaoli Zhang received her master’s degree in Psychiatry from Xuzhou Medical University, China in 2015. She is currently a psychiatrist at the Third Affiliated Hospital of Soochow University in China. She is also a researcher at the Institute of Psychosomatic Gastroenterology of Soochow University. She also has expertise in clinical psychology and psychosomatic gastroenterology. Her research interests include assessment and intervention of psychosomatic gastroenterology.

Lixin Ding received her master degree in Gastroenterology from Soochow University in China in 2021. She is currently a physician at the Third Affiliated Hospital of Soochow University. She does research at the Institute of Psychosomatic Gastroenterology of Soochow University. She majors in psychosomatic gastroenterology. Her research interest includes assessment and intervention of psychosomatic gastroenterology.

Jianxin Cao, MD, received his master degree in Gastroenterology from Nantong Medical College in China in 1992. He worked as a visiting fellow at Gastroenterology Department of Tokyo Medical and Dental University Hospital and Tokushima University Hospital in Japan between 2002-2004. He is the founder and chairperson of Soochow University Psychosomatic Gastroenterology Institute, chief physician of the Third Affiliated Hospital of Soochow University, member of international college of psychosomatic medicine (ICPM), member of the American psychosomatic society (APS). He currently serves on the editorial board of Psychotherapy and Psychosomatics, published by Karger in Basel (IF = 25.6).

Footnotes
QZ and LD contributed equally.
Contributors QZ and LD contributed equally to manuscript writing and editing. JC contributed to the frame and directing of the paper. All authors read and approved the final manuscript.
Funding This study was funded by Changzhou Municipal Government Science and Technology support foundation (CE20215023) and Psychosomatic Gastroenterology Institute start-up foundation from The Third Affiliated Hospital of Soochow University.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.