Article Text

Abstract
Background The internet is an integral part of everyone’s life. College going adolescents are highly vulnerable to the misuse of the internet.
Aims To estimate the pooled prevalence of internet addiction (IA) among college students in India.
Methods Literature databases (PubMed, Web of Science, Scopus, EMBASE, PsycINFO and Google Scholar) were searched for studies assessing IA using the Young Internet Addiction Test (Y-IAT) among adolescents from India, published in the English language up to December 2020. We included studies from 2010 to 2020 as this is the marked era of momentum in wireless internet connectivity in India. The methodological quality of each study was scored, and data were extracted from the published reports. Pooled prevalence was estimated using the fixed-effects model. Publication bias was evaluated using Egger’s test and visual inspection of the symmetry in funnel plots.
Results Fifty studies conducted in 19 states of India estimated the prevalence of IA and the overall prevalence of IA as 19.9% (95% CI: 19.3% to 20.5%) and 40.7% (95% CI: 38.7% to 42.8%) based on the Y-IAT cut-off scores of 50 and 40, respectively. The estimated prevalence of severe IA was significantly higher in the Y-IAT cut-off points of 70 than 80 (12.7% (95% CI: 11.2% to 14.3%) vs 4.6% (95% CI: 4.1% to 5.2%)). The sampling method and quality of included studies had a significant effect on the estimation of prevalence in which studies using non-probability sampling and low risk of bias (total quality score ≥7) reported lower prevalence. The overall quality of evidence was rated as ‘moderate’ based on the Grading of Recommendations Assessment, Development and Evaluation criteria.
Conclusions Our nationally representative data suggest that about 20% to 40% of college students in India are at risk for IA. There is a need for further research in the reconsideration of Y-IAT cut-off points among Indian college students.
PROSPERO registration number CRD42020219511.
- adolescent psychiatry
- behavior
- addictive
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Internet use has evolved into an inseparable routine of human life, and it has revolutionised the world with its infinite possibilities. The use of the internet has transformed the world in terms of information sharing, business opportunities, communication, learning, relationships, socialisation, shopping, entertainment, all now accessible with a single click.1 The internet has become an integral part of life, and currently, India is the second-largest internet user globally. Internet and broadband penetration in India is increasing steadily, with 665.31 million internet users in 2019.2
The use of the internet is highly individualised. The healthy way of using it is to accomplish a planned objective within a reasonable period with no behavioural or intellectual distress. Some individuals succeed in limiting their internet use, whereas others cannot regulate themselves.3 Misuse of the internet has become a health concern worldwide and is growing swiftly and steadily. The field of internet addiction (IA) has experienced significant debates over the years. WHO included internet gaming disorder in the chapter of substance and behavioural addiction in the 11th edition of the International Classification of Diseases and Related Health Problems (ICD-11).4 At present, there are many uncertainties regarding the conceptualisation of IA as a disorder, including internet gaming disorder.5 However, most scholars describe IA as an impulse control disorder characterised by excessive or poorly controlled preoccupations, urges or behaviours regarding computer use and internet access that lead to impairment or distress.6 Multiple scales, questionnaires and instruments are developed over time to measure IA. But the most commonly used reliable scale is the Internet Addiction Test (IAT) developed by Young. The scale consists of 20 items rated on a 5-point Likert scale yielding a total score with a range of 20 to 100.7
The substantial data on the epidemiology of IA are voluminous across the globe. However, there is inconclusive evidence regarding the exact magnitude of the problem because the prevalence varies according to country and study context. A study conducted in six Asian countries reported the prevalence of IA varies from 5% to 21%.8 Even within the same country, there is a marked difference in the prevalence of IA due to diverse screening scales with inconsistent cut-off scores. For example, studies conducted across various parts of the Indian subcontinent revealed variable prevalence estimates of IA among college students (5% to 46.7%).9 IA can reduce the young generation’s productivity and cause cognitive dysfunction, poor academic performance and physical, mental and behavioural disturbances.10 Therefore, it is imperative to estimate IA’s magnitude among Indian college students to obtain accurate epidemiological data to develop different strategies and programmes to intervene in this problem. To the best of our knowledge, no meta-analysis has been conducted to estimate the pooled prevalence of IA among Indian college students. Accordingly, we aimed to estimate the pooled prevalence of IA among Indian college students to provide substantial epidemiological evidence to minimise IA’s catastrophe and facilitate the development of interventions to create productive and responsible citizens.
Methods
Search strategy
This meta-analysis is reported following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist11 and was registered in the PROSPERO database (International Prospective Register of Systematic Reviews) (CRD42020219511). Three investigators (MD, SM, BV) independently searched the following electronic bibliographic databases for studies published up to 31 December 2020: PubMed, Web of Science, Scopus, EMBASE, PsycINFO and Google Scholar. College-based prevalence studies conducted in the Indian setting that estimated IA using the Young Internet Addiction Test (Y-IAT) and published in the English language were evaluated. We included studies from 2010 to 2020 as this is the marked era of momentum in wireless internet connectivity in India.12 Additionally, archives of relevant Indian Journals were reviewed for maximum inclusion of available studies. The cross-references of the identified studies were explored for additional studies. The numerous keywords used in our study across several databases include: epidemiology (MeSH) OR prevalence (MeSH)) AND (internet addiction disorder (MeSH) OR students (MeSH) OR problematic internet use) AND India (MeSH)) AND (students). (online supplemental material 1).
Supplemental material
Inclusion and exclusion criteria
The eligibility criteria of this meta-analysis were based on the PICOS acronym. Population (P): college students attending various professional courses in India (without restriction in the type of professional courses). Professional courses were defined as any academic courses after the 12th standard approved by the Government of India. Intervention/exposure: the excessive use of the internet measured using Y-IAT. Comparison: comparison of self-reported measures of excessive internet use based on Young’s criteria cut-off points 50 (Y-IAT ≥50) and 40 (Y-IAT ≥40). Outcomes: the primary outcome was pooled prevalence rate and severity of IA according to standard cut-off scores of Y-IAT. The related factors such as gender, sampling method, overall methodological quality, professional stream of education and year of publication of included studies that may have an impact on the prevalence of IA were also explored. Study design: observational studies (cross-sectional and cohort studies) conducted among college students attending various professional courses in India. The following studies were excluded: (a) studies that reported IA and were conducted outside of India and (b) epidemiological studies conducted in India with a different population such as school-going adolescents, not mentioning Y-IAT cut-off points or using different screening tools for IA.
Studies selection and data extraction
Two reviewers (JJ, VV) independently assessed and screened the eligibility of studies based on the selection criteria. A list of possible articles was generated, and inconsistencies were resolved by consensus involving a third reviewer (AV). Two investigators (SM, BV) independently appraised the full texts of appropriated records and prepared the preliminary draft of data abstraction. The intellectual revision and verification of data abstraction were carried out by two authors (DK, JJ), and the complete data were arranged based on the following study characteristics: author (year of publication), study setting (state/population), sample size/sampling method, age and prevalence according to the severity of IA and gender respectively.
Quality assessment
Two independent reviewers (MD, VV) employed the ‘JBI Critical Appraisal Checklist for Studies Reporting Prevalence Data’ to assess included studies' methodological quality.13 This checklist has nine criteria with a total quality score ranging from 1 to 9. We classified scores as having high (0 to 3), moderate (4 to 6) and low (7 to 9) risk of bias based on the scoring criteria adopted by an earlier study.14 Discrepancies in the quality scoring of two reviewers were addressed by a third independent reviewer (SS). Any disagreement about the scoring of the included studies' methodological quality was resolved by mutual discussion and reaching a consensus (JJ, AV, MD, VV, SS). The Grading of Recommendations Assessment, Development and Evaluation (GRADE) method was used to evaluate the quality of evidence.15
Statistical methods
The statistical analysis was carried out using the software MetaAnalyst (3.1 beta for windows). Medium heterogeneity between studies was found using I2 and Cochran’s Q statistic (I2=49.1%, Q=99.9, p<0.001), so a fixed effect model was used. Furthermore, I2 was interpreted as zero, low, medium and high heterogeneity with the values of 0%, 25%, 50% and 75%, respectively.16 Moreover, a subgroup analysis (sampling design, gender, the stream of education, severity of addiction, year of publication, methodological quality) and sensitivity analysis were also conducted to address the impact of individual studies. Funnel plot and Egger’s regression tests were used to assess potential publication bias. Egger’s regression test with a p<0.05 was considered as having statistically significant publication bias. Similarly, a two-tailed p<0.05 was considered statistically significant in the entire study. The sources of heterogeneity were explored using meta-regression analysis.
Results
Identification of studies
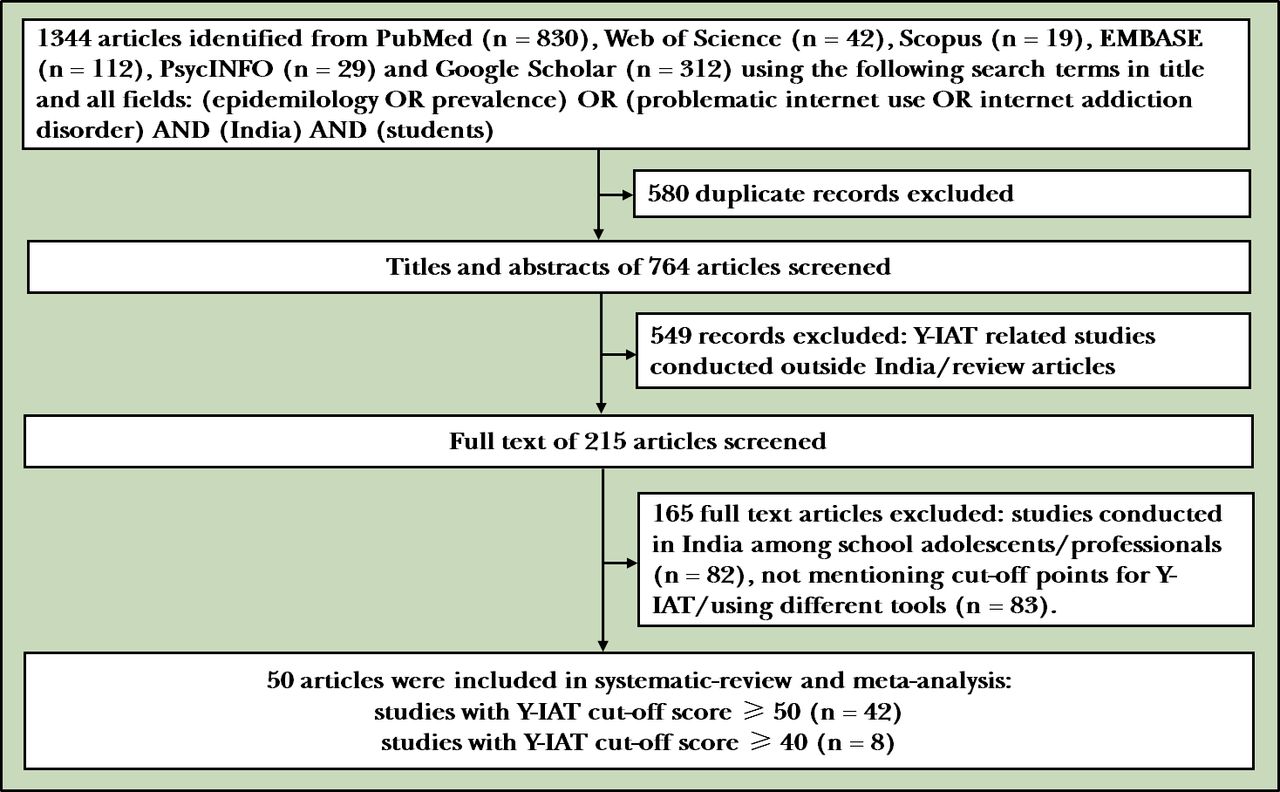
The database search identified 1344 reports: 830 through PubMed, 42 through Web of Science, 19 through Scopus, 112 through EMBASE, 29 through PsycINFO and 312 through Google Scholar. Of these reports, 580 were excluded because they were duplicates. After screening titles and abstracts, another 549 were excluded because they did not meet the selection criteria. The full texts of 215 possibly pertinent records were retrieved for screening, and 165 of these were excluded for the reasons summarised in figure 1. Therefore, 50 eligible articles identified in databases were included in this meta-analysis.

Process of search and selection of studies. Y-IAT, Young Internet Addiction Test.
Characteristics of included studies
A total of 50 studies were included in the systematic review based on Young’s criteria cut-off scores of 50 (Y-IAT ≥50; n=20 901, k=42)17–58 and 40 (Y-IAT ≥40; n=2816, k=8).59–66 The included studies' characteristics are summarised in tables 1 and 2. The sample population covered young adults in the age group 17 to 35 who were pursuing their careers in the medical and engineering science stream (n=15 262, k=39) and allied courses such as basic Science and arts stream (n=8455, k=11). Comprehensive coverage was made possible by the inclusion of studies from 19 states and 1 union territory of India with an adequate representation from different regions: South (k=20), North (k=12), North-East (k=1), Central (k=4), East (k=4) and West (k=10). Convenience sampling designs were used in most of the reports (k=32) compared with probability sampling methods (k=18). The included studies estimated IA’s severity using different cut-off points such as 40, 50, 70 and 80. Therefore, summary estimates of the addiction’s severity, namely moderate and severe IA, were separately extracted according to cut-off points. Most of the included studies investigated the prevalence with a Y-IAT cut-off score of 50 in which the highest and lowest prevalence for moderate and severe addiction were reported at 48.2%, 7.4% and 39.5%, 0.3%, respectively.19 38 51 57 The gender prevalence for IA has also been identified to have an in-depth understanding. A relative proportion of males (n=5442) and females (n=5902) were found in 28 studies. Wide variations were observed in the individual studies on IA’s prevalence among males ranging from 2.2%38 to 67.7%20 and females ranging from 3.3%58 to 43.8%.23
Description of studies measuring prevalence of internet addiction among college students in India based on the Y-IAT (Y-IAT ≥50)
Description of studies measuring prevalence of internet addiction among college students in India based on the Y-IAT (Y-IAT≥40)
Prevalence of IA among college students in India
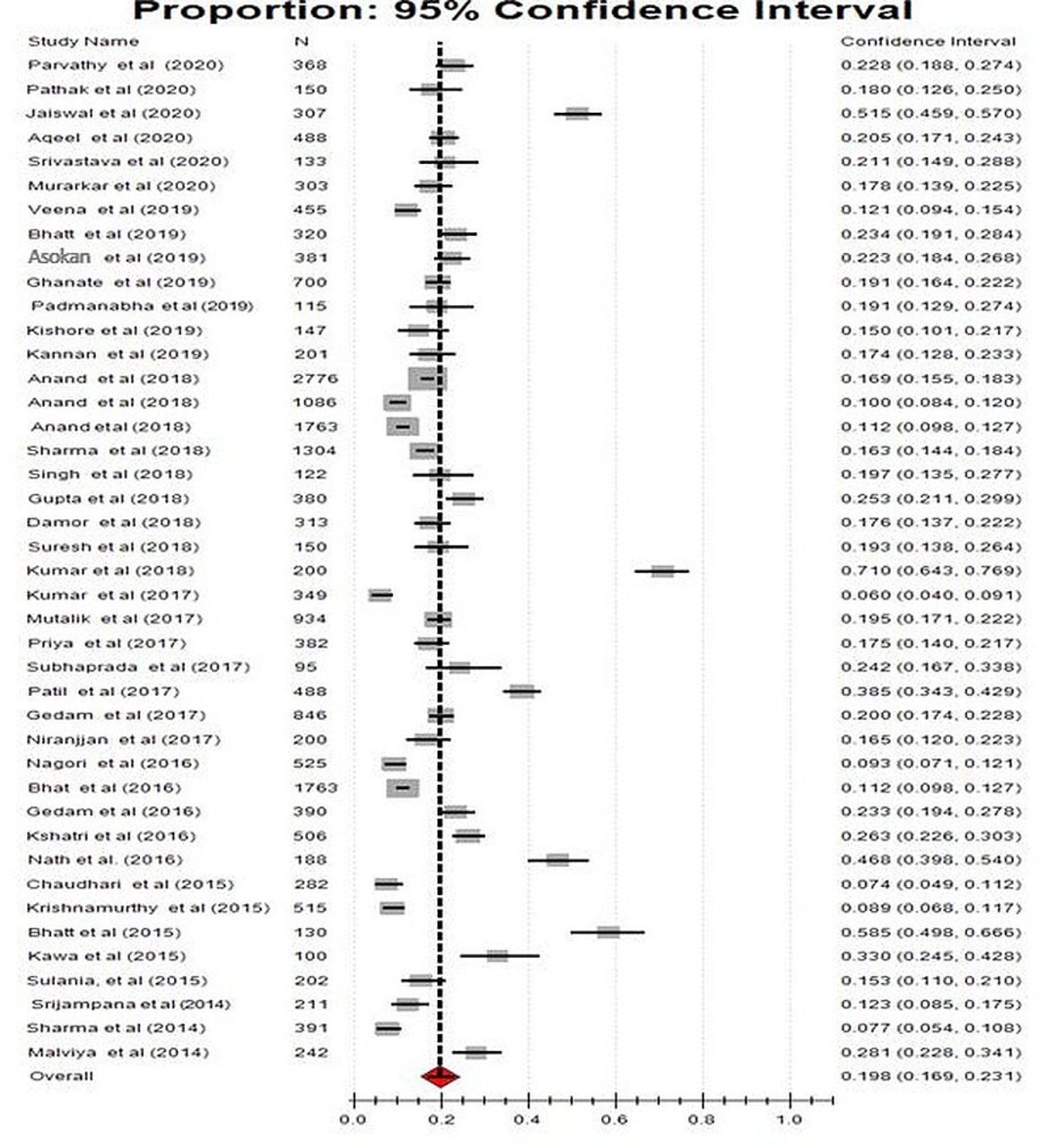
We used a fixed-effects inverse variance model to estimate the pooled prevalence of IA among young adults as there existed mild heterogeneity between studies (Y-IAT ≥50—I2=49.1%, Q=99.9, p<0.001, Tau squared=28.6; Y-IAT ≥40—I2=49.7%, Q=99.8, p<0.001, Tau squared=55.7). The overall prevalence of IA was 19.9% (95% CI: 19.3% to 20.5%; figure 2) and 40.7% (95% CI: 38.7% to 42.8% (online supplemental material 2) based on Y-IAT cut-off scores of 50 and 40, respectively. Furthermore, moderate IA prevalence ranged from 17.6% (Y-IAT 50–79) to 34.2% (Y-IAT 40–69). The estimated prevalence of severe IA was significantly higher in the Y-IAT cut-off points of 70 than 80 (12.7% (95% CI: 11.2% to 14.3%) vs 4.6% (95% CI: 4.1% to 5.2%)).

{kind=link}
{kind=link}
Pooled prevalence of IA among college students (Y-IAT≥50). Y-IAT, Young Internet Addiction Test.
The quality assessment of the studies (k=50) is summarised in online supplemental material 3. The included studies in the meta-analysis were found to have a low (k=26) or moderate (k=24) risk of bias. The quality score ranged from 4 to 9 with a median value of 7 and a mean of 6.72. The overall quality of evidence was rated as ‘moderate’ based on the following criteria GRADE assessment (online supplemental material 4). (a) Risk of bias was evaluated based on Joanna Briggs Institute (JBI) critical appraisal checklist for studies reporting prevalence data. The median and mean score was 7 and 6.72, respectively, in which the total score was ranging from 1 to 9. Therefore, no serious risk of bias was identified. (b) Inconsistency: no serious inconsistency in results was noted as the I2 value was less than 50%. (c) Indirectness: approximately 60% of the studies had an adequate sample frame to address the target population. Therefore, no serious indirectness in the outcome measure was identified. (d) Imprecision: there was a wide CI around the pooled prevalence estimate based on IAT cut-off scores. (e) Publication bias: non-significant p value (0.44) in Eggers’s test was found and a reasonable symmetry of the funnel plot revealed no publication bias (online supplemental material 5).
Sensitivity analysis
Leave-one-out sensitivity analysis was performed to address the possible impact of any particular study on the aggregate pooled effect. There was no significant influence of any specific study on the overall prevalence of adult IA (19.9%), and the values ranged from 19.3% (18.7% to 19.9%) to 20.7% (20% to 21.3%).
Subgroup analysis
Except for the eight studies that used the cut-off score of 40, all the remaining studies (k=42) in this review evaluated IA by using the Y-IAT cut-off point of 50. Therefore, 42 studies and the 8 studies were subjected to subgroup analysis separately based on different variables such as the severity of the addiction, gender, sampling methods, stream of education, quality scoring and year of publication. Subgroup analyses of the severity of addiction were separately done based on the Y-IAT cut-offs of both 40 and 50. Almost all the variables demonstrated significant differences in prevalence rates between the subgroups. Concerning gender, males had a significantly higher prevalence rate for IA as compared with females based on both Y-IAT cut-offs at 40 and 50 (Y-IAT ≥50: 32.5% vs 20.2%; Y-IAT ≥40: 56.8% vs 48.9%). No statistically significant difference was observed in the prevalence of IA based on the stream of education in the Y-IAT cut-off score of 50 (p=0.542). However, students in the medical and engineering stream had a lower prevalence of IA (29.5%) than students who were enrolled in other streams (53.6%) based on the Y-IAT cut-off score of 40. Methodological aspects of the studies, especially the sampling designs, affected the prevalence. The overall prevalence among the studies that used probability sampling was relatively higher as compared with those that used non-probability sampling (Y-IAT ≥50: 22.5% vs 18.2%; Y-IAT ≥40: 44.7% vs 33.1%). All the included studies that used a Y-IAT cut-off score of 40 (n=8) were conducted from 2018 to 2020. Therefore, subgroup analysis based on the period of publication was restricted to studies with Y-IAT ≥50 which revealed a pooled prevalence of 19.9%. (table 3).
Subgroup analysis of Internet addiction (Y-IAT ≥50 & Y-IAT ≥40, respectively) based on the fixed effect model
Meta-regression analysis
The sources of heterogeneity might be the systematic differences between included studies, in terms of cut-off scores of measuring instruments and inclusion/exclusion criteria. Meta-regression analysis was separately done for studies based on Y-IAT cut-off scores of 50 and 40. The results indicated that methodological quality and publication year did not contribute to heterogeneity (online supplemental material 6).
Discussion
Main findings
Fifty studies conducted in 19 states of India estimated the overall prevalence of IA as 19.9% (95% CI: 19.3% to 20.5%) and 40.7% (95% CI: 38.7% to 42.8%) based on Y-IAT cut-off scores of 50 and 40, respectively. The heterogeneity level was mild (I2=49.1%), and most of the included studies had a low risk of bias in terms of methodological quality. Exclusion of any specific study did not affect the overall prevalence in which the values ranged from 19.3% (18.7% to 19.9%) to 20.7% (20% to 21.3%). This pooled estimate of IA in Indian college students is higher than the findings of the two meta-analyses of similar studies conducted in China (11%).67 68 There was a significant difference in prevalence of IA severity based on Y-IAT cut-off points. Moderate IA ranged from 17.6% (Y-IAT 50–79) to 34.2% (Y-IAT 40–69) and severe IA was significantly higher with Y-IAT cut-off points of 70 than 80 (12.7% (95% CI: 11.2% to 14.3%) vs 4.6% (95% CI: 4.1% to 5.2%)). We detected that the pooled prevalence was lower among females, which was similar to the estimates of some of the observational studies69 70 and a meta-analysis.71 Similar findings were also reported in a study conducted in the Indian context.72 The sampling method and quality of included studies had a significant effect on the estimate of prevalence. In general, studies using convenience sampling and low risk of bias (Y-IAT ≥7) reported lower prevalence regardless of the cut-off point of Y-IAT.
The current meta-analysis observed that about 20% to 40% of college students in India are at risk for IA. Y-IAT is a screening instrument and does not diagnose IA, which further adds some possible explanations to our findings. First, the estimated prevalence of IA varies with screening criteria. Studies conducted worldwide have also reported a wide variation in the prevalence of IA among college students. Our findings are comparable to the magnitudes of IA reported in observational studies from Nigeria (20.1%),73 Lebanon (16.8%)74 and Japan (15.0%)75 but higher than the prevalence figures from Spain (6.08%),76 China (6%)77 and lower than those reported from Iran (34.6%),78 Malaysia (36.9%)79 and Jordan (40.0%)80 . Second, the standardisation of the cut-off scores of the screening tool is essential for the exact evaluation of the magnitude of IA in this setting. The present study findings are based on measuring a single standard screening instrument (Y-IAT) with different cut-off points. Y-IAT is a screening instrument, and there is scanty evidences regarding its diagnostic validity across the world. The overall prevalence of 19.9% (Y-IAT ≥50) in this meta-analysis is consistent with some of the previous studies with similar cut-off points conducted in Lebanon (16.8%)74 but lower than those found in Ethiopia (29.4%).81 In subgroup analyses, the pooled prevalence of severe IA was 4.6% and 12.7% based on the Y-IAT cut-off scores of 80 and 70. Interestingly, these significant differences in prevalence estimates were also observed in IA’s moderate category based on the Y-IAT cut-off scores of 50 and 40 (17.6% vs 34.2%). Taken together, all these results further support the need for further research in the reconsideration of cut-off points of Y-IAT among Indian college students.
Implications
The use of the internet is rampant in India, and we found that the overall prevalence of IA among college students was as high as 40.7% based on the Y-IAT cut-off score of 40. Our findings open an area of discussion for placing greater attention on internet usage in young adults, justifying the increased investment in their mental health. India is one of the youngest populations globally, and this population is extremely vulnerable to IA, necessitating appropriate intervention strategies. Although WHO has given recommendations for the duration of screen use for different age groups, there are no specific recommendations from the government of India. In general, there is a lack of awareness about the WHO recommendations, and children are allowed to use the screen and internet from a very young age, as young as infants. Parents are not aware of the deleterious effect of the excessive early use of screens and the internet, and it is fashionable to allow children to use the internet at a very early age. If one considers the increasing trend of IA in the recent years, the high prevalence of IA in adolescents and young adults seen in the present meta-analysis suggests that there is a need to develop a national policy for the use of the internet among the young children, adolescents and young adults. If this is not addressed as a priority, the country must anticipate a large population dependent on the internet, requiring medical attention. There is a need to reorientate the existing mental health services to address this behavioural addiction through internet deaddiction centres.
Strength and limitations
This is the first meta-analysis evaluating the pooled prevalence of IA in Indian college students to the best of our knowledge. Most of the included studies were rated as moderate quality, and the studies covered in this meta-analysis were conducted in different geographic areas of India, which made the sample representative of Indian college students. Heterogeneity is a common pitfall in the meta-analysis of epidemiological studies. However, no serious heterogeneity in results was noted in the current meta-analysis as the I2 value was less than 50%. However, there are some limitations. Although IA’s assessment was based on the Y-IAT tool, the diagnosis was not confirmed in any of the studies. Factors that may influence the prevalence of IA were not examined due to the paucity of such data. Most of the included studies used the convenience sampling method. These could be confounding factors to affect the judgement of the results.
Conclusions
Our nationally representative data suggest that about 20% to 40% of college students in India are at risk for IA. The standardisation of the cut-off scores of Y-IAT is essential for accurately evaluating the magnitude of IA in this setting. The use of the internet is rampant in India, and our findings of the high prevalence of IA in young adults justify increased investment in their mental health, including the development of a national policy. There is a need to reorientate the existing mental health services to address IA by establishing internet deaddiction centres or clinics.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
References
Jaison Joseph obtained a bachelor’s degree from Rajiv Gandhi University of Health Sciences, Karnataka, India in 2009 and postgraduate degree in Psychiatric Nursing from Post Graduate Institute of Medical Education and Research (PGIMER) in India. Currently, he is working as a faculty member in College of Nursing, Pt. BDS University of Health Sciences, Rohtak, India. He is pursuing a PhD degree at Rajiv Gandhi University of Health Sciences, Karnataka, India. His main research interest includes epidemiology and treatment aspects of mental illnesses.

Abin Varghese obtained a bachelor's degree from Mahatma Gandhi University, India, in 2008 and a master's degree in Psychiatric Nursing from All India Institute of Medical Sciences, New Delhi, India. Since then he has been working as a tutor/clinical instructor at the school of nursing under Indian Council of Medical Research, Bhopal, Madhya Pradesh, India. He is pursuing a PhD degree at Rajiv Gandhi University of Health Sciences, Karnataka, India. His main research interest includes aggression and addiction.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
JJ and AV are joint first authors.
JJ and AV contributed equally.
Contributors JJ: study conception, preparation of preliminary and final chapters according to PRISMA checklist and preparation of data extraction table. AV: preparation of meta-analysis and results, methodological quality assessment scoring—selection of assessment criteria. VVR: methodological quality assessment and scoring, screening for related studies. MD: methodological quality assessment and scoring, searching for related studies according to search strategy (database searching), preparation of meta-analysis. SG: intellectual revision of final chapters according to PRISMA checklist. SS: intellectual revision of methodologic quality assessment scoring (third independent reviewer). DK: intellectual revision and verification of final data extraction table. SM: searching for related studies and preliminary data extraction. BPV: screening for related studies and preliminary data extraction.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.