Article Text

Abstract
Background The management of modifiable risk factors and comorbidities may impact the future trajectory of cognitive impairment, but easy-to-implement management methods are lacking.
Aims This study investigated the effects of simple but comprehensive cognitive health management practices on the cognitive function of older adults in the community with normal cognition (NC) and mild cognitive impairment (MCI).
Methods The comprehensive cognitive health management programme included a psychiatric assessment of the cognitive risk factors for those in the intervention groups and individualised recommendations for reducing the risks through self-management supported by regular medical professional follow-up. The intervention groups for this study included 84 elderly participants with NC and 43 elderly participants with MCI who received comprehensive cognitive health management. The control groups included 84 elderly participants with NC and 43 elderly participants with MCI who matched the intervention group’s general characteristics and scale scores using the propensity matching score analysis. The Montreal Cognitive Assessment (MoCA) scale and Geriatric Depression Scale (GDS) scores were compared after a 1-year follow-up.
Results For older adults with MCI in the intervention group, MoCA scores were higher at the 1-year follow-up than at baseline (24.07 (3.674) vs 22.21 (3.052), p=0.002). For the MoCA subscales, the intervention group’s abstract and delayed memory scores had significantly increased during the 1-year follow-up. Furthermore, in a generalised linear mixed model analysis, the interaction effect of group×follow-up was statistically significant for the MCI group (F=6.61, p=0.011; coefficients=5.83).
Conclusions After the comprehensive cognitive health management intervention, the older adults with MCI in the community showed improvement at the 1-year follow-up. This preliminary study was the first to demonstrate an easy-to-implement strategy for modifying the cognitive risk factors of elderly individuals with MCI in the community, providing new insight into early-stage intervention for dementia.
- cognition disorders
- cognition
- depression
- case-control studies
Data availability statement
No data are available. No additional data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Much research has supported the notion that promoting sports and social interaction, reducing depression and implementing cognitive training measures could reduce the incidence of cognition disorders, or at least their severity.
WHAT THIS STUDY ADDS
After the comprehensive cognitive health management intervention, older adults with mild cognitive impairment (MCI) in the community showed improvement at the 1-year follow-up.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This preliminary study was the first to demonstrate an easy-to-implement strategy for controlling the modifiable risk factors of cognition for elderly individuals with MCI in the community.
Introduction
As the global population of elderly adults rapidly increases, the incidence of neurocognitive disorders will triple to 152 million by 2050, making it the most severe health challenge facing humanity in the 21st century.1 A research study in 2012 shows that the social cost incurred by patients with neurocognitive disorders almost equals the combined costs of cancer, heart disease and stroke.2 3 There are no reversals for this degenerative illness, but early standard intervention could maximise patients’ quality of life and reduce the burden of the disease. Alzheimer’s disease (AD) is the most common type of neurocognitive disorder. In 2017, Livingston et al reviewed the risk factors for AD. They believed it was possible to prevent AD by promoting sports and social interaction, reducing depression and implementing cognitive training measures.4 Therefore, identifying risk factors of older adults and implementing interventions to address them may be an effective means to reduce the incidence of the disease, or at least its severity. Mild cognitive impairment (MCI) is a transitional state between normal ageing and early dementia. The prevalence of MCI in older adults aged 60 years or above in China ranges from 15.5% to 27.8%, and the proportion of MCI progressing to AD within 5 years is 10%–15% every year.5 6
However, today in China, cognitive disorder screening, diagnosis and intervention remain deficient. Few intervention methods are known and carried out by older adults with MCI or subjective cognitive decline (SCD). There are several reasons for this. First, elderly persons in Chinese communities do not actively participate in available intervention offerings because of insufficient awareness of cognitive impairment. For example, one study in Shanghai showed that 45% of people believed that ‘dementia is a normal part of ageing’, and only 30% of those interviewed knew the necessity for medical treatment.7 8 Second, cognitive disorders have not been included in policies that address the daily management of chronic diseases and are not prioritised by community physicians in primary medical and health institutions that lack cognitive screening and diagnostic technology. Studies abroad have shown that the sensitivity of community doctors for the diagnosis of mild dementia is only 0.14–0.330.9 Third, professionals and institutions in geriatric psychiatry and neurology tend only to treat and care for patients with dementia more severe than MCI and SCD. Finally, because there is a lack of effective drug treatments, the public have low expectations for treatment benefits,10 which leads to decreased hope and searching for disease treatment and intervention.
Based on the barriers and practical significance of early-stage screening and intervention, we developed a comprehensive cognitive health management method focusing on strengthening health management with risk factor-targeted recommendations by medical professionals in community settings. In this study, we selected elderly residents over 60 years of age in multiple communities in Shanghai for cognitive function screening, conducted comprehensive cognitive health management for a portion of those with normal cognition (NC) and MCI, and then explored the effect on cognitive function. Finally, we sought to verify whether this early-intervention method could be promoted in Chinese communities.
Methods
Participants
Cohort 1 was part of the database of the Shanghai Action of Dementia Prevention for the Elderly (SHAPE) initiated in 2017. It consisted of elderly residents in Shanghai with NC or MCI and patients with dementia. Participants underwent a screening process that included a physical examination, blood tests, MRI scans, and baseline and 1-year follow-up cognitive function assessments.
Cohort 2 were part of the China Longitudinal Aging Study (CLAS) that was initiated in 2012. The CLAS was a multicentre study, and we selected participants from Shanghai. All participants received a clinical examination and cognitive function assessments at baseline and follow-ups; some also received blood tests and MRI scans at the same time periods.
There were 197 older adults with MCI met the inclusion criteria of MCI as follows: (1) age ≥60 years; (2) both the affected individual and their informants reported the memory loss; (3) cognitive decline—Montreal Cognitive Assessment (MoCA) scale score <23 for individuals with >12 years of education, MoCA score <21 for 7–12 years of education, MoCA score <19 for ≤6 years of education and MoCA score <13 for no formal education; (4) normal ability to carry out daily living activities; and (5) able to cooperate and complete relevant assessments. The exclusion criteria for participants with MCI were as follows: (1) unstable cognitive function at follow-up—the MCI status had progressed to AD as confirmed by specialised physicians or the cognitive function had returned to normal; and (2) auditory-visual impairments affecting study participation, depression or severe physical disease that could impact cognitive function.
There were 388 older adults with NC met the inclusion criteria of NC as follows: (1) age ≥60 years; (2) normal cognitive function as indicated by MoCA scores based on years of education: ≥23 for individuals with >12 years of education, ≥21 for 7–12 years of education, ≥19 for ≤6 years of education and ≥13 for no formal education; (3) normal ability to carry out daily living activities; and (4) able to cooperate and complete relevant examinations. The exclusion criteria for NC were as follows: (1) unstable cognitive function at follow-up, that is, the subject with NC progressed to MCI or AD; and (2) auditory-visual impairments affecting study participation, depression or severe physical disease that could impact cognitive function.
Study design and procedure
This study used a longitudinal case–control intervention study that was carried out from May 2019 to October 2020.
Propensity matching score (PMS) analysis was used to match the number of the intervention and control groups (1:1). When the match tolerance was 0.03, we found that age, sex and years of education were balanced between the groups. The operations for selecting the MCI and NC cohorts were similar. Finally, 84–84 intervention–control participants were selected for the elderly participants with NC and 43–43 intervention–control participants with MCI. In our study, the 84 participants with NC and the 43 with MCI in the intervention group received comprehensive cognitive health management with a 1-year follow-up. The control group consisted of 84 elderly individuals with NC and 43 with MCI who matched the gender, age, education level, MoCA scores and Geriatric Depression Scale (GDS) scores of the intervention group but did not receive comprehensive cognitive health management; they received a 1-year follow-up to assess the natural outcome of their cognitive function without the intervention. The above subjects’ baseline and 1-year follow-up data were retrieved from the database, including cohorts 1 and 2 (figure 1).
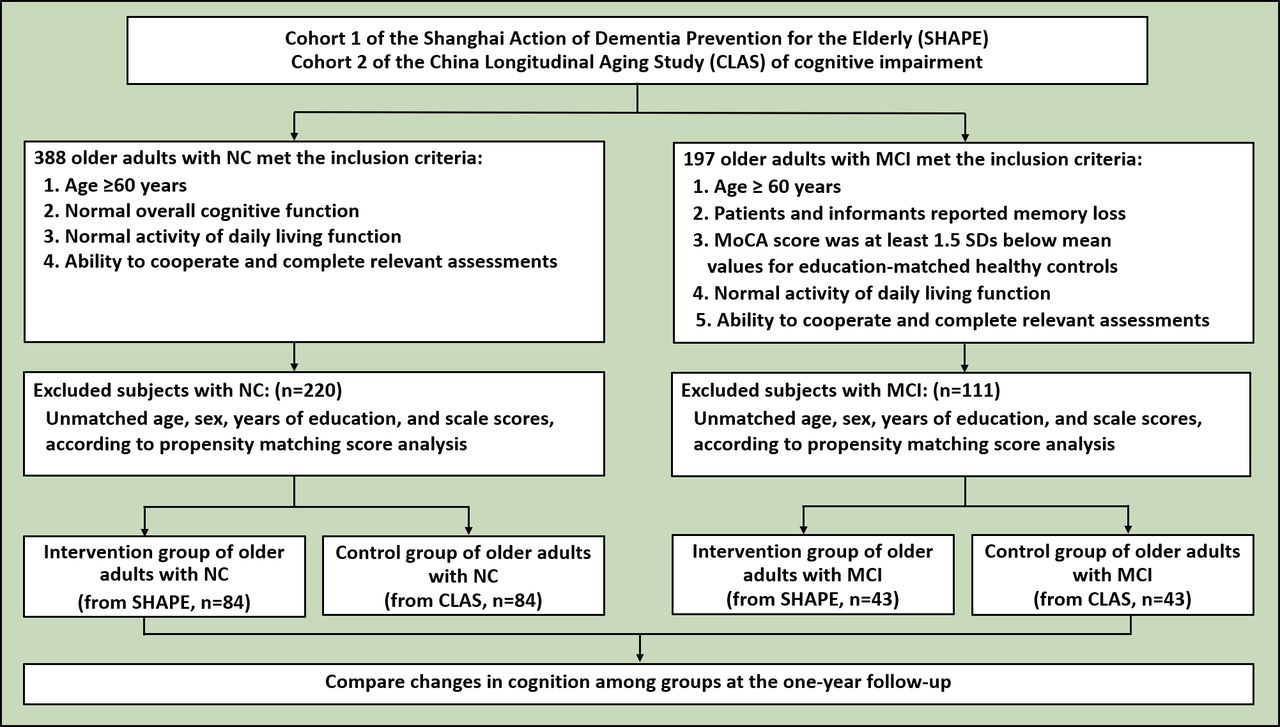
Research flowchart. MCI, mild cognitive impairment; MoCA, Montreal Cognitive Assessment; NC, normal cognition; SD, standard deviation.
The comprehensive cognitive health management was a 30-minute face-to-face psychiatrist-administered interview for participants in the intervention groups. It included informing participants of their cognitive risk based on the psychiatric assessment, providing individualised recommendations for improving their cognition, cognitive health coaching, follow-up and monitoring the implementation of recommendations.
The comprehensive brain health intervention included the following: (1) an explanation of the neuropsychological results from the cognitive function and depression assessment; (2) provision of brain health recommendations based on the individual’s lifestyle, clinical characteristics and biochemical blood tests: eat an appropriate diet, quit smoking and alcohol use, maintain a normal weight, take regular exercise, maintain normal social activities, improve sleep habits and learn new skills; and contact information for medical institutions; (3) health coaching to provide education to reduce the risk of AD by modifying the individual’s lifestyle and increasing awareness of self-management (precision education linking the associations between behaviour risk, lifestyle change and AD can be beneficial and motivating, especially for individuals with poor cognitive risk appraisal); (4) regular monthly phone call follow-up and monitoring by the psychiatrists who performed the baseline assessment, inquiring if the participants had remembered the previous suggestions and how well they were implementing them. At the 6-month follow-up conducted at our hospital, clinical characteristics and biochemical blood tests were examined and recorded. Clinical characteristics were mainly cognitive and emotion related. The laboratory tests included fasting blood glucose, triglycerides, cholesterol, high-density lipoprotein, low-density lipoprotein and blood cell components.
Research tools
All researchers underwent rigorous training and passed a conformance assessment. A professional psychiatrist made the diagnosis about cognitive status. The Beijing version of the MoCA was used to measure cognitive function.11–13 At the same time, we also used GDS to exclude participants with depression scores that were higher than 10.14 Activities of Daily Living, a scale consisting of 14 items of fundamental skills required to care for oneself,15 was used to measure independence in self-care. A score higher than 16 indicated varying degrees of functional abnormalities.
Statistical methods
We analysed data using SPSS (V.24.0) and R (V.4.0.2). The Kolmogorov-Smirnov test was used to test the normality of the distributions of continuous variables. We employed the t-test for continuous variables, the χ2 test for categorical variables, and the non-parametric Mann-Whitney test for non-normally distributed data comparing the intervention and control groups. The Wilcoxon signed-rank test was used to compare the baseline and 1-year follow-up values among the groups. To further verify the comprehensive health intervention efficacy variances in the different groups, the changing effects over time and control for the baseline differences in MoCA subscales, we conducted a generalised linear mixed model (GLMM) analysis with the lme4R package. MoCA total and subscale scores were selected as dependent variates, and fixed effects included group, follow-up, and group×follow-up. Variables that were statistically different between the two intervention and control groups at baseline (MCI: visual space; NC: visual space, naming and language) were corrected.
Results
Comparison of general data and scales at baseline between the intervention groups and the control groups
Among the elderly participants with NC and MCI, the intervention and control groups had no significant differences in gender, age, education, MoCA scores and GDS scores. However, in the MoCA subscales, there was a slight difference in the visual space and execution, naming, and language functions in the NC groups and in the visual space and execution function in the MCI groups (table 1).
Comparison of demographic data and baseline scores between older adults with NC and MCI at baseline
The impact of comprehensive cognitive health management on the cognitive function of elderly individuals with NC and MCI
At the 1-year follow-up, no significant difference was found in the MoCA total scores of the intervention and control groups among the older adults with NC (Z=−0.312, p=0.755). For the MoCA subscales, the visual space and execution and the abstract functions in the intervention group were slightly higher than in the control group (visual space, 4.57 (0.749) vs 4.17 (1.149), Z=2.584, p=0.010; and abstract, 1.65 (0.570) vs 1.27 (0.700), Z=3.800, p<0.001). The remaining subscales did not significantly differ between the two groups. In addition, the two groups had no significant difference in the total GDS scores (table 2).
Comparison of scores at the 1-year follow-up between older adults with normal cognition (NC) and mild cognitive impairment (MCI)
At the 1-year follow-up, the MoCA total scores of the intervention group were significantly higher than the control group among the elderly individuals with MCI (24.07 (3.674) vs 21.40 (4.826), Z=2.449, p=0.014). For the MoCA subscales, the naming, attention, delayed recall and orientation functions were slightly higher in the intervention group than in the control group (naming, 2.47 (0.702) vs 2.14 (0.743), Z=3.323, p=0.001; attention, 5.40 (1.003) vs 4.79 (1.407), Z=2.242, p=0.025; delayed recall, 2.84 (1.703) vs 2.05 (1.731), Z=2.625, p=0.009; and orientation, 5.79 (0.559) vs 5.58 (1.029), Z=2.093, p=0.036); the other subscales did not significantly differ (table 2).
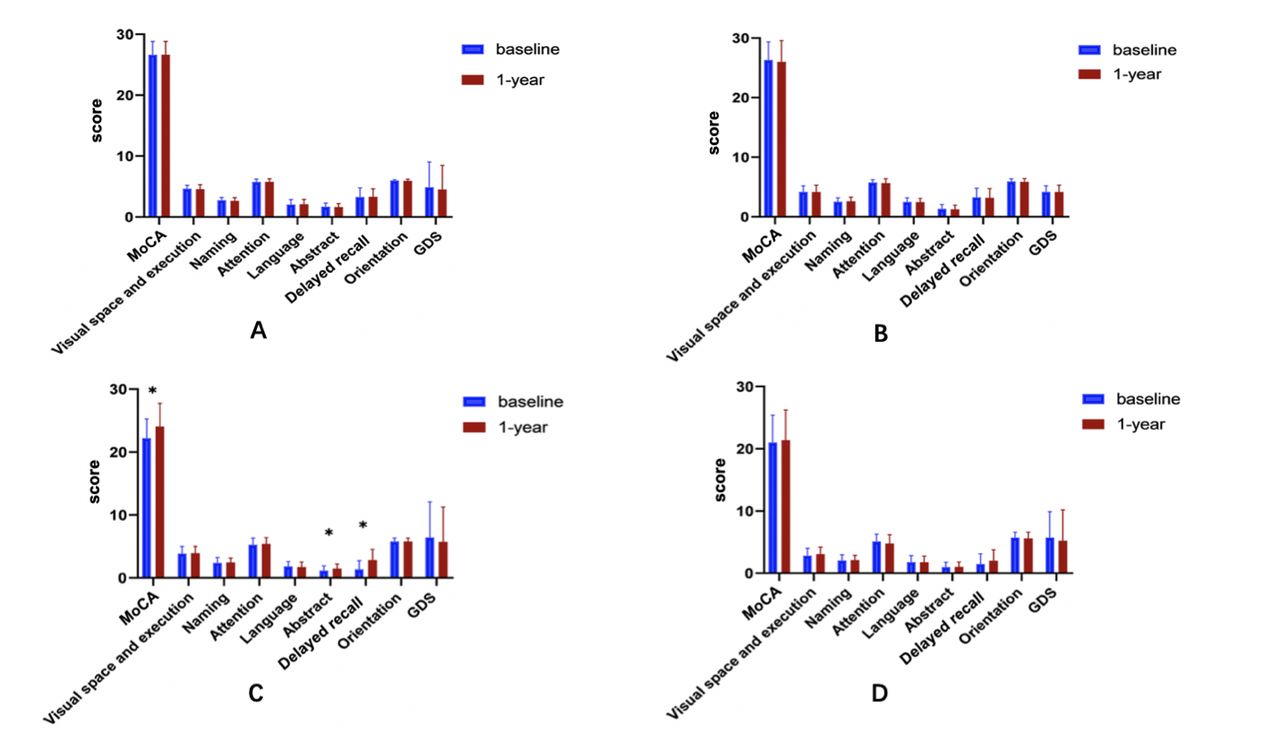
For the elderly individuals with NC, whether in the intervention group or the control group, no significant difference was found between the baseline and the 1-year follow-up MoCA total and subscale scores (figure 2A,B and online supplemental table 1).
Supplemental material
{kind=link}
{kind=link}
Comparison of MoCA and its subscales at baseline and 1-year follow-up. (A) Intervention group of older adults with NC; (B) Control group of older adults with NC; (C) Intervention group of older adults with MCI; (D) Control group of older adults with MCI. *p<0.05. GDS, geriatric depression scale; MCI, mild cognitive impairment; MoCA, montreal cognitive assessment; NC, normal cognition.
The elderly individuals with MCI showed differing characteristics. The participants with MCI in the intervention group had higher MoCA scale scores at the 1-year follow-up than at baseline (p=0.002). For the MoCA subscales, abstract and delayed recall function scores increased significantly from baseline to the 1-year follow-up (abstract, 1.16 (0.746) vs 1.47 (0.735), p=0.038; and delayed memory, 1.33 (1.429) vs 2.84 (1.703), p<0.001); the remaining 1-year follow-up subscale scores did not statistically differ from baseline (figure 2C and online supplemental table 1). These differences were not observed in the control group (figure 2D and online supplemental table 1).
A GLMM analysis in targeting the MoCA total and delayed recall function scores of the older adults with MCI showed that the interaction effects of group×follow-up were significant. The coefficients of the fixed-effects model showed that the MoCA scores of the treatment group and the control group changed differently over time. For each unit increase in time, the MoCA scores in the intervention group increased by 5.83 points compared with that in the control group in the elderly with MCI, and the increase was statistically significant (p<0.001). The subscale of the delayed recall score increased by 0.47 (p=0.02). At the same time, the differences between the intervention and control groups were not significant in the elderly participants with NC (tables 3 and 4 and online supplemental table 2).
Supplemental material
GLMM analysis of older adults with MCI in the MoCA score
GLMM analysis of older adults with MCI in the MoCA subscale delayed recall score
The emotional effect of comprehensive cognitive health management on elderly individuals with NC and MCI
Compared with baseline, the 1-year follow-up after the comprehensive cognitive health management showed decreased GDS scores for both the NC and MCI intervention groups (4.88 (4.164) vs 4.50 (3.971), p=0.443; and 6.44 (5.654) vs 5.74 (5.512), p=0.054, respectively). However, these differences were not statistically significant (figure 2A,C).
Discussion
Main findings
Our study aimed to investigate the effect of comprehensive cognition health management, a non-pharmacological intervention focusing on cognitive function in older adults with NC and MCI. Comprehensive cognitive health management included informing participants of their cognitive risk based on the psychiatric assessment, providing individualised recommendations for improving their cognition, and encouraging and monitoring the implementation of the recommendations during follow-up. This study was a retrospective case–control study. Participants from two cohorts underwent comprehensive cognitive health management and were followed for 1 year. The PMS analysis method was applied to match intervention and control groups, including the main factors related to cognitive function, such as age, gender and education.
There were four main findings from our study. First, at the 1-year follow-up of older adults with NC, no significant differences were found between the intervention and control groups in MoCA total scores and GDS scores. However, the subscale scores of MoCA (visual space and execution, and the abstract functions) were significantly higher in the intervention group than in the control group in the elderly with NC. Second, at the 1-year follow-up of older adults with MCI, the intervention group’s MoCA total scores and the naming, attention, delayed recall, and orientation subscale scores were significantly higher than the control group’s. Third, compared with baseline scores, the elderly participants with MCI in the intervention group scored significantly better on the overall MoCA and the abstract and delayed recall subscales at the 1-year follow-up. In contrast, the control group did not show any significant improvements. Finally, the GLMM analysis showed that the interaction effect of the group×follow-up was significant in the MoCA total and delayed recall subscale scores for the older adults with MCI.
The results of this study indicate some positive effects of comprehensive cognitive health management on the cognitive function of elderly individuals with MCI. After a 1-year follow-up, overall cognitive function, as well as abstract and delayed recall functions, was slightly improved in the intervention group. Coefficient estimation of fixed effects in GLMM analysis showed that MoCA total scores in the intervention group increased by 5.83 after 1 year compared with scores in the control group in the elderly individuals with MCI, and the delayed recall score increased by 0.47 in the intervention group. The comprehensive cognitive health management method emphasised the importance of brain health in the daily life of individuals with MCI by encouraging self-empowerment and cognitive health awareness for patients and their families. Individualised health recommendations were based on a brain health assessment of each participant. They included interventions for diet, exercise, sleep and emotional health so those affected with MCI and their family members could improve their self-management capabilities. Furthermore, the contact information of the medical staff carrying out the intervention and hospitals specialising in diagnosing and treating cognitive impairments was made available to facilitate help-seeking efforts.
Comprehensive cognitive health management can be defined as an attitude-changing, motivational boost to maintain and improve one’s cognitive function through self-care. It purports that individuals with high self-management skills are more likely to take steps to slow the disease progression.16 17 In addition, brain health education for patients and their caregivers can effectively improve awareness and knowledge of signs and early symptoms of cognitive disorders and thus increase screening and prevention rates.18At the same time, we encouraged cooperation between the community general practitioners (GPs) and the psychiatrists of our hospital. The GPs offered psychiatrists guidance about the patients’ daily life functions and chronic comorbidity needs, while the psychiatrists offered GPs the neuropsychological assessment results of the participants’ cognitive outcomes and risks via an online management system. This mutual professional exchange enhanced patient interventions; we hope this cooperation can be sustained and even extended in the future.
This preliminary study was the first to demonstrate an easy-to-implement strategy in the community for controlling the modifiable risk factors of cognition for elderly individuals with MCI. Comprehensive cognitive health management integrated multiple interventions for controllable risk factors, which differed from previous studies targeting a single factor. Experts suggested that modifying 12 risk factors might prevent or delay up to 40% of dementias.19–21 At the same time, it could vastly improve the living and dying circumstances of individuals with dementia, their families and thus society.22 23 Previous studies on drug intervention for elderly individuals with MCI have shown that cholinesterase inhibitors, including donepezil and galantamine, antioxidants such as vitamin E and anti-inflammatory drugs such as rofecoxib cannot prevent the progression of MCI to dementia.24–28 In terms of nutritional intervention, some experimental intervention results showed that supplementation of folic acid or multivitamins has no practical effect on maintaining and improving cognitive function.29–32 On the other hand, studies have found that non-drug cognitive interventions, such as physical exercise and social activities, have a particular effect on delaying the progression of MCI to dementia.33–35 Our results suggest that an intervention with a complete list of combined recommendations is effective. Still, we cannot be sure which of them was decisive in producing the favourable outcome.
Limitations
This article had certain limitations. First of all, this study was a retrospective cohort study. Therefore, cognitive changes may be related to changes in family members, the living environment or physical health, inevitable confounding factors in retrospective studies. The conclusions drawn in this article about the effectiveness of the comprehensive cognitive health intervention could be further strengthened in randomised controlled trials. Second, the participants in this study came from middle-income communities in Shanghai; thus, similar studies should be promoted and vetted in areas with different economic and medical access levels. Third, the effectiveness of comprehensive cognitive health management might be related to the availability of skilled and responsible interventionists and regular follow-up. Finally, the methods of comprehensive health intervention need to be further refined to form a definitive guide. The components we included in our intervention are worth noting in the next step to promote comprehensive cognitive health management research.
Implications
According to these findings, the community-dwelling elderly individuals with MCI may have improved their cognitive function following a 1-year comprehensive cognitive health management intervention. Therefore, daily comprehensive cognitive health management is a potential method for improving cognitive function in community older adults with MCI. More importantly, this approach was feasible and widely available in the communities where professional psychiatrists participate in routine cognitive screening.
Data availability statement
No data are available. No additional data are available.
Ethics statements
Patient consent for publication
Ethics approval
The Ethics Committee of Shanghai Mental Health Center approved the study protocol (2019-70C1), and the study was carried out according to the tenets of the Declaration of Helsinki. After we described the study, we obtained written informed consent from all subjects.
References
Jiayuan Qiu obtained a bachelor's degree from Southern Medical University in 2018. In the same year, he began his postgraduate studies in the Department of Geriatrics at the Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine. He majors in psychiatry and his research interests include cognitive and emotional disorders of the elderly.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JQ and LZ are joint first authors.
JQ and LZ contributed equally.
Contributors JQ and LZ contributed equally to this paper. XL, YF and MS shared joint correspondence in this work. JQ and LZ performed statistical analysis and drafted the manuscript text. XL and YF designed the study and MS helped the validation in follow-up and community popularisation. SX, SZ, LL, JN, LB, SQ and YY collected the data and MP provided key comments. XL was the guarantor and supervised the data collection, statistical analysis, and modified the paper. All authors approved the final version of the manuscript.
Funding This study was funded by Fifth Three-year Action Plans for Public Health (grant number: GWV-9.2); Youth Scientific Research Project of Shanghai Municipal Commission of Health and Family Planning (grant number: 20184Y0298); Project of advanced and appropriate technology from Shanghai Municipal Health Commission (grant number: 2019SY045) and National Key R&D Program of China (grant number: 2017YFC1310501).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.