Article Text

Abstract
Background The ongoing pandemic has led to a global surge in coronavirus disease 2019 (COVID-19)-related mental health research. However, most related publications come from Western countries or China, and their findings cannot always be extrapolated to Arab countries.
Aims This study provides a quantitative and qualitative analysis of mental health research pertaining to Arab countries' response to the COVID-19 pandemic.
Methods A scoping review of the World Health Organization (WHO) COVID-19 database for publications on mental health was conducted by authors affiliated with Arab institutions, including articles from inception to 24 October 2020. The included publications were evaluated for their national distribution, international collaboration, publication type, and main research themes. Methodological quality analysis of the included research studies was performed using the original and modified versions of the Newcastle–Ottawa Scale.
Results In total, 102 articles were included in this study, averaging 4.6 articles per Arab country. Most of the articles emerged from the Kingdom of Saudi Arabia, Jordan, and Egypt. A majority of publications demonstrated international collaboration. Most of the publications were original research studies and cross-sectional in design. The predominant research theme was examining the pandemic’s mental health effects on the general population and healthcare workers. Only 28.0% of the studies were of high methodological quality, whereas 41.5% were moderate and 30.5% were low in quality.
Conclusions Mental health research in response to the COVID-19 pandemic in the Arab region has quantitative and qualitative shortfalls. Arab institutions need to respond to the pandemic promptly in order to address the delineated research gap and to generate higher-quality research output.
- COVID-19
- Mental Health
- Psychiatry
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Arab countries' mental health research contributions are low despite a high disease burden in the region.
Evaluation of mental health research in the Arab region concerning the COVID-19 pandemic is promptly needed.
What this study adds
The Arab world’s mental health research output has multifaceted quantitative and qualitative shortfalls.
A wide gap exists in the Arab world’s COVID-19-related mental health research.
How this study might affect research, practice or policy
This study sheds light on areas of urgent mental health research needs in the region, along with other considerations for potential research improvement.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic is having a profound impact on all aspects of society, including mental well-being. The mental health burden from the ongoing pandemic has been of significant interest to the international scientific community at large and researchers involved in the field of mental health.1–3 This has led to a remarkable acceleration of research during the pandemic, with over 43 000 articles published on COVID-19 in the Scopus and PubMed databases as of 26 August 2020. Of these, 3070 pertained to mental health.2 Western countries, China, and India contributed the most, with 2928 (95%) publications. However, only 13 Arab countries out of 22 (Saudi Arabia, Lebanon, Egypt, Jordan, the United Arab Emirates, Tunisia, Morocco, Oman, Qatar, Bahrain, Libya, Sudan, and Syria) contributed with 94 (3%) publications.2 This is not surprising, as pre-pandemic research has shown that Arab countries produced only 1% of the global publications in mental health research.4 Arab countries’ contributions to the global research on mental health have been plagued by challenges of stigma, conflict, scarce funding, insufficient training, and a shortage of reliable assessment tools.5 This clearly indicates that research output in the Arab region does not meet certain standards and is not commensurate with the magnitude of the disease burden in the area, as psychiatric disorders are one of the leading causes of disability in the region. Calls have been made to close the scientific literature gap between the Arab region and the rest of the world and improve the quality of research.5 Culturally relevant research is essential as it equips policymakers to make informed health policy decisions. This is significant because research conducted elsewhere may be inapplicable to the Arab context as it may not be generalisable to the Arab population due to differences in genetics, culture, socioeconomic standards, and healthcare systems.
The need for research to mitigate mental health consequences was highlighted early in the pandemic by a panel of experts convened by the UK Academy of Medical Sciences.5 However, concerns have arisen that the rapid production of research to address the impact of mental health issues linked to the COVID-19 pandemic has been carried out at the expense of sacrificing scientific rigour. This panel laid out immediate and long-term priorities for mental health research and recommended obtaining high-quality data on the mental health impact of the COVID-19 pandemic across the whole population and specifically among vulnerable groups.6 High-quality research is dependent on the collection of high-quality data, integration across disciplines, and international collaboration.4 5 Rigorous review of research protocols remains the cornerstone of upholding research standards and, thus, safeguarding patients. Lack of adherence to scientific rigour raises concerns about the validity, generalisability, and reproducibility of the research findings. In a recent quality assessment of surveys measuring COVID-19 mental health outcomes in China, only 45% were found to be of high quality.7 Mental health researchers must employ scientific rigour while exploring the direct and indirect psychological and social impacts of COVID-19.
Maalouf and colleagues2 recently published a bibliometric analysis highlighting the mental health research response to the COVID-19, Ebola, and H1N1 outbreaks and confirmed that mental health research output is already greater for COVID-19 than all of the other outbreaks combined. Our study builds on their research by focusing specifically on Arab countries and examining the quality of COVID-19 mental health research in the region. By means of a scoping review, our study aims to map and delineate the mental health literature and scholarly productions that emerged in response to the COVID-19 pandemic in the Arab world. We aim to identify the type and themes of research published, scientific gaps, and areas necessitating future research. Additionally, we endeavour to scope the quality of the published research by examining compliance with basic methodological quality criteria.
Methods
Search strategy
This study is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) reporting guidelines.8 A priori registered protocol was not developed. We conducted a systematic literature search of the WHO COVID-19 database from its inception to the date on which the search was conducted (24 October 2020). The WHO COVID-19 database regularly curates COVID-19-specific citations from multiple bibliographical databases including MEDLINE, PsycINFO, Scopus, CINAHL, Embase, Web of Science, in addition to preprint servers, manual searches and experts’ referrals.9 10
A search query was constructed using mental health-related keywords and the names of the 22 Arab countries: (Egypt* OR Saudi* OR KSA OR Leban* OR Tunis* OR Emirat* OR UAE OR Jordan* OR Qat* OR Moroc* OR Iraq* OR Kuwait* OR Palestin* OR Bahrain* OR Alger* OR Sudan* OR Syria* OR Yemen* OR Libya* OR Somalia* OR Mauritania* OR Djibouti* OR Comoros OR Oman*) AND (Mental* OR Psych* OR stress* OR depress* OR anx* OR addict* OR schizo* OR mood*). No COVID-19-related keywords were added to the query due to the high topical specificity of the WHO COVID-19 database.
Inclusion and exclusion criteria
All articles published by authors affiliated with Arab countries and reporting on the diagnostic, prognostic, or therapeutic aspects of psychiatric disorders or psychological well-being with respect to COVID-19 were included. A coauthoring country was considered as an Arab country if it was one of the 22 member states of the Arab League (ie, Algeria, Bahrain, Comoros, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Palestine, Qatar, Kingdom of Saudi Arabia (KSA), Somalia, Sudan, Syria, Tunisia, United Arab Emirates (UAE), and Yemen).11 Besides including only articles published in English or Arabic with full texts available online, no restrictions were placed on study design, publication type, or publication status. We excluded publications lacking affiliation to Arab countries or unrelated to COVID-19 and mental health research. Similarly, publications in languages other than English or Arabic or with unavailable online full texts were excluded.
Article screening and data extraction
Three of the authors (IHEA, EA-J, and YZ) independently screened the titles, abstracts, and affiliation details of all retrieved citations against our eligibility criteria for full-text screening.
Articles lacking abstracts and/or affiliation information were automatically included for full-text review. Subsequently, full texts of the articles that passed the preliminary eligibility screening were retrieved and examined for final inclusion or exclusion in the study. Articles lacking full-text availability online were excluded from further data extraction and analysis.
Subsequently, the following parameters from the included articles were abstracted independently by the same three authors, using a standardised and piloted data collection form:
Study title
Country of author’s affiliation (in case of articles whose authors’ affiliations include multiple Arab countries, each country was recorded)
International collaboration (defined by the presence of at least one author affiliation from a different country)2 4
Publication type
Study design
Target population characteristics, including age, population type, and setting.
Discrepancies during screening and data extraction were identified and resolved by referring to two other authors (SO and OW).
Data summary and synthesis
Charted data were synthesised and stored in a tabular format using a Microsoft Excel-based spreadsheet. Then, descriptive content analysis was conducted to identify key research themes emerging from included research articles. Accordingly, two of the authors (MHMOH and IHEA) independently examined the charted data and full texts of included research studies. Editorials, letters, expert opinion reviews, and case reports were excluded from this process as they were not considered as primary research articles. Consequently, broad codes corresponding to key research themes were assigned to each study based on their research questions and target population characteristics; assigning more than one theme per study was allowed. Disagreement in this process was resolved through discussion and consensus between the same two authors. Finally, abstracted parameters were aggregated and displayed in summary graphs (tables and bar charts) and statistics (counts and percentages).
Quality assessment
Two authors (MHMOH and IHEA) assessed the methodological quality of the included research articles independently and in duplicate. At this point, qualitative research studies were excluded from the assessment as there is no consensus regarding a reliable method for examining the quality of qualitative research in systematic reviews.12 The quality of included case-control and cohort studies was assessed using the Newcastle–Ottawa Scale (NOS),13 and cross-sectional studies were evaluated by the modified version of the NOS.14 Both instruments assess studies based on three broad categories: the selection of the study groups, the comparability of the groups, and the ascertainment of either the exposure or the outcome.13 14 A visual star-based scoring system was adopted for the studies: seven stars or more were considered to be of high quality, six or five stars were considered to be of moderate quality, and four stars or less were considered as low quality. Disagreements in scoring were resolved by consensus and by consulting a third author (SO).
Results
Search results
Two-hundred and twelve records were retrieved using the search query. After removing duplicates, 195 records remained. Of these, 93 were excluded: 67 had irrelevant topics (examined areas of the COVID-19 outbreak not included in our inclusion criteria--knowledge and practice of physicians during the pandemic, the impact of the outbreak on patient care and medical education, public misconceptions, region-specific and climate-specific prevalence and incidence, infection rate prediction models, and precautionary measures). Only 102 articles were included for further analysis. Figure 1 illustrates the PRISMA flow chart of the inclusion and exclusion process. Details of the included individual publications are provided in online supplemental table 1.
Supplemental material

Preferred reporting items for systematic reviews and meta-analyses flowchart of the inclusion/exclusion criteria. COVID-19, coronavirus disease 2019; KSA, Kingdom of Saudi Arabia; UAE, United Arab Emirates.
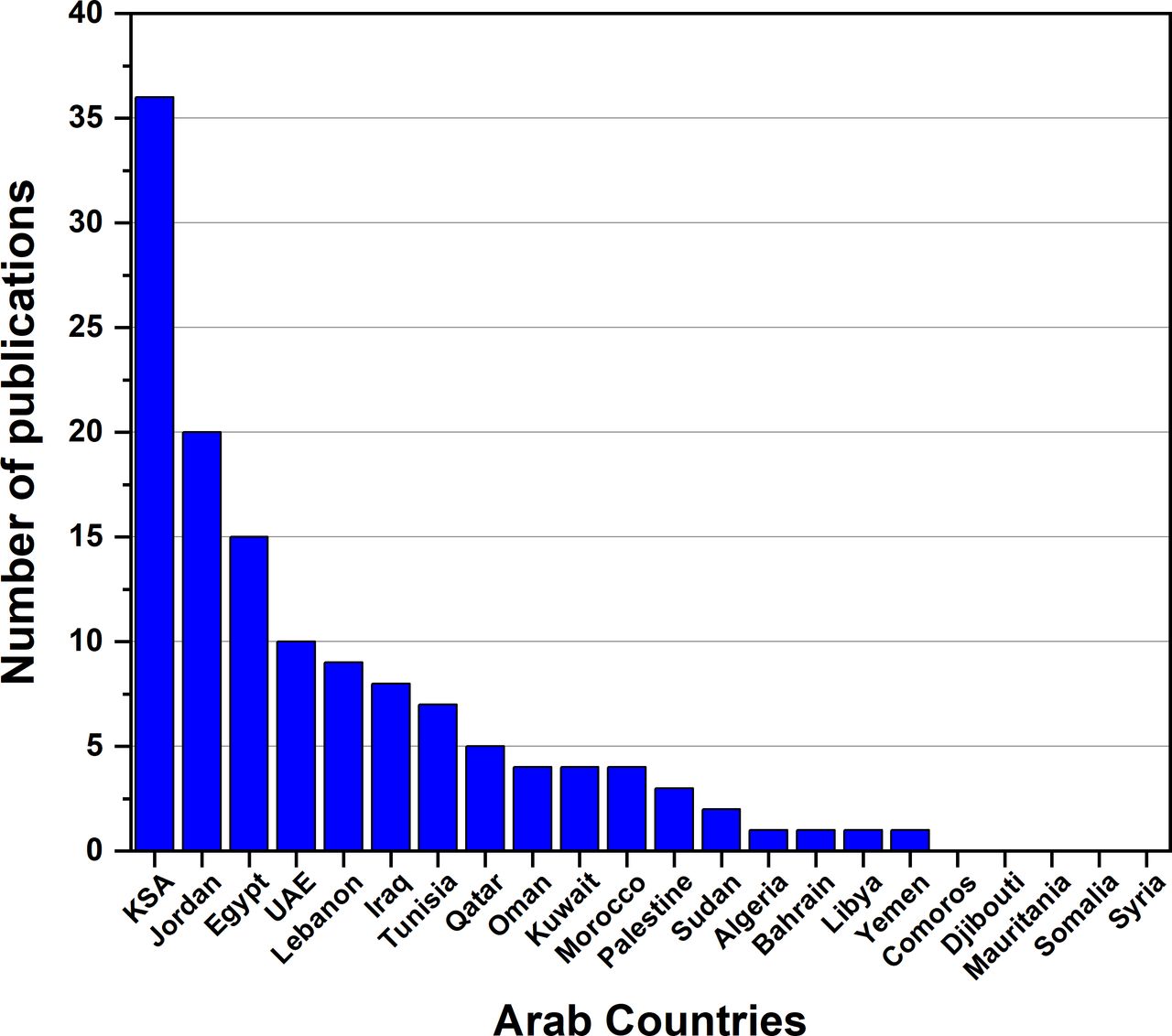
Publications by Arab countries
The three most productive countries were KSA (n=36, 35.3%), Jordan (n=20, 19.6%), and Egypt (n=15, 14.7%), respectively. Fourteen other countries contributed the remaining proportion, and five countries had no publications (figure 2).

Number of COVID-19 mental health-related publications by Arab countries from inception to October 2020. Some publications may be affiliated with more than one country, so the sum of articles by country does not equal the sum of all included articles. All publications by country are included, regardless of their types or analysis-wise exclusion. KSA, Kingdom of Saudi Arabia; UAE, United Arab Emirates.
Scholarly collaboration
More than half of the publications (n=56, 54.9%) involved international collaboration; nearly two-thirds of these were with institutions from non-Arab countries (n=35). The remainder of the publications (n=46, 45.1%) had collaboration with domestic institutions within the same country.
Publication types
Most publications were original research papers (n=84, 82.4%), the majority of which were cross-sectional studies (n=81, 79.4%). No longitudinal or interventional studies were identified (figure 3).
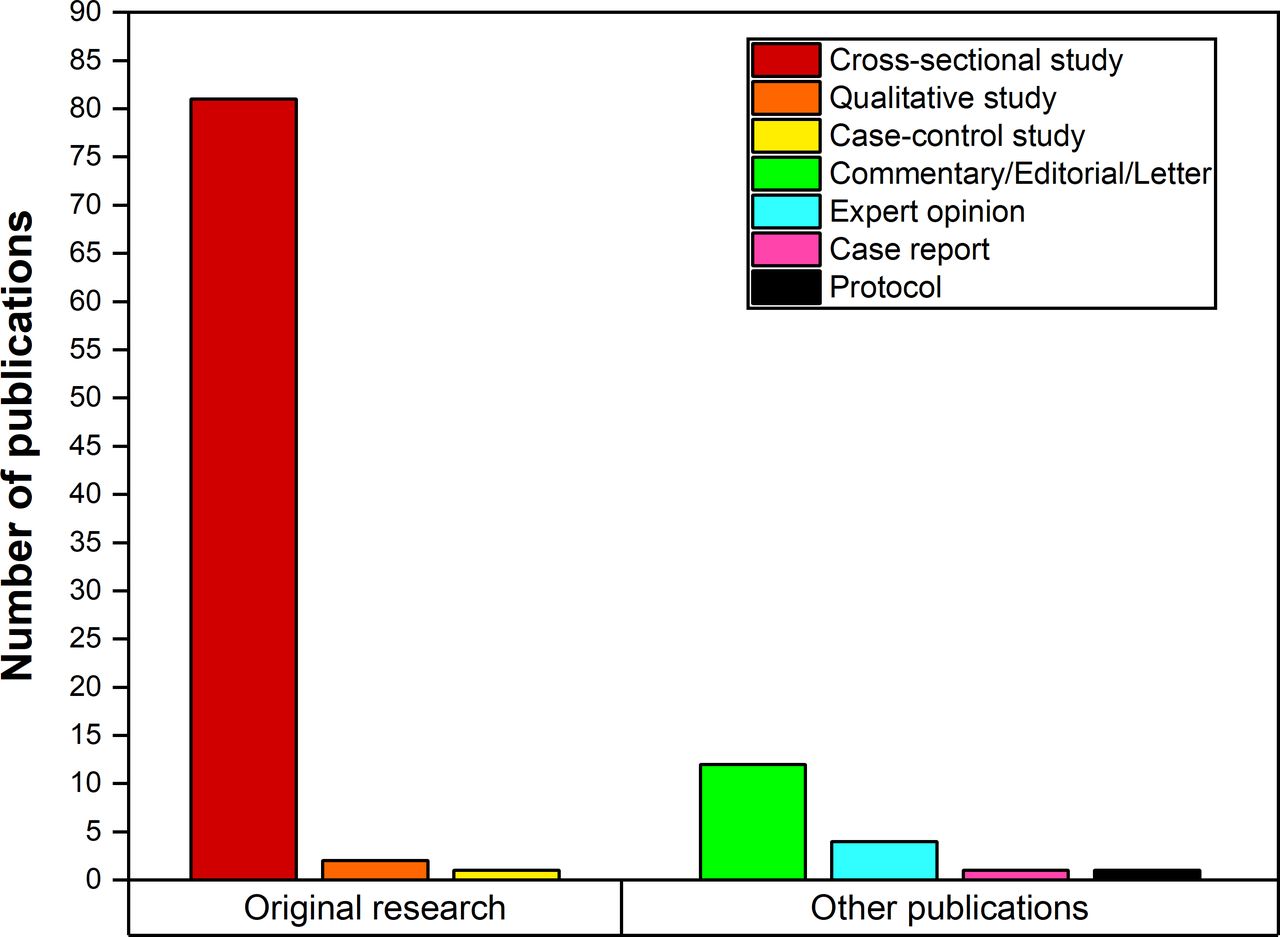
Number of Arab region COVID-19 mental health-related publications by type from inception to October 2020.
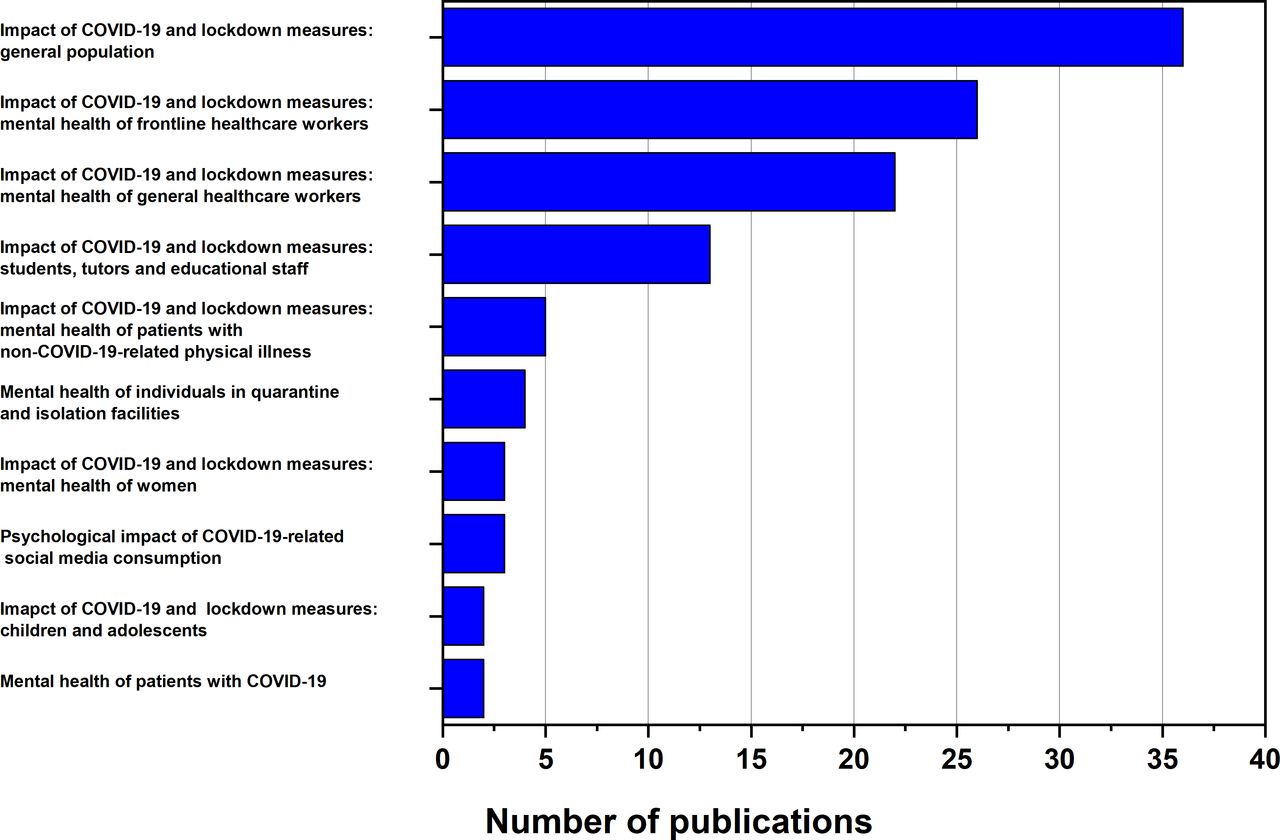
Research themes
Ten main research themes were identified. Thirty-six studies investigated the mental health burden of COVID-19 and lockdown measures on the general public (42.9% (36/84)), 26 studies focused on frontline healthcare providers (31.0% (26/84)), and 22 studies examined general healthcare providers (26.2% (22/84)). These three research themes accounted for 78.6% (66/84) of the included research studies (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of COVID-19 mental health-related research themes in Arab region publications from inception to October 2020. Since each study could be assigned to more than one research theme, these figures do not equal the sum of the total number of included studies. COVID-19, coronavirus disease 2019.
Quality assessment
As detailed in the online supplemental tables 2–5, of the 82 eligible and included research studies, only 23 (28.0% (23/82)) of them were high quality, while 34 (41.5% (34/82)) and 25 (30.5% (25/82)) studies were of moderate and low quality, respectively. The most common methodological shortcomings were poor representativeness of samples, absence of sample size justification, and lack of description of non-respondents.
Supplemental material
Discussion
In this review, by quantitative and qualitative assessment, we systematically examined COVID-19-related publications pertaining to mental health in Arab countries.
Main findings and comparison with global literature
Despite adopting broad selection criteria, only a modest body of evidence was identified, averaging 4.6 publications per Arab country. These figures are in contrast to the global trend showing a massive expansion of medical publications amidst the pandemic.15 However, this finding is consistent with previous studies reporting low Arab World contribution to global mental health research.5
A majority of the included publications from Arab countries demonstrated international collaboration. The proportion of these collaborative efforts outweighed previous reports from the region4 and the aggregate global figures (22%) for COVID-19-related mental health research.2
None of the published studies were interventional, and most of the observational studies were cross-sectional, with no prospective studies identified. This could be because we analysed publications within the first eight months of the pandemic; interventional and prospective studies require a longer period before publication.16 Another explanation is that authors from Arab countries resort to cross-sectional studies because they are easier to conduct, inexpensive, and require fewer resources.17
Our quality assessment indicated that only a minority of studies were of high methodological quality. This aligns with a previous study which showed that Arab countries fell behind other countries in terms of publishing mental health research publications in top-quartile journals.4
The predominant focus of the identified studies concerned the impact of COVID-19 and its socioeconomic implications on the psychological well-being of the public and other diverse healthcare provider groups. Another area of interest in a notable proportion of the included studies was the impact of the pandemic with the associated closure of educational facilities on the mental health of students and staff. These findings are consistent with recently published results from other regions18 that might reflect a global concern towards the rising burden of mental health problems among these population groups.19–31
Strengths and limitations
Our study is the first, to our knowledge, to have examined the scope and quality of COVID-19 mental health research in Arab countries. Our study met all PRISMA-ScR checklist criteria, other than not developing a registered protocol before conducting this study. We used inclusive selection criteria and search query terms with high sensitivity. We also used standardised instruments. In addition, all studies were independently assessed by a group of assessors, and discrepancies were resolved by a separate group. We extended the scoping purpose of the review by mapping the quality and scientific rigour of the included research articles, which might not be achieved through traditional descriptive quantitative and thematic analyses.32
This scoping review has a number of limitations. We only searched the WHO COVID-19 database for this review. However, this database gathers scientific publications from the most important databases in the medical field.9 10
Moreover, as many of the backbone indexes of the WHO-COVID-19 database have higher coverage of English than non-English publications (eg, PubMed/MEDLINE,33 Scopus, and Web of Science34 35), a proportion of evidence might not be covered in our work.
Despite employing a comprehensive search strategy, there is also a possibility that some relevant topics might have not been fully retrieved by our query, especially if they were introduced as abbreviations (eg, ‘BD’ instead of ‘bipolar mood disorder’ and ‘PTSD’ instead of ‘post-traumatic stress disorder'). Finally, our results do not represent the complete course of the fast-growing literature of the current pandemic, since the COVID-19 pandemic continues to evolve.
Implications
This review delineates a wide quantitative and qualitative gap in the Arab world mental health literature that necessitates a timely response from policymakers and researchers.
This work outlines that the amount of research that has come from the Arab world has not been able to meet the population demands produced by the COVID-19 pandemic. Although the number of publications about mental health from Arab countries has been growing at a much faster rate than the rest of the world,4 36 steps need to be taken to promote both quantity and quality of mental health research in the region. The current pandemic sheds light on the importance of the inter-relationship between physical and mental health.37 An adequate response to the pandemic must also entail addressing mental health issues.38 Planning an optimal mental health response plan tailored to the needs of each country or region largely relies on scientific research from that same country or region, since extrapolating data from other countries and regions is not always possible or beneficial.39
Our findings emphasise the urgent need for more research that investigates the mental health problems of diverse, vulnerable, and underprivileged social groups. Ideally, these results will stimulate directing investments for future research that will address the gaps we have identified in the literature.
In addition, our scoping review identified high research activity related to the pandemic-induced mental health burden of the general population, healthcare workers, students, and educational staff. This finding indicates that further work is needed to gain deeper insight into these groups’ psychological needs and inform tailored interventions to address these needs.
Our findings also demonstrated that the preponderance of COVID-19-related mental health literature emerging from the Arab world was cross-sectional studies, the majority of which were of substandard methodological quality. Cross-sectional studies are useful to examine the prevalence and generate hypotheses. However, they have several limitations, including the inability to investigate the temporal relationships between outcomes and risk factors, and the difficulty to interpret the exact meaning of any statistical associations that might be observed.17 40 They are also more prone than other types of studies to non-response bias, recall bias, and confounding bias.17 In the hierarchy of scientific evidence, cross-sectional studies are generally regarded as being among the weakest, superior only to case reports and case series.41 42 That mental health studies in the Arab world are primarily cross-sectional illustrates that the quality of research still largely lags behind international standards, despite some observed improvement over the last few years.4 5
Our review helped identify that most publications produced by Arab countries were not just lower in the evidence hierarchy, but also suffered various methodological shortcomings. These methodological flaws can severely impede the generalisability of any findings and seriously affect the quality of the studies.43 Since the objective of any research is to extrapolate data beyond the studied sample, these flaws are rendered as severe limitations.43 44 It is crucial that actions are taken to improve the quality of mental health research in Arab countries. These actions could include greater emphasis on research skills in mental health training programmes and increased incentives for high-quality research in the field.5 Academic institutions in Arab countries need to prioritise psychiatric research and pool resources, if possible, through mutual collaborations.5 Such collaborations have previously been associated with higher quality research publications4 5 and may help promote mental health research in the Arab world. Finally, our analysis has revealed the expansion of international research collaboration between Arab and non-Arab countries, and this finding could further nurture these collaborative efforts.
Conclusion
Because mental health is even more sensitive to cultural and societal differences than physical health, direct extrapolation of relevant Western research findings to non-Western sociocultural contexts is limited in application. However, presently mental health research pertaining to COVID-19 in Arab countries continues to have quantitative and qualitative shortfalls. Collaboration of academic institutions in Arab countries both regionally and within the international community can promote excellence in mental health research and enhance the overall quality and range of published papers. Higher-quality research, in turn, could translate into evidence-based plans tailored to the specific COVID-19-related mental health needs of Arab countries.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Dr Mohamed H.M.O. Hassan obtained his MBBCh degree from the Faculty of Medicine, Ain Shams University, Cairo, Egypt in 2012. After completing his psychiatry residency training at Hamad Medical Corporation, Doha, Qatar in 2019, he is currently serving as a second-year Advanced General Adults Psychiatry Fellow at the same institute. Dr Hassan’s areas of interest span a broad range of topics, including healthcare services development and evaluation, travelers’ mental health, scientometrics and secondary research, among other aspects of translational psychiatry and clinical neuroscience.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
MHMOH and IHEA are joint first authors.
Contributors MHMOH, SO and OW designed the study. MHMOH, SO and OW constructed the search and data extraction strategy. IHEA, EA-J and YZ screened the studies and extracted the necessary data. MHMOH and IHEA conducted the quality assessment of the included studies. MHMOH, IHEA, SO and OW drafted the manuscript. MHMOH, SO and OW made critical revisions. All authors read and approved the final version of the manuscript. Both MHMOH and IHEA are joint first authors. MHMOH is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.