Article Text

Abstract
Background Prospective studies suggest that tea consumption may decrease the risk for cognitive impairment in late life. However, little research has examined the association between tea consumption and cognitive performance across multiple domains. In addition, no research has examined the benefit of tea consumption on cognitive performance among older adults with existing impairment.
Aims The current study examined the association between tea consumption and performance on tasks of global cognitive function, episodic memory and executive function in cognitively healthy (CH) older adults and older adults with mild cognitive impairment (MCI).
Methods The analytical sample included 1849 community-dwelling older adults from the Shanghai Brain Aging Study (65.6% female, mean age of 69.50 (8.02) years). Following ascertainment of cognitive function, 816 were categorised as MCI. In addition to completion of a demographics questionnaire, participants reported their tea consumption and completed a battery of tests to measure global cognitive function, episodic memory and working memory.
Results Independent analyses of covariance revealed a significant association between tea consumption and measures of episodic memory; however, these associations were restricted to CH older adults but not older adults with MCI. Tea consumption was not associated with working memory performance.
Conclusions The current study suggests that the benefit of tea consumption is restricted to cognitively healthy older adults and does not extend to older adults with MCI.
- geriatric psychiatry
- cognition
- life style
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
According to WHO, dementia is a progressive neurodegenerative syndrome that affects approximately 50 million people worldwide, with 10 million new cases diagnosed each year.1 The heterogeneous syndrome may be characterised by decrements in cognitive abilities that significantly impede independent, daily functioning. Among the different variants of dementia, Alzheimer’s disease (AD) and vascular dementia are the most prevalent subtypes, accounting for 60% to 80% of all cases.2 Recognised as a leading cause of disability, dementia impacts the individual’s quality of life and well-being, and may further place burden on family, community and the healthcare system. In 2016, the global economic cost of dementia reached US$948 billion,3 a cost that continues to rise in the context of an ageing population.
There is currently no cure for dementia and available treatments for AD and other dementias are minimally effective at best. Consequently, the examination of lifestyle behaviours that may prevent or delay dementia has surged in the last two decades. Indeed, epidemiological analyses of cognitive trajectory in later adulthood suggest that declineing in cognitive function is largely dependent on modifiable lifestyle behaviours.4 5 Nutrient intakes and nutraceuticals have gained increasing attention over the last decade as potential effect modifiers in the risk of cognitive impairment.6 7 More recently, the benefits of tea consumption for cognitive health in later adulthood has been investigated.
Next to water, tea (aka, Camellia sinensis (L.)) is the most frequently consumed beverage around the world. Although null associations have been reported in some studies,8 epidemiological studies suggest that tea consumption may decrease the risk of cognitive impairment and dementia.9 10 In a meta-analysis of 17 studies investigating the association between tea consumption (green, black/oolong) and the risk of cognitive disorders, it was found that high tea consumption was associated with a reduced risk of cognitive disorders. Furthermore, dose-response analyses of eight studies suggest a dose response in reduced risk from 100 mL/day (6% reduced risk) to 300 mL/day (19% reduced risk), and 500 mL/day (29% reduced risk) of tea consumption.11
Although the exact mechanism remains elusive, multiple bioactive components of tea that may modulate neuronal function have been identified. Tea polyphenols, especially epigallocatechin gallate, have been shown to hold anti-oxidative, anti-inflammatory and neuroprotective properties. Furthermore, theanine has been shown to impart neuroprotective effects through its regulatory effects on glutamate, which is vital for learning and memory. A third bioactive component, notably found in black tea, are theaflavins. Theaflavins have been shown to offer neuroprotective effects through its antioxidant and anti-apoptosis properties.12 Accordingly, tea consumption may protect cognitive processes in late life through various mechanisms of action.
To date, studies examining the benefit of tea consumption on brain health have focused on the prediction of cognitive impairment; however, few studies have examined the association between tea consumption and the performance on specific tasks of cognitive function. In a sample of 712 non-demented Chinese participants aged 55 or older, it was found that tea consumers performed better on tasks of memory and executive function, relative to non-consumers.13 However, this study excluded persons who displayed cognitive impairment and were indexed by a score of <24 on the Mini-mental State Examination.13 As such, the relationship between tea consumption and cognitive performance among older adults with cognitive impairment is unknown.
The objective of this study was to investigate the association between tea consumption and cognitive performance among cognitively healthy (CH) older adults and older adults with mild cognitive impairment (MCI). Based on previous research, it was hypothesised that tea consumption would associate with better performance on cognitive tasks of episodic memory and working memory. It was also hypothesised that this association would be observed among older adults with MCI.
Methods
Data source and the participants
The analytical sample was derived from Shanghai Brain Aging Study, a prospective cohort study established in July 2016. Data for the current study are restricted to baseline measures, collected between July 2016 and June 2018 across nine community sites in Shanghai. To be included in the study, participants were required to be 55 years of age or older, and to be living in Shanghai. As illustrated in figure 1, a total of 2026 participants were recruited into the study. Participants were deemed ineligible if they presented with factors that would prevent completion of the cognitive testing protocol, including impairments in vision, hearing and illiteracy. For the current analytical sample, 177 participants were removed due to missing cognitive assessments or diagnosis, gender or age, and/or tea consumption data, which resulted in a total sample of 1849 participants.
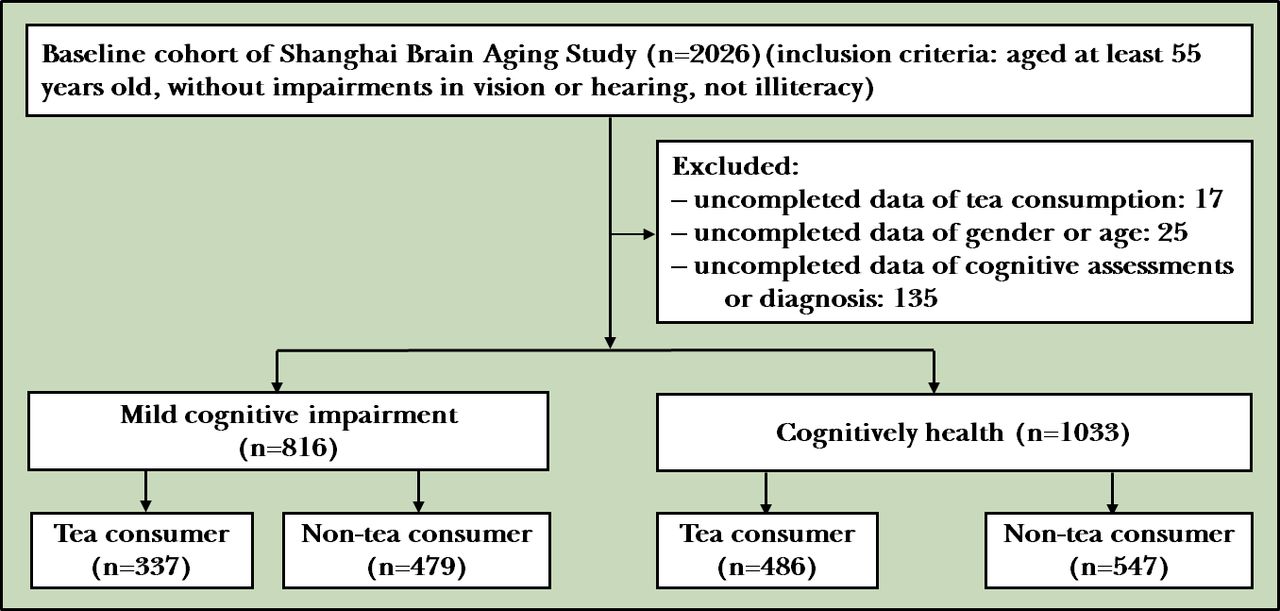
{kind=link}
Flowchart of the study.
Ascertainment of cognitive status
Cognitive status was determined by a comprehensive assessment which included a medical history review, a physical examination, cognitive assessment (normed reference scores by sex and education level), self-reported daily activities of living and neuroimaging biomarkers. MCI was diagnosed according to the core diagnostic criteria of the National Institute on Aging and the Alzheimer’s Association14: (1) concern regarding a change in cognition provided by the participant, the participant’s informant or a clinician; (2) objective evidence of impairment in one or more cognitive domains, including memory; (3) preservation of independence in functional abilities; (4) not demented. A total of 816 participants met the criteria for MCI.
Cognitive performance
Participants completed the Montreal Cognitive Assessment (MoCA, a measure of global cognitive function15), the Hopkins Vocabulary Learning Test (HVLT, a measure of verbal episodic memory16 17) and the Digit Span Test (DST, a measure of short-term rote memory (DST forward) and working memory (DST backward)).18 Cognitive assessments were administered by trained psychologists, who received standard training before the study and achieved the same evaluation level.
Tea consumption and potential study covariates
Being a tea drinker (vs non-tea drinker) was operationalised as drinking tea (green, oolong or black) more than three times a week, for at least 6 months. Participants also responded to questions pertaining to demographic characteristics (age, sex, years of education), medical history (diagnosed hypertension, heart disease, hyperlipidemia), smoking history (defined as currently smoking or cumulative smoking over 6 months at any point during the lifespan) and history of alcohol intake (defined as alcohol consumption of more than 20 g/day on average over 6 months).
Statistical analyses
Data distribution met the assumptions of normality. Between-group differences between tea and non-tea consumers were assessed for all demographic and health-related variables for the entire sample (the CH group and the MCI group). Age, sex and education were considered a priori covariates. Other variables with significant differences between tea consumers and non-tea consumers were treated as additional covariates in subsequent analyses (ie, fully adjusted models).
To examine the association between tea consumption and cognitive function, independent analyses of covariance were conducted for each of the cognitive performance scores. Analyses were first conducted for the entire sample and then for each of the cognitive status groups.
All statistical analyses were conducted using IBM SPSS Statistics for Windows, V.23.0. The significance level was set as p<0.05 for two-tailed tests.
Results
Participant characteristics by cognitive status
Within a sample of 1849 participants, 1033 were categorised as CH and 816 were categorised as MCI. Of the study sample, 65.6% was female, with a mean age of 69.50 (8.02) years. As expected, compared with the CH group, the MCI group was significantly older (70.25 (8.48) years vs 68.90 (7.60) years, t=3.567, p<0.001), reported fewer years of education (9.65 (4.04) years vs 11.12 (3.37) years, t=−8.350, p<0.001) and were less likely to be tea consumers (41.3% vs 47.1%, χ2=6.099, p=0.014). Groups did not differ with respect to sex, smoking or alcohol history (p value ranged from 0.081 to 0.794). Compared with CH participants, MCI participants were more likely to report a history of heart disease (22.9% vs 17.2%, χ2=7.967, p=0.005) and were less likely to report a history of hyperlipemia (37.6% vs 45.0%, χ2=8.572, p=0.003). Groups did not differ for self-reported hypertension or diabetes (p value ranged from 0.114 to 0.136). As expected, the MCI group performed more poorly on all cognitive tests compared with the CH group (table 1).
Demographic and cognitive function of the participants
Participant characteristics by tea consumption
Of the 823 participants who were labelled as tea consumers, as displayed in table 2, tea drinkers were more likely to be male, to report more years of education, and to report a history of smoking and alcohol intake. These between-group differences were found in the entire sample and in each of the cognitive status groups. Self-reported heart disease was more common among non-tea drinkers, relative to tea drinkers; however, this difference was restricted to the CH group. Scores of cognitive tests were generally higher among tea drinkers relative to non-tea drinkers (table 2).
Sample characteristics by tea consumption and cognitive status
Association between tea consumption and cognitive function within the entire sample
Controlling for age, sex and education, analyses of covariance (ANCOVAs) revealed a statistically significant association between tea consumption and HVLT total (F(1, 1844)=10.65, p=0.001, ηp2=0.006) and delayed recall score (F(1, 1841)=4.36, p=0.037, ηp2=0.002) within the entire sample. The results did not change in the fully adjusted model for HVLT total or delayed recall score. The association between tea consumption and DST forward was trending in the initial adjusted model (F(1, 1841)=3.26, p=0.071, ηp2=0.002) and reached statistical significance in the fully adjusted model (F(1, 1540)=4.65, p=0.031, ηp2=0.003). No significant associations were found for performance on the MoCA or DST backward (table 3).
Analyses of covariance examining the association between tea consumption and cognitive function
Association between tea consumption and cognitive function by cognitive status
Controlling for age, sex and education, ANCOVAs revealed significant associations between tea consumption and HVLT total (F(1, 1028)=10.51, p=0.001, ηp2=0.01) and delayed recall score (F(1, 1026)=6.39, p=0.012, ηp2=0.006) within the CH group, but not the MCI group (p=0.330 and p=0.928, respectively). The findings did not significantly change in the fully adjusted models. The association between tea consumption and DST forward was trending in the initial adjusted model for the CH group (F(1, 1026)=3.10, p=0.078, ηp2=0.003), and reached statistical significance in the fully adjusted model (F(1, 1026)=4.47, p=0.035, ηp2=0.005). No additional associations were found in the CH group or the MCI group (table 3)
Discussion
Main findings
A body of research suggests that tea consumption is a modifiable lifestyle behaviour that may decrease the risk of cognitive impairment and dementia in later adulthood. Few studies have examined the benefit of tea consumption on specific domains of cognitive function and there is a paucity of research that has examined the relative benefit of tea consumption on cognitive performance among cognitively healthy and cognitively impaired older adults. The current study addressed this gap in knowledge by examining the relative benefit of tea consumption for cognitive function in healthy non-demented older adults and older adults with MCI.
The current study suggests that the benefit of tea consumption is relatively small, and that this benefit is restricted to cognitively healthy older adults, and does not extend to older adults with MCI. This finding is novel because it is the first study to examine the association between tea consumption and cognitive performance in cognitively healthy and cognitively impaired older adults separately. These results further call to question the benefits of tea consumption once cognitive impairment is expressed through standardised neurocognitive testing. However, it is also important to recognise that MCI participants were less likely to be tea consumers relative to the cognitively healthy group.
Similar to findings reported by Feng et al,13 tea consumption among cognitively healthy older adults was associated with better performance on tasks of episodic memory (HVLT) and short-term memory (DST forward). However, in contrast to Feng et al,13 no significant relationship was observed for executive functioning (DST backward) or global cognitive function (MoCA). Conflicting findings may be attributed to the age of the analytical sample, with the current sample being older (on average 69 years of age relative to 64 years of age). Conflicting results may also be attributed to the discrepancy in categorisation of tea consumption. Rather than dichotomising non-tea consumers and tea consumers (ie, consumption of three or more cups of tea per day), Feng et al13 created an ordinal variable according to frequency of tea drinking, with three or more cups per day as the maximum consumption. Despite differences in statistically significant associations, both studies reported a small effect of tea consumption on tests of memory. Although Feng et al13 speculated that the small effect was due to sample characteristics, namely that the sample was high functioning, the current study does not support this conclusion.
The current results suggest that tests of short and delayed verbal memory, which are hippocampal dependent, are more sensitive to the benefits of tea consumption. Within the current study, it is plausible that the association between tea consumption and tests of memory were not significant as the hippocampus is a primary structure that is compromised in persons with MCI and dementia.19 While a research has shown that tea consumption can delay the onset of MCI and dementia,11 it may be surmised that once neural pathology is present, the benefit of tea consumption is void. Indeed, in a placebo-controlled study by Ide et al,20 12 months of green tea consumption (relative to placebo powder) failed to improve cognitive function among older adults with cognitive impairment, despite improvements in biomarkers of oxidative stress. While in healthy older adults, a placebo-controlled study by Lianghui et al21 showed that treatment with Shentai Tea Polyphenol (Jendari) capsules over a 90-day period improved memory, language and executive function, relative to controls.
The current study contributes to the growing body of literature that examines the benefits of tea consumption on cognitive health in late life by examining this association in cognitively healthy and cognitively impaired older adults.
Limitations
Results from this study must be considered in light of several study limitations. The first limitation pertains to quantifying tea consumption and the type of tea consumed. A dichotomous measurement was used, with tea consumption defined as persons who consumed three or more cups of tea per day over the last 6 months. Unfortunately, this study did not quantify intake in millilitres per day of tea or strength of the brew (ie, dilution). A research suggests that tea consumption may have a dose-response effect, with the greatest benefit observed for 500 mL/day of tea consumption.11 Further, while a majority of participants reported the consumption of green tea (65.81%), approximately 27% consumed a combination of green, black and/or oolong tea, which differed in level of fermentation, and their neuroprotective properties. As such, the neuroprotective mechanisms remain unclear. The second study limitation pertains to the cross-sectional evaluation, which precludes causal statements in the association between tea consumption and cognitive functioning.
Implications
This is the first study to examine the association between tea consumption and cognitive performance on tests of memory and executive function in cognitively healthy and older adults with MCI. Although previous researches suggest that tea consumption may delay the onset of MCI and dementia, the current study findings suggest that the benefit of tea consumption may be negated once pathological impairment exists. These findings further suggest that the relative benefit of tea consumption on cognitive function is small and thus must be considered in combination with other lifestyle behaviours, including dietary pattern intake and physical activity, to ensure optimal cognitive function in late life.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics statements
References
Dr. Hua Xu has been working as a psychiatrist in Shanghai Mental Health Center in China since 2001. She got her PhD degree from Shanghai Jiao Tong University School of Medicine, Shanghai, China in 2018. She then worked as a postdoctoral fellow at the Faculty of Education and Medicine in the University of Ottawa, Canada in 2019. Her main research area is geriatric psychiatry, including cognitive impairment and late-life depression.

Footnotes
HX and AJF are joint first authors.
GL and SX contributed equally.
Contributors HX, AJF and XL drafted the manuscript. AJF and HX conducted the statistical analyses. TW and GL were responsible for case diagnosis and data collection. SX oversaw the research study. All authors reviewed the final manuscript.
Funding This work was supported by the Science and Technology Commission of Shanghai Municipality (grant number 18411961500, 19MC1911100), Shanghai Health Committee (grant number 202040366), the Shanghai Mental Health Center (grant number 2017-YJ-12, CRC2017ZD02), Shanghai Jiao Tong University School of Medicine (15ZH4010), Shanghai Brain Health Foundation (SHBHF2016001) and Shanghai Jiao Tong University School of Medicine and Institute of Neuroscience, Chinese Academy of Sciences (2015NKX003).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.