Article Text

Abstract
Background Caregivers play a pivotal role in providing care for mentally ill patients. Increase in caregiver burden can make them vulnerable to mental illness themselves.
Aims We assessed the severity of burden of care and its association with depression, anxiety and quality of life among caregivers of patients with alcohol use disorder (AUD) and schizophrenia.
Methods This was an observational, cross-sectional, single-centred study of 50 consecutive caregivers of patients with AUD and schizophrenia. Participants were recruited from the psychiatry outpatient department of a tertiary care hospital between January and June 2017. The caregivers were further assessed by demographic details, Hospital Anxiety Depression Scale for assessment of depression and anxiety, Zarit Burden Interview for assessment of caregiver burden and WHO Quality Of Life-BREF for assessment of quality of life. Statistical data were analysed using GraphPad InStat V.3.06 (California). Multiple linear regression analysis was applied to identify the predictors of caregiver burden.
Results Burden of care experienced by caregivers of patients with AUD is as high as that of caregivers of patients with schizophrenia (U=1142.5, p=0.46). Caregivers experiencing high burden of care are likely to have symptoms of anxiety (U=22, p<0.001), depression (U=32, p<0.001) and poor quality of life (U=84.5, p<0.001). Female caregivers are likely to experience higher burden of care (U=819.5, p=0.006). For caregivers of patients with schizophrenia, anxiety, environmental health, socioeconomic status and patients’ occupation can predict burden of care, while for caregivers of patients with AUD, depression and environmental health can predict burden of care.
Conclusion Our study suggests that caregivers of patients with AUD experience burden of care as high as that of caregivers of patients with schizophrenia. Caregivers with high burden of care are more likely to have depression, anxiety and poor quality of life.
Trial registration number CTRI/2017/03/008224.
- alcohol drinking
- schizophrenia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Family is the basic unit of the society and is extensively involved in the well-being of kith and kin.1 With the alarming rise in the incidence of mental illness across the globe, there is a proportionate rise in the burden of care among caregivers of those who are mentally ill. Aside from providing help with activities of daily living, families also provide emotional, social and financial support to individuals with mental illness.2 3 Being the first ones to come in contact with the person with mental illness, family members also have to face the stigma, shame and prejudice from the society. Chronic mental illness in one family member may paralyse the life of others in the family and restrict their avenues for leisure, socialisation and employment. This puts them at greater risk of suffering from mental illness.3 4
Alcohol use disorder (AUD) is a group of behavioural and physical symptoms that can include withdrawal, tolerance and craving.5 Often considered a family disease, AUD also takes a toll on the lives of family members.6 The increase in unpredictable and unreliable behaviour in individuals with AUD translates into stress and strain in caregivers.7 This leads to defective coping and increases their vulnerability to mental illness.8 Family bears the brunt of domestic violence of all forms, that is, physical, verbal and sexual.9 Low marital satisfaction, poverty and embarrassment are other impediments to the well-being of caregivers. This ultimately pushes the family to penury.10
Schizophrenia refers to the dysfunction in cognitive, behavioural and emotional domain,5 and is an extremely damaging disorder that leads to long-term disability. It onerously affects family members.11 Caregiving restricts family members’ freedom, personal space and social activities. Encouragement of deinstitutionalisation in mental health policies leads the family to being caught unprepared to take care of members with schizophrenia, which in turn increases their burden.9 Studies conducted previously have reported an increase in the incidence of depression, anxiety and stress among caregivers of individuals with schizophrenia.12 13
The dearth of data comparing the burden of care among caregivers of individuals with AUD and schizophrenia led us to pursue this study. Our study aims to assess the severity of burden of care and its association with depression, anxiety and quality of life among caregivers of individuals with schizophrenia and AUD.
Materials and methods
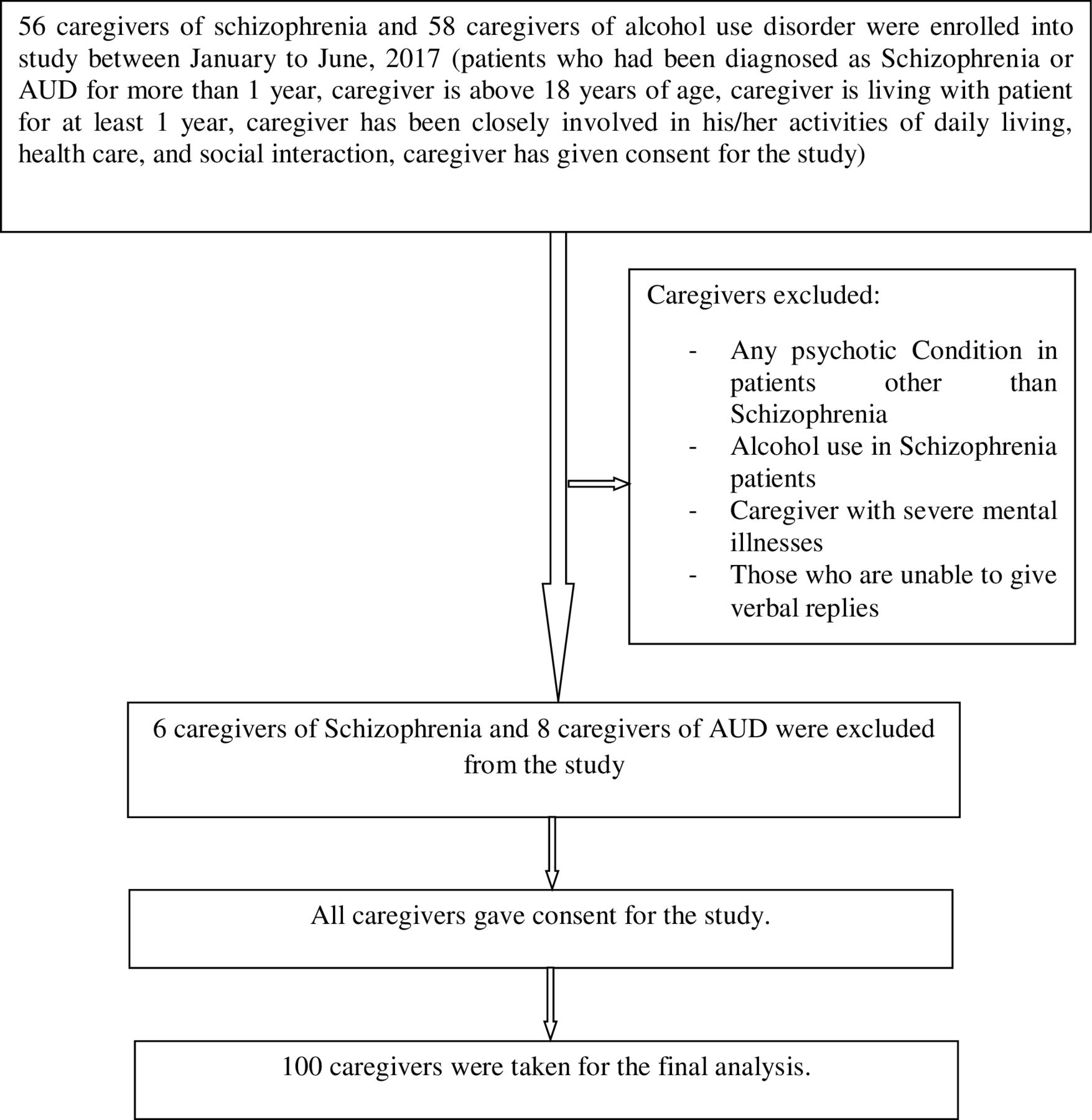
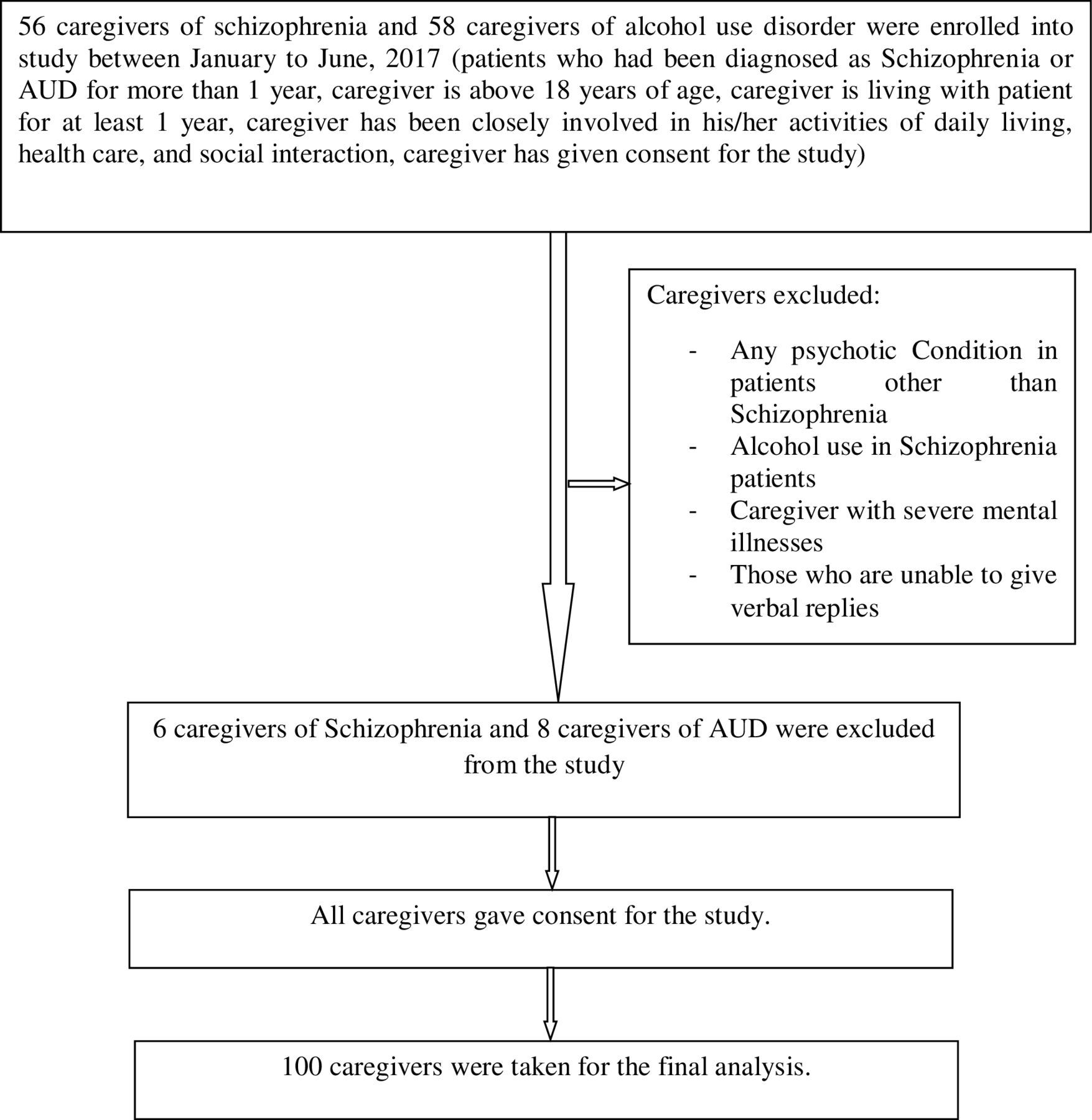
This is an observational, cross-sectional, single-centred study. Schizophrenia and AUD were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders-5. Fifty consecutive caregivers of patients with schizophrenia and AUD were recruited from the psychiatry outpatient department of a tertiary care hospital between January and June 2017. Patients who had been diagnosed with schizophrenia or AUD for more than 1 year, caregivers older than 18 years, caregivers living with the patient for at least 1 year before recruitment to this study, caregivers who have been closely involved in patients’ activities of daily living, healthcare and social interaction, and those who provided consent to participate in the study, were included. Any psychotic condition other than schizophrenia, alcohol use in patients with schizophrenia, caregivers with severe mental illnesses, such as schizophrenia or bipolar mood disorder, those unable to give verbal replies, and those who do not give consent to participate in the study, were excluded. The purpose of the study was explained to the participants and written informed consent was obtained from them. The pro forma for participants contained patients’ and caregivers’ demographic details, the Hospital Anxiety Depression Scale (HADS), Zarit Burden Interview (ZBI) and WHO Quality of Life-BREF (WHOQOL-BREF) scales to be applied to caregivers. Interview with the participants was done in their vernacular language. Caregivers were interviewed separately from the patients to increase comfort and avoid any bias due to the presence of patients. Maintenance of anonymity and confidentiality of participants was ensured. Figure 1 depicts the flowchart of the study method.
{kind=link}
Flowchart of the study method. AUD, alcohol use disorder.
The HADS is a 14-item, 4-point Likert scale designed to assess anxiety and depression in a hospital setting. It comprises two subscales, each containing seven questions to assess anxiety and depression, respectively. It measures symptoms over the past 1 week and contains both positively and negatively constructed items. The even-numbered items measure depression, while the odd-numbered items measure anxiety. The responses for each question range from 0 to 4. The total possible score ranges from 0 to 21 for each subscale. Higher scores on each subscale suggest more severe symptoms. A total subscale score of 0–7 denotes no symptoms, 8–10 denotes borderline abnormal case, and 11–21 denotes abnormal case of depression or anxiety. A cut-off score of 8 denotes abnormal case. The HADS shows good internal reliability, test–retest reliability, concurrent validity, sensitivity and specificity.14 In the present study, it has a Cronbach’s alpha coefficient of 0.977.
The ZBI is a 22-item, 5-point Likert scale developed by Zarit et al 15 to measure the burden of care experienced by caregivers of individuals with mental illness. The responses for each question range from 0 (never) to 4 (nearly always). The total possible score ranges from 0 to 88. Higher scores on the scale denote higher burden of care experienced by caregivers of individuals with mental illness. A total score of 0–20 represents little or no burden, 21–40 represents mild to moderate burden, 41–60 represents moderate to severe burden and 61–88 represents severe burden. The ZBI has been found to have good internal consistency, construct validity and test–retest reliability.15 In the present study, it has a Cronbach’s alpha coefficient of 0.978. A cut-off score of 40 was used to distinguish between low burden and high burden following recommendations of an earlier study.16
The WHOQOL-BREF questionnaire is a 26-item, 5-point Likert scale developed by the WHO to assess quality of life over the past 2 weeks. It assesses quality of life in four domains: physical health (seven items), psychological health (six items), social relationships (three items) and environmental health (eight items). It also consists of two other items for overall quality of life and general health. Each item on the scale is rated from 1 to 5; scores of items for each domain are summed up to determine a raw score for each domain. Higher scores on the scale are indicative of higher quality of life. The WHOQOL-BREF domain scores demonstrate good discriminant validity, content validity, internal consistency and test-retest reliability.17 In the present study, it has a Cronbach’s alpha coefficient of 0.980.
Statistical analysis
Qualitative data are expressed as percentages, while quantitative data are expressed as mean (SD). Proportions of participants were compared using the χ2 test. The Kolmogorov-Smirnov normality test was applied. Scores on HADS, ZBI and WHOQOL-BREF scales that followed normality test were compared using Student’s two-tailed t-test, while scores that did not follow normality test were compared using Mann-Whitney test. Statistical analysis was done using GraphPad InStat V.3.06 (San Diego, California, USA). Multiple linear regression analysis was applied to identify the predictors of caregiver burden. Here, the ZBI score was taken as the outcome variable, and the anxiety and depression subscale scores of HADS, domain scores of WHOQOL-BREF and the demographic variables as predictor variables. A p value ≤0.05 was considered statistically significant.
Results
Demographic characteristics
The demographic characteristics of caregivers and patients with schizophrenia and AUD are shown in table 1.
Demographic characteristics and other factors of caregivers and patients with schizophrenia and AUD.
The mean duration of illness was longer in patients with AUD than in patients with schizophrenia, while the mean duration of treatment was longer in patients with schizophrenia than in patients with AUD. Hence, these two variables were not comparable.
Few caregivers of patients with AUD and schizophrenia suffered from adjustment disorder or anxiety disorder.
Level of burden of care and its association with other variables
Table 2 shows that caregivers of individuals with AUD with high burden of care are likely to have higher scores in the depression subscale (U=48, p<0.001) and anxiety subscale (U=36, p<0.001) of HADS, and lower scores in the physical health domain (U=129.5, p=0.002), psychological health domain (U=104, p<0.001), social relationships domain (U=141, p=0.004) and environmental health domain (U=88, p<0.001). Caregivers of individuals with schizophrenia with high burden of care are likely to have higher scores in the depression subscale (U=32, p<0.001) and anxiety subscale (U=22, p<0.001) of HADS, and lower scores in the physical health domain (U=84.5, p<0.001), psychological health domain (U=68.5, p<0.001), social relationships domain (U=115, p<0.001) and environmental health domain (U=45.5, p<0.001).
Comparison of HADS and WHOQOL-BREF scores between caregivers with high burden and low burden of care of patients with alcohol use disorder and schizophrenia.
Comparison of variables between schizophrenia and AUD
As shown in table 3, there was no statistical difference in scores on ZBI (U=1142.5, p=0.46), depression (U=973, p=0.056) and anxiety (U=1087, p=0.26) subscales of HADS, and all domains of WHOQOL-BREF between caregivers of patients with schizophrenia and AUD.
Results of comparison of HADS, ZBI and WHOQOL-BREF scores between schizophrenia and alcohol use disorder groups.
Effect of gender on burden of care and other variables
Table 4 shows that female caregivers of patients with AUD are likely to have higher scores on the ZBI scale (t=2.42, p=0.01) and on the anxiety subscale of HADS (t=2.52, p=0.01), and lower scores on the physical health domain (t=3.21, p=0.002), psychological health domain (t=3.44, p=0.001), social relationships domain (U=128, p=0.04) and environmental health domain (t=4.43, p<0.001). Female caregivers of patients with schizophrenia are likely to have higher scores on the ZBI (U=198.5, p=0.04) and the anxiety subscale of HADS (U=183, p=0.02), and lower scores on the environmental health domain (t=2.16, p=0.03).
Comparison of ZBI, HADS and WHOQOL-BREF scores between male and female caregivers of patients with schizophrenia and alcohol use disorder.
Predictors of burden of care
Linear regression analysis was applied to identify the predictors of burden of care using the stepwise technique. All predictors found to be significant in the univariate analysis were then entered into the multivariate analysis. In the present model, ZBI score was considered as the outcome variable.
The multiple regression model for caregivers of individuals with AUD with all predictors produced an adjusted R²=0.784, which stipulates that 78.4% variance in the outcome variable can be explained by the predictors. This model was also significant in prediction (F(2, 48)=90.023, p<0.001). Similarly, the multiple regression model for caregivers of individuals with schizophrenia with all predictors produced an adjusted R²=0.757, which stipulates that 75.7% variance in the outcome variable can be explained by the predictors. This model was significant in the prediction (F(4, 46)=39.151, p<0.001).
For the ZBI score of caregivers of patients with AUD, after two-step linear regression model, depression score on HADS (B=2.780, p<0.001) and environmental health domain score on WHOQOL-BREF (B=−0.224, p=0.008) were found to be significant predictors of burden of care (table 5). For the ZBI score of caregivers of patients with schizophrenia, after four-step linear regression model, anxiety score on HADS (B=2.032, p<0.001), environmental health domain score on WHOQOL-BREF (B=−0.326, p=0.003), socioeconomic status of caregiver (B=0.001, p=0.022) and patients’ occupation (B=−9.009, p=0.024) were found to be significant predictors of burden of care (table 5).
Linear regression analysis of predictors of burden of care in caregivers of individuals with alcohol use disorder and schizophrenia.
As can be seen in table 5, scores on the depression subscale of HADS had positive weightage, so caregivers of individuals with AUD with higher scores on this scale are expected to have higher ZBI score, while scores on the environmental health domain of WHOQOL-BREF had negative weightage in the model, so caregivers of individuals with AUD with low scores on the environmental health domain are expected to have higher ZBI score. Similarly, anxiety score on HADS and the socioeconomic status of caregivers of individuals with schizophrenia had significant positive regression weightage, stipulating that caregivers of individuals with schizophrenia with higher scores on the anxiety subscale of HADS and caregivers of individuals with schizophrenia with higher socioeconomic status are expected to have higher ZBI score. The environmental health domain score of WHOQOL-BREF and patients’ occupation had a significant negative weightage, indicating that caregivers of individuals with schizophrenia with lower scores on the environmental health domain and with unemployed patients are expected to have higher ZBI score.
Depression score on HADS is the strongest predictor of burden of care in caregivers of individuals with AUD (table 5), while unemployed patient with schizophrenia is the strongest predictor of burden of care in caregivers, as can be seen in table 5.
Working model to predict ZBI score for caregivers of individuals with AUD and its application to the next caregiver is as follows:
ZBI score=23.238 + 2.780 (depression score) – 0.224 (environmental health domain score).
Working model to predict ZBI score for caregivers of individuals with schizophrenia and its application to the next caregiver is as follows:
ZBI score=48.159 + 2.032 (anxiety score) – 0.326 (environmental health domain score) + 0.001 (socioeconomic status) – 9.009 (patient’s occupation).
Discussion
Main findings
Our results suggest that caregivers of patients with schizophrenia are likely to experience a significant burden of care. Schizophrenia is a chronic illness, which might hamper the insight of an individual to a great extent. The burden of care in caregivers of patients suffering from schizophrenia may be attributed to the above factors at large. However, several other factors that play an important role in increasing the burden of care include taking care of the patient’s grooming, hygiene, daily needs, medications, and dealing with exacerbation and relapse of illness. This can make the caregiver feel burdened. These findings were corroborated by other studies.18–20
As can be seen in tables 2 and 5, caregivers of patients with schizophrenia with higher burden of care are likely to have depression, anxiety and poor quality of life. Also burden of care in caregivers can be predicted by anxiety and environmental quality of life. This can be because the burden of caring affects caregivers’ ability to cope with illness. Longer duration of illness and caregiving become chronic stressors for caregivers. Social isolation may follow, leading to increased stress and making them vulnerable to depression and anxiety. Moreover, caregivers are flooded with patient and family responsibilities and are burdened with caregiving duties and persistent worries about their patients. This will result in withdrawal from the society and leisure activities, leading to poor quality of life. Similar results were found in previous studies.12 13 21
Table 5 suggests that burden of care in caregivers of patients with schizophrenia can be predicted by the employment status of the patient. A possible explanation for this can be that owing to unemployment, patients and caregivers are forced into a life of penury. They spend more time at home and so caregivers are burdened with caregiving tasks, in comparison with patients who are employed where caregivers get more time of rest and relief while patients are away for work. Monetary scarcity further increases the burden. Our findings were substantiated in earlier studies.4 21–23
Our results show that caregivers of patients with AUD are likely to experience significant burden of care. Repeated quarrels, verbal and physical abuse by the person with AUD, and seclusion of caregivers from other family members and society significantly impact their physical and mental health. These can lead to increased burden in caregivers of patients with AUD. Other studies also showed similar results.24 25
Caregivers of patients with AUD with higher burden of care are likely to have depression and anxiety, and burden of care can be predicted by anxiety (tables 2 and 5). This can be explained on the basis that health-related issues among caregivers themselves, violence committed by the patients, financial crisis, shame and stigma from the society towards alcoholics can lead to depression and anxiety in caregivers. These findings were confirmed in other studies.10 26
Our study suggests that caregivers of patients with AUD are likely to have poor quality of life and that burden of care can be predicted by the environmental domain of quality of life (tables 2 and 5). This can be explained by the fact that AUD in one family member, especially when he/she is the sole breadwinner, may cause myriad problems for the caregivers. Some of these are occupational dysfunction, premature and compulsory retreat from jobs, solitude, changes in responsibilities, disruption of routine and social activities, and financial burden. All these can lead to poor quality of life among caregivers. Similar results were found in other studies.7 27
The results of our study show that there was no statistical difference in the burden of care experienced by caregivers of patients with schizophrenia and AUD (table 3). Caregivers of patients with AUD experience burden of care as high as that of caregivers of patients with schizophrenia. Other studies supported our results.28 29
As can be seen in table 4, female caregivers have higher caregiver burden and anxiety and poor quality of life. This might be due to female caregivers differing in their appraisal and in coping with stressors, and the lack of social support framework that caters to their needs. The sociocultural expectations imposed on them to adopt a caregiving role despite their difficulties add fuel to the fire.4 22 23 Contradictory results were found in a few studies, where male caregivers experienced significant burden of care than female caregivers.28 30
Limitations
Although we have used validated scales of assessment, our study has some limitations, such as its small sample size, being a hospital-based study, participant recruitment from a single centre and being a cross-sectional study, cause-effect relationship cannot be established. The mean duration of illness and the mean duration of treatment were not adjusted in the univariate analysis. We have not taken into consideration the supporting network that our patients and their caregivers might have, which may influence burden of care. Further multicentric cohort studies with large sample size are required to obtain further insights into this subject.
Implications
Psychological problems of caregivers of patients with mental illness are not given enough attention or are ignored. There is a strong need to give proper attention towards caregivers’ mental well-being to prevent mental illness and to identify early those who are at risk.
Conclusion
Caregivers of patients with AUD experience burden of care as high as that of caregivers of patients with schizophrenia. Caregivers with high burden of care are more likely to have depression, anxiety and poor quality of life. Female caregivers are likely to experience higher burden of care. For caregivers of patients with schizophrenia, anxiety, environmental health, socioeconomic status and patients’ occupation can predict burden of care, while for caregivers of patients with AUD, depression and environmental health can predict burden of care.
References
Dr Sneha Vadher completed her MBBS from Govt Medical College, Bhavnagar, India, in 2014. She obtained her degree of MD in Psychiatry from Govt Medical College, Bhavnagar, India, in 2018. She has been working as an assistant professor in the Department of Psychiatry at Pramukhswami Medical College, Karamsad, India, since 2019. Her research interest includes substance use disorder. Currently she is involved in research activity in Social Medial Addiction.

Footnotes
Contributors SV did the planning, designing, analysis and interpretation of data, and helped in drafting and revising the work. RD helped in drafting and revising the work. BP helped in planning and designing the work. AV helped in planning and designing the work and critically revising the work. IJR helped in planning and designing the work, interpretation of data, and critically revising the work. MPR helped in the data analysis and in critically revising the work. KV helped in planning and designing the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Prior approval from the local ethics committee was taken before starting the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.