Article Text

Statistics from Altmetric.com
Introduction
Schizophrenia is a devastating mental disorder affecting 20 million people worldwide.1 Early diagnosis is crucial for disease management and improvement in prognosis, and diagnostic biomarkers can serve as objective indicators for the early screening of the disease. Based on the observation of diminished flush responses to niacin in patients with schizophrenia,2 Horrobin proposed a non-invasive niacin skin flush screening for schizophrenia.3
Methods like optical reflection spectroscopy4–6 or laser Doppler flowmetry7 8 are commonly used to evaluate niacin skin test results for diagnosis, but they heavily rely on medical instruments and thus, lack accessibility. Visual rating9–11 is a more accessible option, but it is subjective, easily affected by noise, and therefore less reliable.
Adopting artificial intelligence (AI) technologies for image recognition, we developed a more dependable and accessible diagnostic system based on the niacin skin test that can be used for first-episode schizophrenia (FES) screening. To implement our screening algorithm, we designed a portable device with data collection and processing features for FES screening that detects and evaluates the subject's degree of skin-flushing response to niacin.
Methods
Our study included 54 patients with FES, 48 individuals at clinical high risk (CHR) for developing psychosis, and 73 healthy controls (HCs). The device we designed is shown in figure 1. The subject’s forearm is placed on the arm tray while holding the crossbar (figure 1A). Then, aqueous methylnicotinate is applied simultaneously in four dilutions (0.1 M, 0.01 M, 0.001 M, and 0.0001 M) to the inner forearm skin using filter paper patches. The patches are removed after 60 seconds. Five minutes after the removal, the camera above the tray takes four photographs of the arm at 5-minute intervals with the fill lights turned on (figure 1B). This way, the photographs are collected from a fixed vertical view in a well-lit environment, controlling data quality for the subsequent analysis.

Structure diagram of the device used to measure niacin skin-flushing.
Generally, healthy people are more reactive to the niacin flush effects than patients with FES (figure 2A vs figure 2B). However, situations also occur where the reactions of healthy individuals and patients with FES are indistinguishable by visual judgement. Our diagnostic algorithm explained below overcomes this ambiguity by using statistical features to evaluate the ‘redness’ of the niacin flush response.
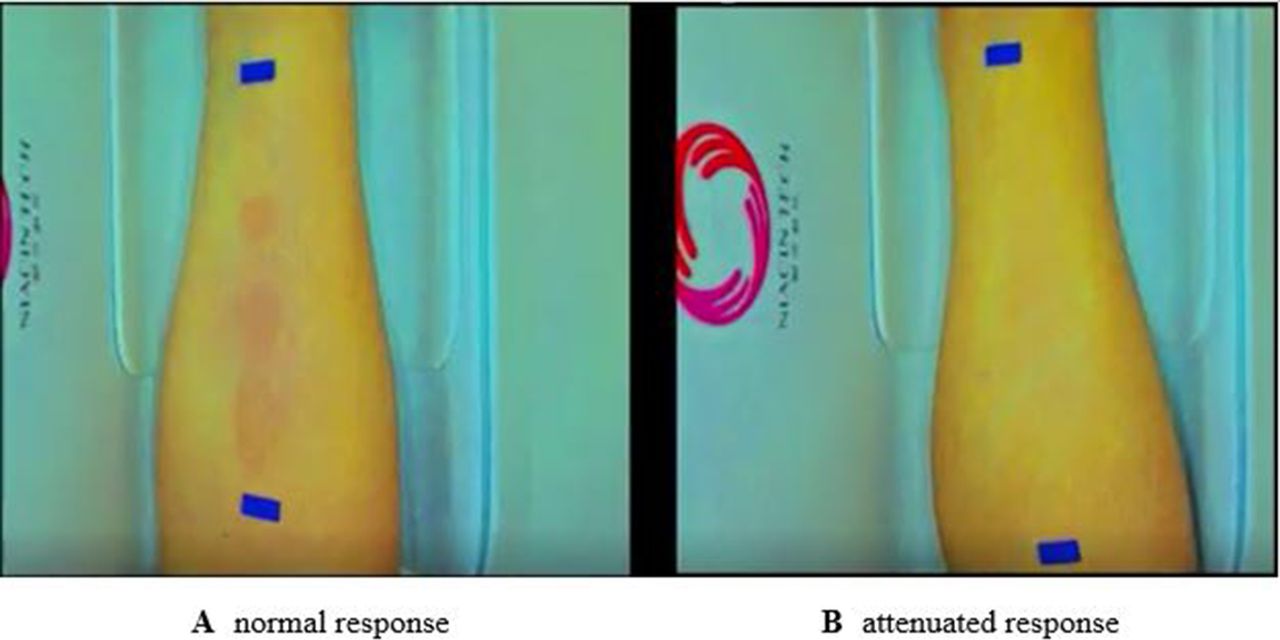
Niacin skin flush response.
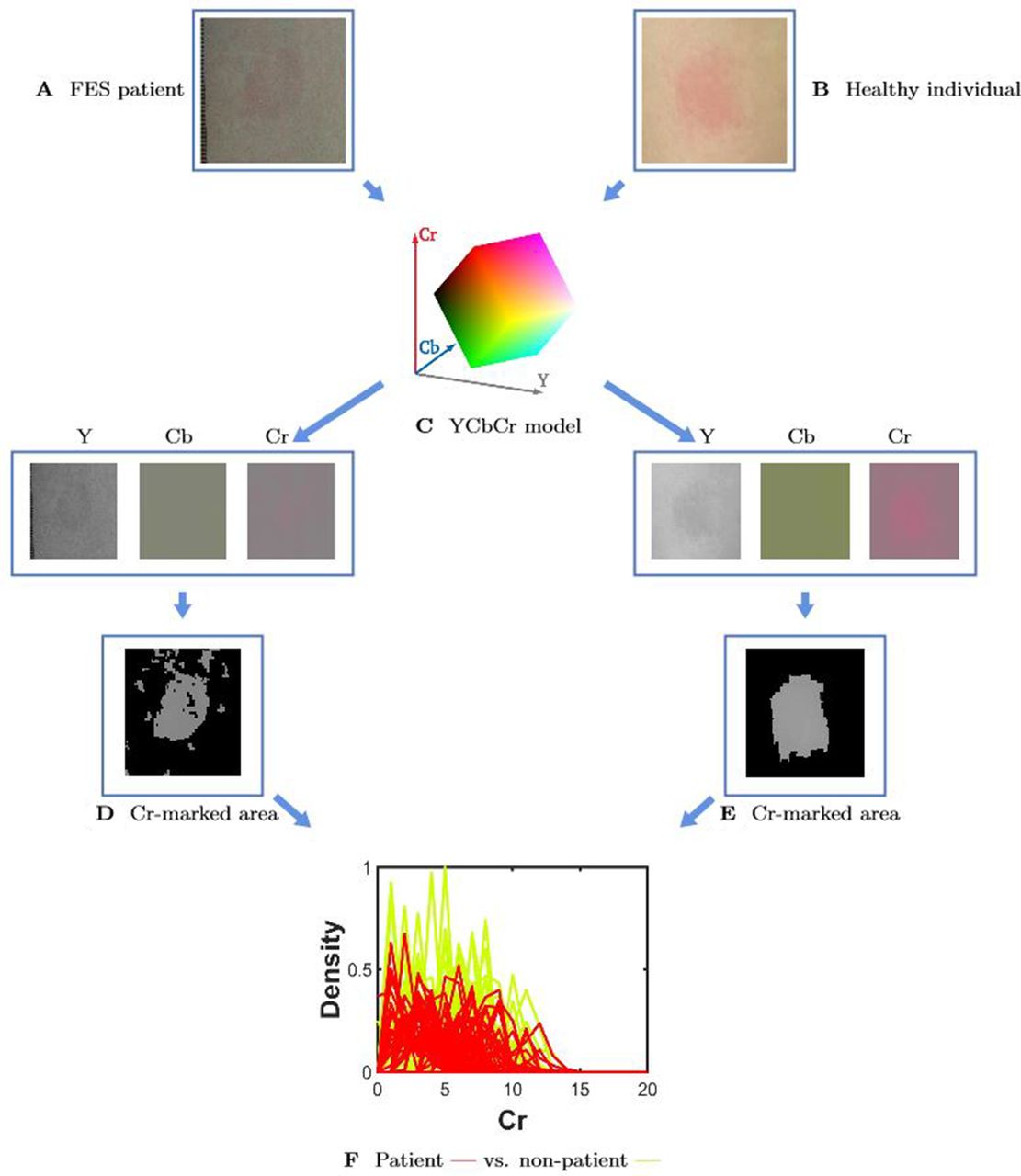
We began by detecting the reaction areas using a convolutional neural network. Then, we quantified the images of the reaction areas (figure 3A,B) through the YCbCr colour system (figure 3C): Y, Cb, and Cr indicate the brightness, blue-difference, and red-difference chrominance components of each image, respectively. By encoding the ‘redness’ with the Cr parameter, we marked the area containing the erythema using the Cr values (figure 3D,E). We then collected the Cr values of individuals’ erythema, standardised by their unique, individual skin colours. Because patients with FES have standardised Cr distributions that are distinct from HCs (figure 3F), we could find a ‘hyperplane separation’ -- which works as a classifier for diagnosis -- between patients and HCs based on the difference in those distributions. More specifically, we treated each individual’s Cr density as the input and a numerical prediction result as the output, with ‘one’ indicating ‘FES’ and ‘zero’ indicating ‘healthy’. We then searched for a set of weights projecting from the input to the output by minimising the prediction error when classifying patients with FES versus HCs. The weights obtained through this minimisation were then applied to generate diagnostic results for the early psychosis screening of individuals with CHR, based upon their skin reaction images. Since such predicted outputs do not precisely equal zero or one numerically, we define the diagnostic result as ‘FES’ if the predicted value is larger than 0.5 and ‘healthy’ otherwise.
{kind=link}
{kind=link}
{kind=link}
Niacin flush response evaluation. FES, first episode schizophrenia.
To justify the validity of our algorithm, we estimated a set of weights using the FES and HC groups; then, we performed a blind test using the 48 individuals with CHR that included 10 conversion cases and 38 non-conversion cases. The prediction results, the positive predictive value (PPV), the negative predictive value (NPV), the sensitivity, and the specificity are displayed in tables 1 and 2. For the in-sample performance within the FES and HC groups, all 54 patients with FES and 69 of the 73 HCs were correctly identified, as shown in table 1. For the out-of-sample performance in the group with CHR, all 10 conversion cases and 33 of the 38 non-conversion cases were correctly predicted, as shown in table 2.
In-sample performance (within the FES and HC groups)
Out-of-sample performance (for the individuals with CHR)
The algorithm also embodies a self-improvement feature. As more individuals get tested, we can collect the traditional diagnoses by follow-up. Then, the classifier can be kept updated by constantly estimating the hyperplane separation with the enlarging sample.
The algorithm described above is installed in our device, along with the classifier derived from the FES and HC samples. When diagnosing individuals for FES in the future, the device could automatically perform an analysis in which the predetermined classifier would generate a test report based on the individual’s standardised Cr density obtained from the forearm images. We have attached a short video as an online supplemental file to illustrate the implementation of this device.
Supplementary video
Discussion
Timely diagnoses and treatment are crucial to reducing the dire prognoses of psychosis, especially for those at high-risk. Presently, traditional FES screening tools that use the niacin response biomarker lack accessibility and accuracy. However, AI technologies allowed us to quantify the niacin response biomarker and develop a dependable, accessible tool for FES detection. As a result, we have designed and configured a device with a diagnostic algorithm that can expedite early psychosis screening. Our AI-assisted method could also be applied more broadly in clinical psychiatry for biomarker-based early screening of mental diseases.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The ID for ethics approval is 2020-100. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
For the purpose of commemorate, Prof. Jeffrey Yao passed away on 22 March, 2018. He was founder and core member of this study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
TZ and JW contributed equally.
Contributors TC proposed the integration of AI technologies into medical research and designed the prototype of the device. HL optimised both the hardware and software of the device. TC, TZ and JW designed the medical study. TC, RT and WX analysed the data. RG provided the clinical data. TZ and JW conducted the clinical experiments. TC, RT and TZ wrote the paper. All authors revised the paper.
Funding This study was supported by National Natural Science Foundation of China (82171544, 81971251, 81671329, and 81871050), Science and Technology Commission of Shanghai Municipality (19441907800, 16ZR1430500, 19ZR1445200, 17411953100, 21S31903100, 2018SHZDZX01, 19410710800, 19411969100, 19411950800)
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.