Article Text

Abstract
Background Marijuana use among adolescents, including high school students, has been consistently reported to be associated with a high incidence of suicidal behaviours. Little empirical research has been conducted on the propensity impact of marijuana use on suicidal behaviours in Africa.
Aims To assess factors associated with marijuana use and further quantify marijuana use as an associated factor of suicidal behaviours, including repeated attempted suicide, suicidal ideation and suicide planning, among high school students in Africa.
Methods A cross-sectional study was conducted among 32 802 school-going adolescents using the Global School-Based Student Health Survey data from 10 African countries grouped into West Africa, North Africa, South-East Africa, South Africa and East Africa subregions. Marijuana use and repeated attempted suicide were the main outcome variables. We employed double selection least absolute shrinkage and selection operator poisson regression model to assess risk factors associated with marijuana use and dominance analysis to establish ranked important and common risk factors. Inverse probability weighting poisson regression adjustment was applied to assess impact.
Results The prevalence of marijuana use and repeated attempted suicide were 3.7% (95% CI: 3.1 to 4.3) and 6.6% (95% CI: 5.9 to 7.4), respectively. The most important risk factor for marijuana use generally across the countries and specifically in three subregions was alcohol consumption, which constituted approximately 40% of the impact. The average treatment effect on the treated (ATT) indicated that marijuana use significantly increased the risk of suicidal ideation, suicide planning and repeated attempted suicide by 12% (ATT=0.12 (95% CI: 0.02 to 0.22)), 18% (ATT=0.18 (95% CI: 0.13 to 0.22)) and 31% (ATT=0.31 (95% CI: 0.20 to 0.41)), respectively.
Conclusions Marijuana use was significantly associated with suicidal behaviours (suicidal ideation, planning and repeated attempted suicide) among the students. To achieve Sustainable Development Goal 3.5 (to strengthen prevention and treatment of substance abuse), school-based psychosocial interventions should be streamlined to adequately assess and manage marijuana use. Targeting the most dominant risk factors in this population could translate into the reduction of suicidal behaviours in countries within Africa.
- marijuana smoking
- suicidal ideation
- suicide
- attempted
- suicide
Data availability statement
Data are available in a public, open access repository. Dataset downloaded free online from https://extranet.who.int/ncdsmicrodata/index.php/catalog The data were downloaded from the WHO NCD Microdata Repository. The terms and conditions regarding the use of the GSHS dataset are as follows: (1) the data and other materials provided by the National Data Archive will not be redistributed or sold to other individuals, institutions or organisations without the written agreement of the National Data Archive; (2) the data will be used for statistical and scientific research purposes only. They will be used solely for reporting of aggregated information, and not for investigation of specific individuals or organisations; (3) no attempt will be made to re-identify respondents, and no use will be made of the identity of any person or establishment discovered inadvertently. Any such discovery would immediately be reported to the National Data Archive; (4) no attempt will be made to produce links among datasets provided by the National Data Archive, or among data from the National Data Archive and other datasets that could identify individuals or organisations; (5) any books, articles, conference papers, theses, dissertations, reports or other publications that employ data obtained from the National Data Archive will cite the source of data in accordance with the Citation Requirement provided with each dataset; (6) an electronic copy of all reports and publications based on the requested data will be sent to the National Data Archive; (7) the original collector of the data, the National Data Archive and the relevant funding agencies bear no responsibility for use of the data or for interpretations or inferences based on such uses.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Marijuana is the most widely used (illicit) substance across the world and the consumption is expected to increase, as various countries legalise the recreational use of marijuana.1 2 Globally, it is estimated that over 13 million students aged 15 to 16 years use marijuana, which corresponds to an annual prevalence of 4.7%—a rate that is higher than the rate (3.9%) among the adult population.3 In sub-Saharan Africa, the proportion of adolescents who use marijuana is estimated to be 15.65%, with East Africa recording the highest proportion of 28.9%.4
Adolescence and early adulthood are important periods of developmental transition; it is a time of rapid physical growth, forming social relations, confronting pressure-laden emotions and psychological development.5 6 For some, adolescence is also a time of increased vulnerability to the initiation of drug use including marijuana.2 Marijuana use has been associated with several adverse health outcomes, including impaired cognitive functioning, increased risk of developing both psychotic and affective disorders, dependence, dropping out of school, unemployment, risks of cancer and other health challenges.7 8 Marijuana use among adolescents, including senior high school students, has been consistently reported to be associated with a high incidence of suicidal behaviours.9 10
Notably, though, the nature of the data analysed in this study necessitates the focus of this study to be on suicidal ideation, planning and repeated attempted suicide. Globally, 78% of all suicides are reported in low- and middle-income countries (LAMICs)11; suicide is now the second leading cause of death for those between the ages of 15 and 29 years.12
Across the world, the pooled 12-month prevalence estimates of suicidal ideation, planning and attempts are 7.5%, 14.2% and 4.5% respectively.13 Suicidal ideation has been reported to be higher among adolescents in Africa with a pooled 12-month prevalence estimate of 21%, compared with 8.0% in Asia.14 Similarly, a higher pooled 12-month prevalence estimate of suicide planning has been reported in Africa (23.7%) compared with the overall estimate of 17% across LAMICs.15 Also, the aggregate 12-month prevalence estimate of suicide attempts is higher in Africa (16.3%) relative to other regions of the world, including Asia (5.8%), Europe (3%), North America (3%) and Oceania (2.4%).13–16
Suicidal ideation and planning are critical risk factors for attempted suicide17; however, the most important risk factor for death by suicide across all age groups within the general population is previously attempted suicide.18–20 In other words, repeated attempted suicide represents the single strongest risk for suicide.18 21 22 Whereas there is emerging significant evidence on suicidal ideation, planning and attempts, and associated risks and protective factors among adolescents in Africa,13 we are aware of only one recently published study that has reported the association between marijuana use and repeated attempted suicide among school-going adolescents in Ghana.23 The evidence suggests that, compared with non-users of marijuana, adolescents who used marijuana were significantly 2 to 5 times likely of repeated attempted suicide during the previous 12 months.23 This study, therefore, aimed to expand this evidence base by (1) estimating the prevalence of marijuana use and suicidal behaviours, including repeated attempted suicide, (2) determining risk factors associated with the use of marijuana and (3) assessing how marijuana use influences suicidal ideation, planning and repeated attempted suicide among high school students within and across the five subregions of Africa.
Methods
Data source
Data from the Global School-Based Student Health Survey (GSHS) conducted by WHO and the Centers for Disease Control and Prevention (CDC), with support from United Nations International Children's Emergency Fund (UNICEF), United Nations Educational, Scientific and Cultural Organization (UNESCO) and United Nations Programme on HIV/AIDS, were used for this study. The core objective of the GSHS is to provide accurate national-level data on health behaviours and outcomes as well as risk and protective factors among students. This school-based survey was conducted to help participating countries to develop priorities, establish programmes and advocate for resources for school health and youth health programmes and policies and to allow international agencies, countries and others to make comparisons across countries regarding the prevalence of health behaviours and protective factors.24
Study design and participants
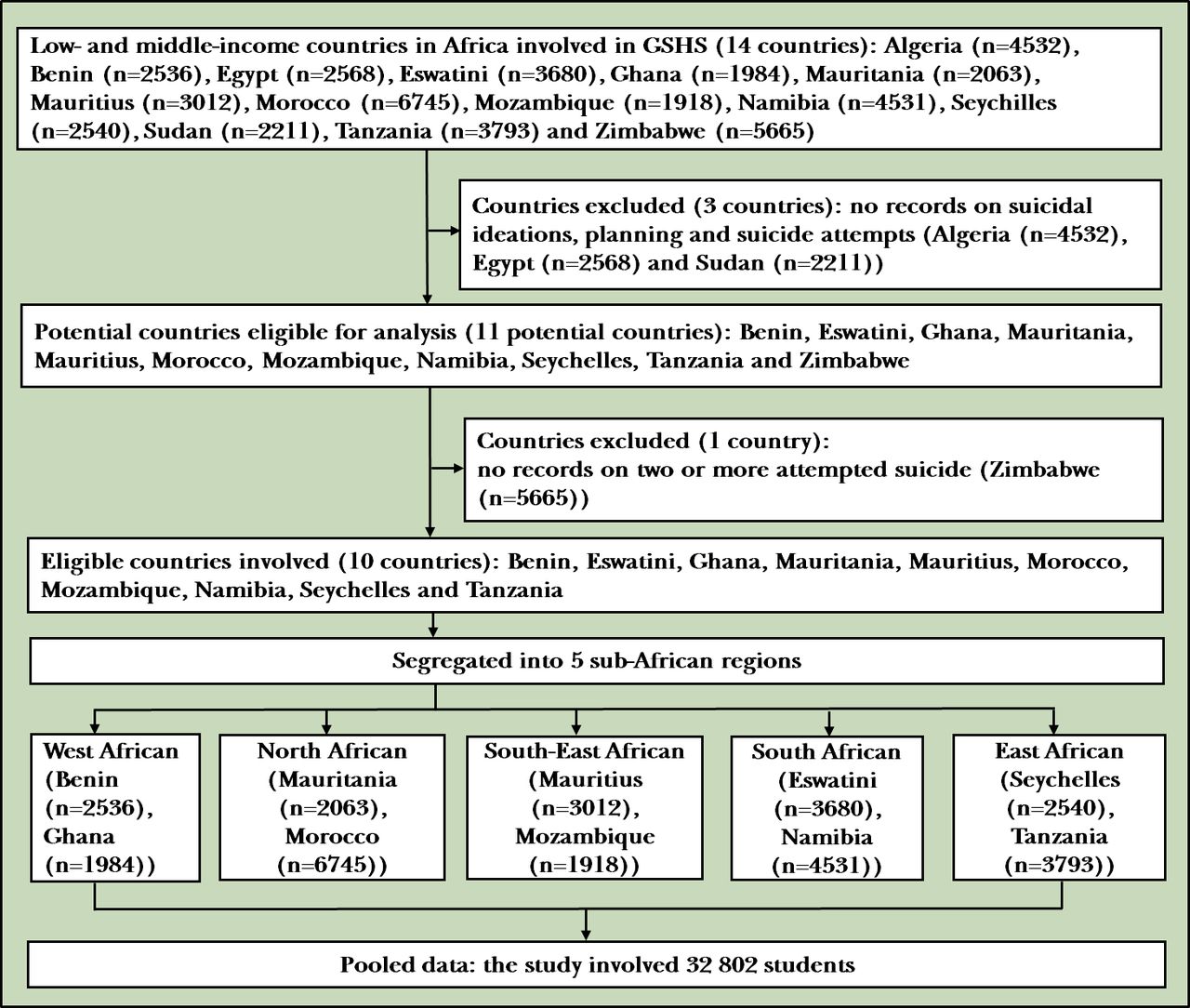
The GSHS was a cross-sectional study with a two-stage cluster sampling method. Probability proportional to school enrolment size was adopted at the initial stage to sample schools for the study. Students were randomly selected from each school to participate. This study is a secondary analysis of the GSHS data involving 32 802 senior high school students from 10 African countries (Benin (year 2016), Eswatini (year 2013), Ghana (year 2012), Mauritania (year 2010), Mauritius (year 2017), Morocco (year 2016), Mozambique (year 2015), Namibia (year 2013), Seychelles (year 2015) and Tanzania (year 2014)). The countries were further grouped into five subregions: West Africa (n=4520), North Africa (n=8808), South-East Africa (n=4930), South Africa (n=8211) and East Africa (n=6333). This was done using the Commonwealth classification.25 Individual country sample, year of GSHS, sample size involved and countries and the corresponding subregions are presented in figure 1.
{kind=link}
Flow chart defining participants involved in the study. GSHS: Global School-Based Student Health Survey.
Survey data collection
A country-specific standardised self-report questionnaire for the GSHS was adopted from WHO/CDC standardised generic questionnaire. In each participating country, rigorously trained data collection personnel and research assistants distributed the questionnaire to the participants; students self-responded to the questionnaire on a computer scannable answer sheet. Items on the questionnaire covered sociodemographic characteristics of participants (eg, sex and age), alcohol and drug use, dietary behaviours, hygiene, mental health (eg, loneliness, sleeplessness, suicidal ideation, suicide planning and suicide attempts), physical activity, protective factors, sexual behaviours, tobacco use and violence and unintentional injuries.
Outcome measure
The primary outcome variables considered in this study were 12-month prevalence estimates of suicidal ideation, planning and repeated attempted suicide. For suicidal ideation and planning, GSHS asked students binary response (yes/no) rated questions: suicidal ideation–During the past 12 months, did you ever seriously consider attempting suicide? and suicide planning–During the past 12 months, did you make a plan about how you would attempt suicide? These variables were recoded with response ‘yes’=1 or ‘no’=0. For suicide attempts, GSHS asked students, During the past 12 months, how many times did you actually attempt suicide? Responses to the item were rated 0 time, 1 time, 2 to 3 times, 4 to 5 times and 6 or more times. For analysis in this study to measure the 12-month prevalence of repeated attempted suicide, we recoded the responses as ‘no’=0 (combined 0 and 1 time) or ‘yes’=1 (combined 2 to 6 or more times).
Exposure variable
The key exposure variable considered a priori in this study based on the previous study23 was marijuana use among senior high school students. Students were asked, During the past 30 days, how many times have you used marijuana? The responses were further recategorised into ‘none’ (0 time)=0 or ‘yes’ (1 or 2 times, 3 to 9 times, 10 to 19 times and ≥20 times)=1.
Covariates
This study assessed 20 covariates involving sex differential, age group (≤17 or ≥18), grade (low level (first to third year average) and high level (fourth year average or higher)), the experience of hunger (no or yes), bullying victimisation (no or yes), experience of insomnia (no or yes), having close friends (none, 1 friend, 2 friends or ≥3 friends), weekly smoking exposure (never, 1 to 2 or ≥3), parent smoker (no or yes), alcohol intake (no or yes), truancy (no or yes), social support at school (no or yes), loneliness (no or yes), checking of homework by a parent (no or yes) and engaging in a physical fight (no or yes). Detailed variable definition, type of variable, measurement and scale of measurement can be found in online supplemental table 1.
Supplemental material
Data analysis
The first approach to data analysis was carried out by summarising the background characteristics of the participants studied. This was performed by adjusting for the denormalised design effect of the GSHS (adjusting for the primary sampling unit, stratification and the sampling weight). Denormalisation of the sampling weights was computed by dividing the sampling weights by the sampling fraction of the students in each country. The Rao-Scott χ2 test statistic, a design-based version of normal Pearson’s χ2, was employed to assess a significant proportion of covariates across the five subregions studied. In a complex sample survey, the Rao-Scott χ2 has been applied both in Ghana26 and elsewhere.27
Considering the high number of covariates included in the study and to prevent any potentially high multicollinearity, the double selection least absolute shrinkage and selection operator poisson regression model (DSLASSOPM) was considered appropriate for our analysis. One key advantage of DSLASSOPM is that it treats collinear covariates differently from traditional estimators. With this model, we specified our covariates that might be included in the model and then specified the variables to be included in the model for double selection. After identifying significant factors associated with marijuana use from the DSLASSOPM model, we then applied a weighted dominance analysis developed28 to rank the estimators. This form of analysis was deemed appropriate to estimate the relative importance of factors significantly associated with marijuana use.29
Finally, to address the hypothetical objective of our study, we employed the inverse probability weighting poisson regression adjustment (IPWRA) model by estimating the average treatment effect on the treated (ATT).30 As this study used an observational dataset, a matching procedure was considered appropriate to improve and reduce imbalances in the estimation of an effect between treated (senior high school students who have used marijuana during the past 30 days) and control groups (non-users of marijuana during the past 30 days). The reduction of imbalance in covariates between the two groups increases the likelihood of estimating the association of marijuana use with suicidal ideation, planning and repeated attempted suicide among the students.31 Through cross-sectional data analysis, IPWRA has been applied elsewhere to assess the impact of participation in collective actions on the economic, social and environmental sustainability.32 The conceptual framework defining the analytical process can be found in online supplemental figure 1. Analysis was performed using Stata V.16, and a p value ≤0.05 was deemed statistically significant.
Results
Characteristics of research participants
The study involved 32 802 senior high school students from 10 LAMICs distributed across the five subregions of Africa. The pooled ratio of male to female was almost 1:1 with the highest male ratio occurring among students from the West African region (approximately 2:1). In all, the majority of the students were aged ≤14 years (41.7%), however, in West Africa and South Africa, most of the students were aged 17 years or older (68.9% and 42.9%, respectively). Overall, most of the students were in low level school grades (59.8%), except in West Africa where most of the students were in high level school grades (86.2%). Rao-Scott χ2 test of independence showed that there was a significant difference in proportions of all covariates studied and subregion of resident (all p values <0.001), except truancy (χ2=2.07, p>0.05; table 1).
Characteristics of students in the five African subregions
Prevalence of marijuana use and suicidal behaviours
The overall prevalence of marijuana use among the students was 3.7% (95% CI: 3.1 to 4.3) with the highest prevalence estimate reported among the North African students (6.3%; 95% CI: 5.1 to 7.8). The overall prevalence of repeated attempted suicide was 6.6% (95% CI: 5.9 to 7.4) with the highest prevalence reported among the West African students (10.1%; 95% CI: 8.6 to 11.7). Also, the overall 12-month prevalence of suicidal ideation and planning were 15.0% (95% CI: 14.2 to 15.9) and 14.2% (95% CI: 13.2 to 15.4) respectively. Interestingly, the highest prevalence of suicidal ideation (18.3% ; 95% CI: 17.0 to 20.0) and planning (24.5%; 95% CI: 22.2 to 26.8) both occurred among the South African students (table 2).
Prevalence of marijuana use, suicidal ideation, planning and repeated attempted suicide
Marijuana use and its associated factors
Marijuana use and risk factors were assessed and presented in table 3, both with pooled analysis and individual subregions. The most common factors associated with increased risk of marijuana use were male gender, three or more days exposure to smoking, having a parent smoker, alcohol use and truancy. Unsurprisingly, male gender was associated with increased risk of marijuana use: the overall prevalence of marijuana use was 70% higher among male students compared with female students (adjusted Prevalence Ratio (aPR)=1.70 (95% CI: 1.38 to 2.08)) with the same occurring among students in West Africa but statistically insignificant (aPR=1.70 (95% CI: 0.87 to 3.34)). Meanwhile, the highest risk occurred among male students in South-East Africa (aPR=3.36 (95% CI: 2.07 to 5.45)). In all, students who were exposed to smoking within 3 or more days were approximately 3 times likely to use marijuana (aPR=2.75 (95% CI: 2.11 to 3.58)) compared with no exposure. Exposure to smoking over the past week was over sixfolds likely among South-East African students (aPR=6.15 (95% CI:2.70 to 13.95)) compared with no exposure. Having a parent smoker generally was associated with marijuana use by approximately twofolds, compared with non-parent smokers (aPR=1.78 (95% CI: 1.48 to 2.15)). The same risk factor was 2.4 times higher among North African students (aPR=2.41 (95% CI: 1.89 to 3.08)) compared with non-parent smokers. Alcohol use showed a fivefold influence on marijuana use (aPR=4.53 (95% CI: 3.58 to 5.73)), and this association was over 7 times higher among students in the East African subregion (aPR=7.05 (95% CI: 4.37 to 11.36)). Alcohol use was 80% higher among students in the West African subregion, but this did not reach statistical significance (aPR=1.80 (95% CI: 0.87 to 3.70)). Overall, the prevalence of marijuana use was over 2 times higher among truant students compared with their non-truant counterparts (aPR=2.10 (95% CI: 1.72 to 2.57)). The analysis showed truancy to have a significantly higher prevalence of marijuana use among students in all the five subregions (table 3).
Factors significantly associated with marijuana use among students in five African subregions
Dominance analysis showed that, generally, the most important risk factor of marijuana use was alcohol consumption within three subregions. Overall, alcohol use constituted approximately 40% of the impact (Standardised Dominance Statistics (SDS)=0.404), but in South-East Africa, South Africa and East Africa, alcohol use constituted approximately 34%, 34% and 46% of the share of the variation, respectively. Another key risk factor identified was truancy. Comparatively, truancy was the fourth important risk factor, which constituted about 13% impact on marijuana use; however, in West Africa and North Africa subregions, truancy was the first important risk factor for marijuana use. About 38% of the variation in marijuana use could be explained by truancy in West Africa and 23% in North Africa. Exposure to smoking and having a parent smoker generally were found to constitute about 5% and 9% of the variations, respectively. In South-East Africa and East Africa subregions, smoking exposure was identified as the second key risk factor for marijuana use; it constituted about 21% and 15% of the variation in marijuana use in the South-East and East Africa subregions, respectively. Having a parent smoker emerged as the second important risk factor of marijuana use among students in the North African and South African subregions (table 4).
Relative importance of factors significantly influencing marijuana use among students in five sub-African regions
Marijuana use as a risk factor for suicidal ideation, suicide planning and repeated attempted suicide
Generally, the evidence suggested that marijuana use significantly affected repeated attempted suicide, suicidal ideation and planning among the students. The average treatment effect of marijuana use on repeated attempted suicide, suicidal ideation and planning among the students showed that, overall, marijuana use significantly increased the risk of suicidal ideation by 12% (ATT=0.12 (95% CI: 0.02 to 0.22)), suicide planning by 18% (ATT=0.18 (95% CI: 0.13 to 0.22)) and surprisingly repeated attempted suicide by 31% (ATT=0.31 (95% CI: 0.20 to 0.41)). In terms of individual subregions, marijuana use was found to have a significantly increased risk associated with suicidal ideation by 24% among students in the West African subregion (ATT=0.24 (95% CI: 0.10 to 0.33)) and 13% in the North African subregion (ATT=0.13 (95% CI: 0.06 to 0.20). We also found marijuana use to be associated with increased risk of suicide planning by 24% in West Africa (ATT=0.24 (95% CI: 0.10 to 0.38)), 16% in North Africa (ATT=0.16 (95% CI: 0.11 to 0.22)) and 11% in South Africa (ATT=0.11 (95% CI: 0.02 to 0.20)). Generally, marijuana use was found to be strongly associated with an increased risk of repeated attempted suicide among the students across all five subregions (table 5).
Effect of marijuana use on suicidal ideation, planning and repeated attempted suicide
Discussion
Main findings
Using a large sample of 32 802 school-going adolescents, alcohol use is a significant risk factor of marijuana use (accounted for approximately 40% from dominance analysis). In addition, physical fights, injuries, truancy and having a parent smoker are key factors associated with marijuana use among school-going adolescents in the study countries. Marijuana use appeared to increase the likelihood of suicidal behaviours (12% for ideation, 18% for planning and 31% for repeated suicide attempts).
Prevalence of marijuana use and associated factors
The overall prevalence of marijuana use among the students in this study was 3.7% and was relatively higher among the North African students (6.3%; including Mauritania and Morocco) and and lower among the South-East African students (1.8%; including Mauritius and Mozambique), respectively. The composite prevalence as established in this study was approximately 40% less compared with what has been reported by a similar cross-national study involving nine African countries (4.1%).33 In terms of subregions, Olawole-Isaac et al reported 28.9%, 25.7% and 7.6% in East Africa, South Africa and West Africa, respectively, compared with 2.6% in East Africa, 5.1% in South Africa and 2.4% in West Africa reported in this study. The variations in the reported prevalence estimates of marijuana use between several studies could be owing to the different study designs adopted and the population involved. For example, even though Peltzer and Pengpid used the same dataset as this study, they involved 9 countries with data between 2009 and 2013,33 whereas this study included 10 countries with data collected between 2010 and 2017. In addition, time-specific period of study could be a potential explanation.
This study has found that the most common factors associated with increased risk of marijuana use among school-going adolescents in Africa are male gender, having 3 or more days of exposure to smoking, having a parent smoker, alcohol use and truancy. This finding is in line with other studies that reported higher prevalence estimates of marijuana use among males and found the male gender to be associated with increased risk of marijuana use and other substances compared with their female counterparts.13 34 Similarly, Zapata et al reported in their study among Columbian emerging adults attending college that being a male was a significant predictor of marijuana use, in addition to parental education, perceived stress and having marijuana-using peers.35 Male gender, greater impulsivity and depression were also reported to be associated with marijuana use among college students.36 Also, exposure to smoking, having a parent smoker, alcohol use and truancy have been found as risk factors for marijuana use by other previous studies.4 23 37–39
Interestingly, this study (through dominance analysis) has found that alcohol use represents the most important risk factor for marijuana use; in three African subregions, alcohol use constituted approximately 40% of the overall impact on marijuana use. Engaging in physical fights and having injuries in the past 12 months and truancy were also important risk factors generally. In terms of subregions, truancy was associated with increased risk of marijuana use among high school students in West and North Africa, while alcohol use showed a strong association with increased risk of marijuana use in South-East, South and East Africa. In South-East and East African subregions, smoking exposure was identified to be the second key risk factor for marijuana use, and that it constituted about 21% and 15% of marijuana use. Having a parent smoker emerged as the second important risk factor for marijuana use among students in the North and South African subregions.
Taken together, these findings are consistent with the socioecological model40 41 and the conceptual framework guiding this analysis. The analysis in this study has shown that the factors associated with marijuana use among high school students in Africa are multiple and multilayered, covering personal, family, school and community level factors. However, the cross-sectional nature of this study does not readily allow for the exploration of the subregional-specific factors accounting for these findings. Future studies could employ more robust designs (including qualitative approaches) to help identify context-specific explanations for these statistical findings.
Suicidal ideation, suicide planning and repeated attempted suicide
This study has reported an overall average 12-month prevalence estimate of repeated attempted suicide as 6.6%, ranging from 5.2% (in East Africa) to 10.1% (in West Africa). In assessing repeated attempted suicide, this study adopted a similar method employed to assess the association between marijuana use and repeated attempted suicide among senior high school students in Ghana.23 The previous study reported a 12-month prevalence estimate of repeated attempted suicide to be 11.5%—nearly 2 times the estimate reported by this study. Interestingly, this study has also shown a relatively higher prevalence estimate in West Africa (10.1%), where Ghana is located. Considering that emerging studies on suicidal behaviours among school-going adolescents in countries within West Africa have mostly reported only single episode of attempted suicide, but not repeated episodes,10 it is strongly recommended that future studies examine the prevalence of repeated attempted suicide in West Africa and across the African continent.
The overall prevalence estimates of suicidal ideation and planning during the past 12 months were 15.0% and 14.2%, respectively, with the highest prevalence estimates of suicidal ideation (18.3%) and planning (24.5%) occurring among the South African students, which are still higher relative to the global estimates. A recent global meta-analysis reported relatively lower 12-month prevalence estimates of suicidal ideation (14.2%) and suicide planning (7.5%).13 In Africa, some studies on adolescent suicidal behaviours have reported an approximate overall pooled prevalence of 21% for suicidal ideation.14 39 This is comparatively higher than that reported by this study among African high school students. Similarly, some recent studies have reported relatively higher 12-month prevalence estimates of suicidal behaviours in high school students from other parts of Africa: suicidal ideation (18.2%) and planning (22.5%) from Ghana42 and suicidal ideation (18% in 2002 and 19% in 2008) from South Africa.43 Among persons living with HIV/AIDS, the prevalence of suicidal ideation has been established as 228.3/1000 persons.44 The difference in the prevalence estimates could be attributed to the differences in samples and sampling strategies used, geographical representation as well as differences in methodology.
Association between marijuana use, suicidal ideation, planning and repeated attempted suicide
We found the likelihood of repeated attempted suicide significantly increased by 31% among students who use marijuana, compared with their counterpart non-users. In addition, marijuana use was strongly associated with increased risk of suicidal ideation (12%) and planning (18%). This significant finding affirms the observation that heavy cannabis users are more likely to report suicidal ideation than non-users.45
Generally, whereas marijuana use has been found to worsen negative mental health outcomes and symptoms, including depression,46 47 there is still limited evidence, particularly, from Africa regarding the association between marijuana use and suicidal behaviour, especially, repeated attempted suicide.23 48 Evidence of a recent meta-analysis48 and an earlier longitudinal study49 suggests that chronic marijuana use represents a risk factor for death by suicide, while frequent use of marijuana presents as a risk factor for a daily experience of suicidal ideation.50 51 Suicides among adolescents have a variety of causes.52 Marijuana has mind-altering compounds (like dopamine) that affect the brain and can potentially worsen the symptoms of any mental disorders including schizophrenia and other forms of psychoses.45
Contextually, the finding of this study is consistent with the evidence reported recently from Ghana involving a nationally representative sample of high school students that marijuana use showed a strong positive association with repeated attempted suicide.23 Other studies have shown significant associations between marijuana use and suicidal ideation and suicide attempts, even after having controlled for other (potential) confounding variables, including depression.53–55 Although some studies have explained the strong association between cannabis use and suicidal behaviours based on markers of psychological and behavioural problems,49 further studies using biopsychological approaches are needed to understand the mechanism of repeated attempted suicide in the presence of marijuana use.
Limitations
A related key limitation, though, is that the findings may not necessarily apply to ‘out-of-school’ adolescents, including truants; the GSHS involves only students present on the day of the survey. The cross-sectional nature of the GSHS data does not support the inference of causation. The study’s outcome variables (marijuana use and suicidal behaviours) could also be influenced by mental health problems (eg, depression and anxiety), parental socioeconomic status and social adversities (eg, physical and sexual abuse), but these factors were not included in this study. Besides the influence of non-disclosure, the dataset analysed in this study is likely to be affected by social desirability bias, considering that both suicidal behaviours and marijuana use are criminalised in most African countries.56 57 In addition, participants were selected within the schools, so an absent student did not have the opportunity to be selected for the study, conferring potential limitation. Additionally, recall bias and the problem of the different time intervals for suicidal behaviours and the exposure variable (marijuana use in last 30 days) are potential limitations.
Three countries (Algeria, Egypt and Sudan) were excluded from the analysis of the study because suicidal behaviours were not assessed by the GSHS in these countries. Also, Zimbabwe was excluded from the final list of included countries, as no data on the prevalence of repeated attempted suicide were assessed. Potentially, the exclusion of these countries from this study limits the generalisability of the findings. Longitudinal studies are needed in future to confirm or elaborate the hypothesised causal relationship between marijuana use and suicidal behaviours.
Implication
This study has shown alcohol use, physical fights, injuries, truancy and having a parent smoker as key factors associated with marijuana use among school-going adolescents in Africa. The findings show that marijuana use represents an important risk for suicidal ideation and planning and for repeated attempted suicide among school-going adolescents in Africa. Thus, marijuana use correlated positively with or significantly increased the risk of suicidal behaviours. This evidence underscores the need for school-based intervention and prevention programmes against marijuana use, in particular, and substance use, in general. School-based mental health promotion interventions for the prevention of marijuana use in schools are essential, in addition to tailored marijuana use programmes that support school age children deal with suicidal ideation problems. To achieve Sustainable Development Goal 3.5 (to strengthen prevention and treatment of substance abuse), school-based psychosocial interventions should be streamlined to adequately assess and manage the use of marijuana among students. Targeting the most dominant risk factors in this young population could translate into the reduction of suicidal behaviours in countries of Africa.
Data availability statement
Data are available in a public, open access repository. Dataset downloaded free online from https://extranet.who.int/ncdsmicrodata/index.php/catalog The data were downloaded from the WHO NCD Microdata Repository. The terms and conditions regarding the use of the GSHS dataset are as follows: (1) the data and other materials provided by the National Data Archive will not be redistributed or sold to other individuals, institutions or organisations without the written agreement of the National Data Archive; (2) the data will be used for statistical and scientific research purposes only. They will be used solely for reporting of aggregated information, and not for investigation of specific individuals or organisations; (3) no attempt will be made to re-identify respondents, and no use will be made of the identity of any person or establishment discovered inadvertently. Any such discovery would immediately be reported to the National Data Archive; (4) no attempt will be made to produce links among datasets provided by the National Data Archive, or among data from the National Data Archive and other datasets that could identify individuals or organisations; (5) any books, articles, conference papers, theses, dissertations, reports or other publications that employ data obtained from the National Data Archive will cite the source of data in accordance with the Citation Requirement provided with each dataset; (6) an electronic copy of all reports and publications based on the requested data will be sent to the National Data Archive; (7) the original collector of the data, the National Data Archive and the relevant funding agencies bear no responsibility for use of the data or for interpretations or inferences based on such uses.
Ethics statements
Ethics approval
Ethics approval was not required as it was an observational study from publicly available data. Meanwhile, WHO/CDC country-specific ethical guidelines were strictly observed during GSHS. The country-specific education ministry’s ethical procedures were strictly observed regarding student participation in research activities. Informed consent was obtained from all heads of participating schools, parents/guardians of underage participants (those below 18 years) and all participating students. For underage students, assent and parental consent were obtained for each student. The guidelines for collecting, labelling and packing of data files collected by WHO/CDC were strictly observed.
Acknowledgments
This study was based on public data from WHO and CDC; we are grateful for the data.
References
John Tetteh is a senior research assistant at the Department of Community Health, University of Ghana Medical School in the Republic of Ghana (from 2019). He holds a Bachelor of Public Health degree from the School of Public Health, the University of Health and Allied Sciences, Hohoe, Ghana, and a Higher National Diploma in Statistics from the Accra Technical University. He is a young researcher who has served as a field coordinator for several research projects and has authored research publications. He is currently engaged in the UNICEF ‘Scaling Pneumonia Response Innovations’ (SPRINT)- Ghana project as a Data Analyst. His main research interests include higher statistical models to any complex survey data to influence international, national health, and social policy.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JT had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: JT and GE-F. Acquisition, analysis and interpretation of the data: JT. Drafting of the manuscript: JT, GE-F and SMS. Critical revision of the manuscript for intellectual content: EN-BQ, MAA, NAHS, KOA and AEY.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.