Article Text

Abstract
Background Self-reflectiveness, one dimension of cognitive insight, plays a protective role in an individual’s mental state. Both high and low levels of self-reflectiveness have been reported in patients with schizophrenia and individuals at clinical high risk for the illness.
Aims This study aimed to explore the relationship patterns between self-reflectiveness and clinical symptoms in individuals during the pre-morbid and early clinical stages of psychosis.
Methods A total of 181 subjects, including individuals with attenuated positive symptoms (APS, n=122) and patients with first-episode psychosis (FEP, n=59), completed the Beck Cognitive Insight Scale and were evaluated using the Schedule of Assessment of Insight and Positive and Negative Syndrome Scale. All subjects were classified into three groups according to their level of self-reflectiveness: low level (LSR, n=59), medium level (MSR, n=67) and high level (HSR, n=55). Both linear and non-linear relationships between self-reflectiveness and clinical symptoms were explored.
Results More individuals with APS were classified into the MSR group, while more patients with FEP were classified into the LSR group. The LSR group demonstrated less awareness of illness than the MSR and HSR groups, more stereotyped thinking and poorer impulse control but less anxiety than the MSR group, and lower levels of blunted affect and guilt feelings than the HSR group. The MSR group demonstrated lower stereotyped thinking than the HSR group. Compared to the LSR group, the MSR group had increased self-reflectiveness, improved awareness of illness, decreased stereotyped thinking, and better impulse control, but increased feelings of guilt. The HSR group showed increased stereotyped thinking when compared to the MSR group, but the other variables did not change significantly between these two groups. Overall, self-reflectiveness demonstrated an approximately inverse S-shaped relationship with the awareness of illness, a U-shaped relationship with stereotyped thinking and poor impulse control, and an almost linear relationship with anxiety and guilt feelings.
Conclusions Self-reflectiveness demonstrates complex relationships with clinical symptoms and fails to exert significant positive effects when reaching a certain high level.
- schizophrenia spectrum and other psychotic disorders
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Self-reflectiveness, one dimension of cognitive insight, is a protective factor. However, patients with schizophrenia and individuals at clinical high risk for the illness do not always have lower levels of self-reflectiveness than normal subjects.
WHAT THIS STUDY ADDS
This study indicates that there may be a balance point in the protective effect of self-reflectiveness. When it reaches a certain level, its protective effect may be offset by other factors.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We can conclude that it is necessary to comprehensively evaluate and pay attention to psychological states when implementing interventions targeting cognitive insight.
Introduction
Self-reflectiveness refers to an individual’s capacity and willingness to consider alternative explanations of their own thoughts and constitutes one dimension of cognitive insight, as measured by the Beck Cognitive Insight Scale (BCIS).1 A high level of self-reflectiveness was not only associated with good clinical insight,1 2 including awareness of illness, relabelling of specific symptoms, and treatment compliance, but also with increased depressive symptomatology.3 4 In addition, we found that self-reflectiveness had potential positive correlations with negative symptoms in individuals with attenuated psychotic symptoms (APS)--one type of clinical high risk for psychosis (CHR)--when the duration of untreated APS was longer than 12 months.5 Previous studies consistently demonstrated the paradox of self-reflectiveness, emerging not only in patients with schizophrenia spectrum disorders6 7 but also in individuals with subclinical psychosis.8 However, García-Mieres et al3 showed that the association between higher self-reflectiveness and increased depression was meaningful because self-reflectiveness can moderate the relationship between depressive symptoms and general psychological distress. Moreover, self-reflectiveness presented a predictive role in prospective symptom outcomes.9 10 In a 4-year follow-up study, O’Connor et al10 found that self-reflectiveness was an independent predictor for prospective symptom severity in psychosis.
However, there are many inconsistent conclusions about the differences between groups. Some studies found that patients with psychosis reported lower self-reflectiveness than the non-psychiatric sample.11 12 Conversely, some studies failed to reveal any differences between psychotic patients and non-psychiatric subjects.13 14 Additionally, inconsistent findings have been reported in patients with schizophrenia with varying symptoms. For example, Warman et al14 reported that psychotic individuals without delusions showed lower levels of self-reflectiveness than individuals with delusions and healthy control (HC) subjects, with the latter two groups demonstrating no significant differences. However, Engh et al15 reported that the occurrence of delusions is associated with low self-reflectiveness, while patients with only hallucinations demonstrated high self-reflectiveness. Moreover, inconsistent results have also been reported in CHR individuals. Kimhy et al16 reported that patients with schizophrenia scored significantly higher on self-reflectiveness than CHR and HC subjects, the latter two groups demonstrating no significant difference. Other studies also reported no significant difference in self-reflectiveness between CHR and HC groups.17 18 However, Clark19 found that self-reflectiveness was significantly higher in CHR individuals than in HC subjects. Our previous study found that CHR individuals demonstrated poorer cognitive insight, with lower scores on self-reflectiveness than HC subjects.5
The inconsistent results may be associated with multiple factors, such as different sample compositions, but we proposed the complex relationship between self-reflectiveness and symptoms3 as another possibility. For example, when subjects had high levels of depression, anxiety, or negative symptoms, the level of self-reflectiveness may also be high.4 5 These relationships may have clinical implications, such as alleviating general psychological distress.3 However, whether the relationship between self-reflectiveness and depression, anxiety, or negative symptoms is linear or non-linear has not yet been reported. We hypothesised that there may be a balance point of self-reflectiveness that exerts positive effects on clinical symptoms: when below the balance point, the positive effects may increase as self-reflectiveness improves; but after reaching the balance point, the positive effects may be compromised because of the complex relationship between self-reflectiveness and symptoms. In other words, self-reflectiveness may demonstrate non-linear relationships with clinical symptoms.
García-Mieres et al3 analysed the effect of depressive symptoms on general psychological distress among three groups with low, medium, and high levels of self-reflectiveness. Building on their study and our hypothesis, we divided the subjects in this study into three groups according to the quartile of self-reflectiveness: low, medium, and high self-reflectiveness groups. This study aimed to observe the distribution of attenuated psychotic symptoms (APS) and first-episode psychosis (FEP) in subjects and the differences in clinical characteristics among the three groups and to analyse the relationship patterns between self-reflectiveness and clinical symptoms.
Methods
Procedure
This study was conducted at the Shanghai Mental Health Center and its affiliate, the Shanghai Psychotherapy and Psychological Counselling Center, with the recruitment of subjects from February 2019 to May 2021. The inclusion criteria for participants were individuals with APS or patients with FEP aged between 11 and 45 years who had completed at least 6 years of primary education. The exclusion criteria included a history of psychotic disorder, severe somatic diseases, mental retardation (intelligence quotient (IQ)<70), dementia, ingestion of antipsychotic medication for more than 2 weeks, and the exhibition of positive symptoms induced by other mental disorders or psychoactive substances. The study was carried out according to the tenets of the Declaration of Helsinki. All the participants, as well as the next of kin or legal guardian for those younger than 18 years, signed written informed consent forms.
Participants
The study enrolled 185 subjects who had been referred by psychiatrists to the Shanghai At Risk for Psychosis-extended (SHARP-extended) programme. They were preliminarily screened and interviewed by trained raters using the general interview section of the Structured Interview for Psychosis-risk Syndromes (SIPS). They were also assessed with the five positive symptom items of the Scale of Psychotic-risk Syndromes (SOPS) and the Global Assessment of Functioning (GAF) Scale. Four enrollees were excluded, three because of taking antipsychotic medications for longer than two weeks, and one for bipolar disorder symptoms. One hundred and twenty-two subjects met the criteria of APS with or without the genetic risk and deterioration syndrome, and 59 subjects met the criteria for FEP with the presence of psychotic symptoms. The APS and FEP groups were combined for the analysis. All participants were classified into three groups according to the quartile of self-reflectiveness: low level (≤11 scores of self-reflectiveness, LSR, n=59); medium level (12–16 scores of self-reflectiveness, MSR, n=67) and high level (≥17 scores of self-reflectiveness, HSR, n=55). See the flowchart of subject recruitment in figure 1.
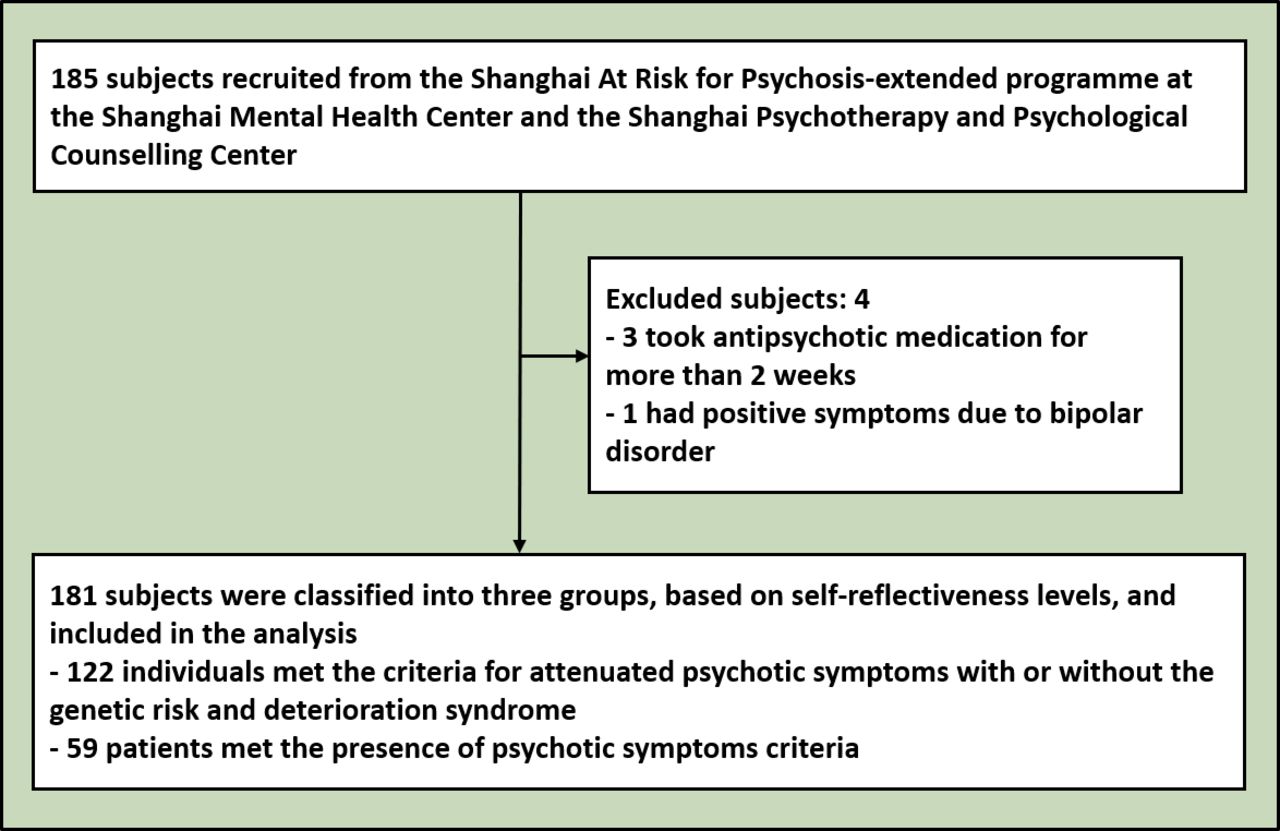
Flowchart of participants recruitment.
Measures
Self-reflectiveness and clinical insight
Self-reflectiveness was measured using nine items of the Beck Cognitive Insight Scale (BCIS),1 which is a self-report questionnaire with 15 items and two subscales. Participants were asked to rate their degree of agreement with the statement for each item on a 4-point scale, from ‘strongly disagree’ to ‘strongly agree’. The Chinese version of the BCIS has acceptable reliability and validity, and the Cronbach’s alpha coefficient of the self-reflectiveness subscale is 0.7.20 Clinical insight was measured using the Chinese version of Schedule of Assessment of Insight (SAI),21 which is a semi-structured interview tool including seven items, with a total score of 14 (0–6 for awareness of illness, 0–4 for relabelling of specific symptoms, and 0–4 for treatment compliance).
Psychopathological symptoms
SIPS is a structured interview tool including a general interview, family history of mental illness, the SOPS and GAF scales, and criteria for schizotypal personality. We used this tool to rule out prior psychotic episodes and identify individuals with APS and patients with current psychotic episodes. The Positive and Negative Syndrome Scale (PANSS) was used to assess the participants’ psychopathological symptoms. Shafer and Dazzi22 conducted a meta-analysis on factor analyses of the PANSS and proposed five factors, including positive symptoms, negative symptoms, disorganisation, affect, and resistance. The Chinese version of PANSS has good reliability and validity.23
Statistical analysis
SPSS V26.0 was used to conduct the analysis. A one-way analysis of variance (ANOVA) was conducted to compare demographic continuum variables among the LSR, MSR, and HSR groups. A χ2 test was conducted to compare the differences in the proportions of categorical variables among different groups. Adjusted standardised residuals (ASR) were calculated for contingency tables to analyse the contribution of different cells to the significance of the χ2 test. For ASR>1.96, statistical significance was set at p<0.05 and, for ASR>2.58, at p<0.01. Multivariate analysis of covariance (MANCOVA) was used to compare clinical variables controlling for covariates. Multiple comparisons were adjusted using Bonferroni’s method. Binary logistic regression analysis was conducted to differentiate among the LSR, MSR, and HSR groups. Receiver operating characteristic (ROC) analysis was conducted, and the area under the curve (AUC) was calculated. Linear relationships in each group and non-linear relationships in total sample of self-reflectiveness with clinical insight and clinical symptoms were explored using linear and non-linear regression analysis. The level of significance was set at 0.05 (two-tailed).
Results
Demographics and clinical characteristics
The one-way ANOVA revealed significant differences in the father's education among subjects with different levels of self-reflectiveness (F=4.662, p=0.011). The post hoc analysis (Bonferroni correction) showed that the father's education in the LSR group was significantly lower than in the MSR group (p=0.008). APS individuals and patients with FEP were distributed differently in low and medium levels of self-reflectiveness (χ2=7.904, p=0.019). A larger proportion of APS individuals were distributed in the MSR group (ASR=2.2, p<0.05), while a larger proportion of patients with FEP were distributed in the LSR group (ASR=2.6, p<0.01) (see table 1).
Comparison of demographic and clinical characteristics
The categorical variable of diagnoses (APS and FEP) was transformed into a dummy variable (APS=0, FEP=1) and then added into the covariates, along with age, education and gender, when MANCOVA was conducted. The results showed a significant main effect of groups on each dimension of clinical insight (p<0.05). Pairwise comparisons adjusted using the Bonferroni method revealed that compared to the MSR and HSR groups, the LSR group had poorer awareness of illness (p=0.002, p=0.021, respectively) and poorer total clinical insight (p<0.001, p=0.026, respectively). The MSR and HSR groups demonstrated no significant differences in clinical insight. In terms of relabelling of specific symptoms and treatment compliance, the LSR group scored lower than the MSR group (p=0.008, p=0.011, respectively).
Comparison of the five PANSS factors among the groups
Controlling for age, education, gender and diagnoses, MANCOVA revealed that there were significant main effects (p<0.05) of groups on the factors of disorganisation, affect, and resistance, and the items of N1 (blunted affect), N5 (difficulty in abstract thinking), N7 (stereotyped thinking), G13 (disturbance of volition), G2 (anxiety), G3 (guilt feelings), and G14 (poor impulse control) (see table 2). Multiple comparisons adjusted using the Bonferroni method revealed that compared to the MSR group, the LSR group got higher scores on stereotyped thinking (p=0.043), poor impulse control (p=0.020), and the resistance factor (p=0.019); however, compared to the HSR group, the LSR group got lower scores on blunted affect (p=0.037) and disturbance of volition (p=0.020). Compared to the MSR and HSR groups, the LSR group also had lower scores on anxiety (p=0.017, p=0.006, respectively), guilt feelings (p=0.028, p=0.003, respectively), and the affect factor (p=0.019, p=0.006, respectively). The MSR and HSR groups had no significant differences. In addition, the MSR group showed a lower score on stereotyped thinking than the HSR group (p=0.039), demonstrating no significant difference with the LSR group.
Comparison of the five PANSS factors among groups (multivariate analysis of covariance)
Binary logistic regression analysis for differentiating different groups
LSR vs MSR
Binary logistic regression analysis, controlling for age, education, gender and diagnoses revealed that awareness of illness, stereotyped thinking, anxiety, and poor impulse control entered the model for differentiating between the LSR and MSR groups (omnibus tests of model coefficients: χ2=36.727, p<0.001) (see figure 2A). Higher levels of stereotyped thinking and poor impulse control were associated with lower levels of self-reflectiveness. However, individuals with lower levels of self-reflectiveness demonstrated lower levels of anxiety. As expected, self-reflectiveness was positively associated with awareness of illness. ROC analysis showed that the model differentiated between the LSR and MSR groups by 79.9% AUC (95% CI: 0.722 to 0.876).
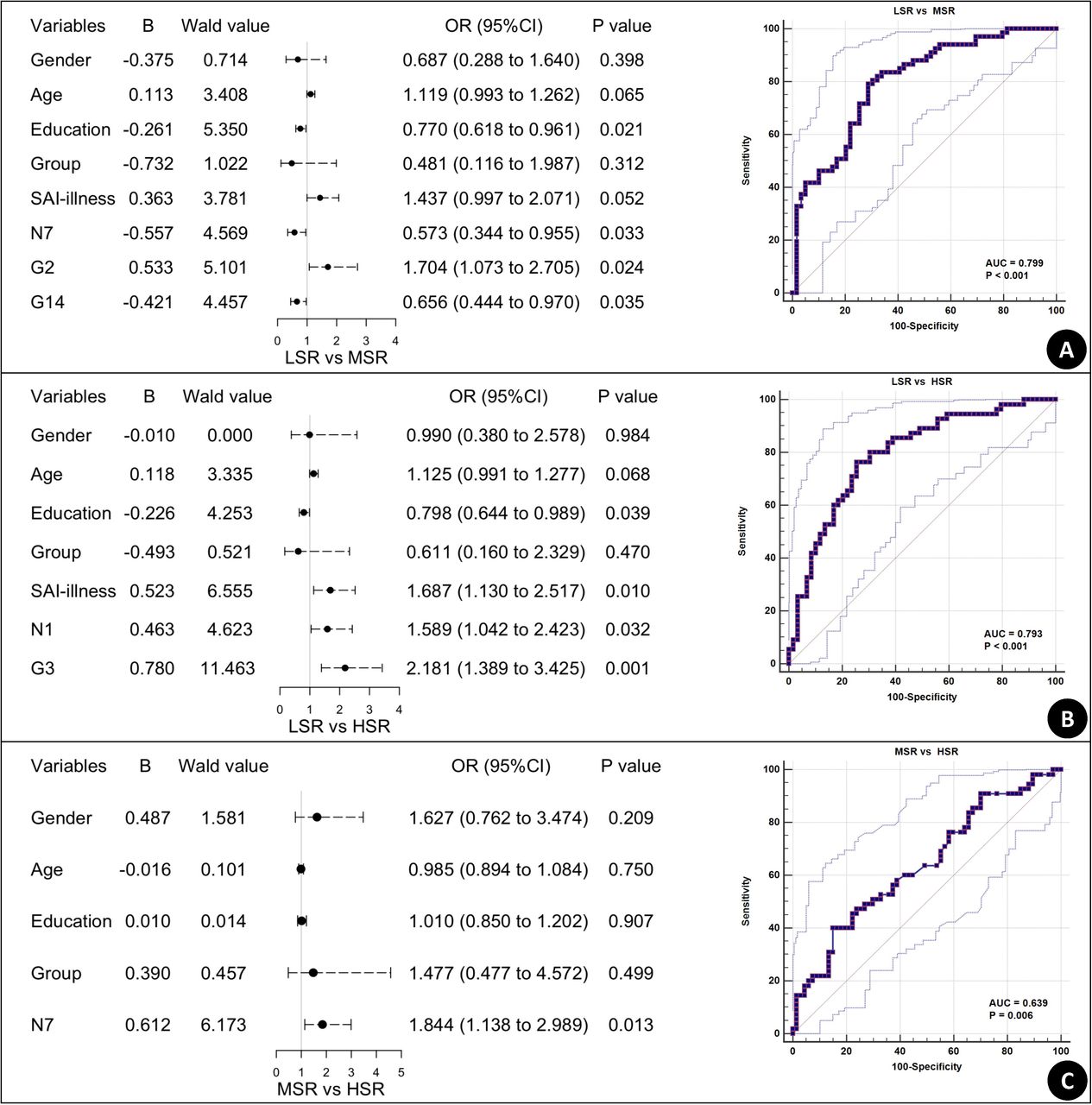
Forest plot and receiver operating characteristic curve of binary logistic regression differentiating individuals with different levels of self-reflectiveness. LSR, low scores on self-reflectiveness; MSR, medium scores on self-reflectiveness; HSR, high scores on self-reflectiveness; N1, blunted affect; N7, stereotyped thinking; G2, anxiety; G3, guilt feelings; G14, poor impulse control; SAI, Schedule of Assessment of Insight.
LSR vs HSR
Awareness of illness, blunted affect, and guilt feelings entered the model when differentiating between the LSR and HSR groups (omnibus tests of model coefficients: χ2=32.811, p<0.001) (see figure 2B). Self-reflectiveness was still positively associated with awareness of illness. However, with the increase in self-reflectiveness, blunted affect and guilt feelings also increased correspondingly. The ROC analysis showed that the model differentiated between the LSR and HSR groups by 79.3% AUC (95% CI: 0.710 to 0.876).
MSR vs HSR
Only stereotyped thinking entered the model for differentiating between the MSR and HSR groups (omnibus tests of model coefficients: χ2=8.840, p=0.116) (see figure 2C). However, in contrast with the model for differentiating between the LSR and MSR groups, a higher level of stereotyped thinking here was associated with a higher level of self-reflectiveness. In other words, a lower or higher level of self-reflectiveness is closely associated with stereotyped thinking. The ROC analysis showed that the model differentiated between the MSR and HSR groups by 63.9% AUC (95% CI: 0.540 to 0.738).
Non-linear relationship between self-reflectiveness and symptoms
Linear and non-linear regression analysis were conducted to explore the linear relationships in each group and non-linear relationships in the total sample of self-reflectiveness with awareness of illness, blunted affect, stereotyped thinking, anxiety, guilt feelings, and poor impulse control (see figure 3). From the low to medium level of self-reflectiveness, the trend line for each clinical variable was relatively consistent, although it did not reach the significance level for some variables at a low or medium level. However, at a high level, all variables reached a relative plateau, except for stereotyped thinking (which was opposite to the previous direction and elevated (F=3.748, p=0.058)) and blunted affect (which was slightly raised (F=1.248, p=0.269)). Although a significant difference in blunted affect existed between the LSR and HSR groups, the linear regression in each group and the non-linear regression in the total sample did not reach the level of significance (p>0.05). In the non-linear regression with statistical significance, the relationships of self-reflectiveness with anxiety and guilt feeling tended to be straight; the relationships of self-reflectiveness with stereotyped thinking and poor impulse control tended to be U-shaped; and the relationship of self-reflectiveness with awareness of illness tended to be inverse S-shaped.

{kind=link}
{kind=link}
{kind=link}
Non-linear relationship between self-reflectiveness and clinical symptoms. LSR, low scores on self-reflectiveness; MSR, medium scores on self-reflectiveness; HSR, high scores on self-reflectiveness; total, the total sample; N1, blunted affect; N7, stereotyped thinking; G2, anxiety; G3, guilt feelings; G14, poor impulse control; SAI, Schedule of Assessment of Insight. Quadratic curve fitting revealed significant non-linear relationships of self-reflectiveness with stereotyped thinking (y=0.0152×2-0.4365x+4.8885), anxiety (y=−0.0055x2+0.2127x+1.1379), guilt feelings (y=−0.0047x2+0.2058x+0.1188), and poor impulse control (y=0.0105×2-0.3312x+4.6292); quartic curve fitting revealed a significant non-linear relationship between self-reflectiveness and awareness of illness (y=0.0001×4-0.0068x3+0.1125x2-0.3833x+1.3655).
Discussion
Main findings
Based on the self-reflectiveness paradox and the inconsistent results among different groups reported in previous studies, we examined whether self-reflectiveness presents non-linear relationships with clinical symptoms. The results showed that awareness of illness improved with the increase of self-reflectiveness from the low to medium level but reached a plateau when self-reflectiveness reached a high level. Anxiety and guilt feelings generally decreased with the increase of self-reflectiveness, although they demonstrated a plateau or decreased slightly at a high level of self-reflectiveness. Stereotyped thinking and poor impulse control decreased with the increase of self-reflectiveness from a low to medium level but demonstrated a reverse increase at a high level of self-reflectiveness, especially stereotyped thinking which showed a marked rise.
Regarding the differences in self-reflectiveness between APS individuals and patients with FEP, this study found the two categories of subjects distributed differently among the low, medium, and high levels of self-reflectiveness, demonstrating that APS individuals accounted for more subjects in the MSR group, while patients with FEP accounted for more subjects in the LSR group. There was no difference in the proportion of subjects in the HSR group between the two categories. This result indicates that a medium level of self-reflectiveness may be desirable, while low and high levels of self-reflectiveness may have different negative effects. Compared with patients with FEP, APS individuals not only had milder symptoms but also exhibited less functional impairment,24 and even remained relatively intact in some aspects of their functionality.25
Previous studies consistently reported that self-reflectiveness was closely related to clinical insight26 27 and emotional symptoms, such as depression and anxiety,3 6 which was further reinforced by this study. However, although there were significant differences in each dimension of clinical insight among the three levels of self-reflectiveness, logistic regression analysis revealed that only awareness of illness entered the regression model for distinguishing the LSR from the MSR and HSR groups. The results indicate that self-reflectiveness may play an indirect role in relabeling specific symptoms and treatment compliance through awareness of illness. Lui et al26 proposed that cognitive insight complements clinical insight in affecting medication adherence in patients with schizophrenia. In addition, we found that anxiety, guilt feelings, and clinical insight, as well as blunted affect, entered the regression model for differentiating the LSR from the MSR or HSR groups. Our previous study also found that self-reflectiveness positively correlated with negative symptoms.28 However, this study further selected self-reflectiveness as the independent variable and blunted affect as the dependent variable to conduct regression analysis and found that it did not reach significance. Blunted affect refers to diminished emotional responsiveness, characterised by a reduction in facial expression, modulation of feelings, and communicative gestures. Jeganathan and Breakspear29 proposed a computational framework for emotional expression based on active inference and stated that blunted affect derives from uncertainty about whether one’s emotional expression is effective in responding to others’ affective responses. It is possible that blunted affect influenced self-reflectiveness. When a person has weak inferences about the validity of emotional responses, their self-reflectiveness might be reduced.
Stereotyped thinking and poor impulse control presented a U-shaped curve with self-reflectiveness. Poor impulse control refers to disordered regulation and control of action on inner urges, resulting in sudden, unmodulated, arbitrary, or misdirected discharge of tension and emotions without concern for consequences. Individuals with a low level of self-reflectiveness lack introspection and openness to external feedback,13 indicating that they may not be able to observe their own internal emotional impulses, while conversely lacking tolerance for external stimuli. They may, therefore, be more impulsive. However, it is difficult to understand that the HSR group also scored higher on poor impulse control, although there was no significant difference between the HSR and MSR groups. In addition, stereotyped thinking refers to decreased fluidity, spontaneity, and flexibility of thinking. The subjects may refuse to accept another idea or have difficulty in switching from one idea to another, which is understandable in the LSR group, but contrary to the concept of self-reflectiveness in the HSR group. García-Mieres et al3 reported that although self-reflectiveness was positively correlated with depression, it also reduced the degree of psychological distress associated with depressive mood. It remains to be investigated whether higher self-reflectiveness correlated with higher poor impulse control and whether stereotyped thinking has a special role to play as García-Mieres et al have reported.
Limitations
This study has several limitations. First, this study assumes a continuous spectrum from the varying severity of CHR to the first episode of psychotic symptoms, so we included both CHR and FEP to analyse the three groups at different levels of self-reflectiveness. Although the categorical variable of diagnoses was selected as a covariate in the statistical analysis, there may be qualitative differences between the CHR individuals and patients with FEP, therefore, the differences in different groups at different levels of self-reflectiveness can be further explored after the subsequent expansion of the sample size. Second, this study did not investigate psychological stress or distress associated with symptoms and so failed to further explore the regulatory role of self-reflectiveness demonstrating positive or U-shaped correlations with symptoms, as previous researchers have done. Third, the transition rate of APS individuals to psychosis at 24 months was reported to be 19%.30 Those who did not convert to psychosis may ultimately have a different diagnosis,31 such as mood disorders, and may score relatively high on self-reflectiveness.1 Stereotyped thinking and poor impulse control have been reported to be common and perhaps even more pronounced in mood disorders.32 Therefore, whether higher scores on these items in the HSR group are related to the final diagnosis needs to be clarified by further follow-up studies. The follow-up results of some subjects could not explain this issue because the information from the subjects in this study was not completely collected until May 2022.
Implications
In summary, self-reflectiveness is beneficial to the maintenance of clinical insight but may also have a positive linear correlation with anxiety and guilt feelings, which supports the notion of the self-reflectiveness paradox. Additionally, self-reflectiveness may present U-shaped relationships with stereotyped thinking and poor impulse control, meaning that moderate levels of self-reflectiveness may be more beneficial. Therefore, the U-shaped relationship between self-reflectiveness and some variables should be considered when the causal associations between self-reflectiveness and clinical symptoms are explored. Conversely, changes in some relevant clinical symptoms should be noted during interventions to improve self-reflectiveness.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Research Ethics Committee of the SMHC (No 2020-100) . Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Sincerely appreciate great support from participants and their families.
References
Lihua Xu obtained a master’s degree from Soochow University in China in 2011 and a PhD from Shanghai Jiao Tong University in China in 2017. She is currently an attending doctor and assistant researcher and has worked at the Electromagnetic brain imaging and Eye movement laboratory of Shanghai Mental Health Center (SMHC) since 2017. As a member of early identification and intervention for clinical high risk of psychosis in SHARP (Shanghai At Risk for Psychosis) team, she is mainly engaged in the study of biological markers for the transition into psychosis of individuals with clinical high-risk syndromes, including eye movement, electrophysiology, and neuroimaging.

Footnotes
Contributors LX wrote the first draft of manuscript and conducted the statistical analyses; HC, YW, ZQ, YW, HH and QG interviewed participants and organised the primary data; XT, YH and YT reviewed and revised the draft; TZ and JW designed the study and provided supervision in the implementation of the study; JW was responsible for the overall content as the guarantor. All authors have approved the final manuscript.
Funding This study was supported by the Ministry of Science and Technology of China, National Key R&D Program of China (2016YFC1306800); National Natural Science Foundation of China (81671332, 81971251, 81671329, 81871050, 81901832, 81971251, 82001406, 82101582, 82151314, and 82171497); Shanghai Municipal Science and Technology Major Project (2018SHZDZX01, 2018SHZDZX05) and ZJLab; Science and Technology Commission of Shanghai Municipality (16JC1420200, 16ZR1430500, 19410710800, 19411950800, 19411969100, 19441907800, 19ZR1445100, 19ZR1477800, 20ZR1448600, 21ZR1481500, and 21S31903100); Shanghai Municipal Health Commission (202040361); Project of the Key Discipline Construction, Shanghai 3-Year Public Health Action Plan (GWV-10.1-XK18); Shanghai Clinical Research Center for Mental Health (19MC1911100); Clinical Research Plan of SHDC (SHDC2020CR4066); Clinical Research Center at Shanghai Jiao Tong University School of Medicine (DLY201817, 20190102); Shanghai Jiao Tong University Foundation (ZH2018ZDB03, ZH2018QNB19), The Clinical Research Center at Shanghai Mental Health Center (CRC2018ZD01, CRC2018ZD04, CRC2018YB01, CRC2019ZD02, and 2020-FX-02), Shanghai Mental Health Center (2019-zd01).
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.