Article Text

Abstract
Background Cognitive–behavioural theories of panic disorder posit that panic attacks arise from a positive feedback loop between arousal-related bodily sensations and perceived threat. In a recently developed computational model formalising these theories of panic attacks, it was observed that the response to a simulated perturbation to arousal provided a strong indicator of vulnerability to panic attacks and panic disorder. In this review, we evaluate whether this observation is borne out in the empirical literature that has examined responses to biological challenge (eg, CO2 inhalation) and their relation to subsequent panic attacks and panic disorder.
Method We searched PubMed, Web of Science and PsycINFO using keywords denoting provocation agents (eg, sodium lactate) and procedures (eg, infusion) combined with keywords relevant to panic disorder (eg, panic). Articles were eligible if they used response to a biological challenge paradigm to prospectively predict panic attacks or panic disorder.
Results We identified four eligible studies. Pooled effect sizes suggest that there is biological challenge response has a moderate prospective association with subsequent panic attacks, but no prospective relationship with panic disorder.
Conclusions These findings provide support for the prediction derived from cognitive–behavioural theories and some preliminary evidence that response to a biological challenge may have clinical utility as a marker of vulnerability to panic attacks pending further research and development.
Trial registration number 135908.
- panic disorder
- panic attacks
- biological challenge
- prediction
- systematic review
- spontaneous panic attacks
- vulnerability
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- panic disorder
- panic attacks
- biological challenge
- prediction
- systematic review
- spontaneous panic attacks
- vulnerability
Introduction
Panic attacks are characterised by brief episodes of intense arousal and fear that arise suddenly, often in the absence of a clear internal or external trigger. Cognitive–behavioural theories posit that panic attacks arise from a ‘vicious cycle’ between the bodily sensations associated with physiological arousal and a sense of perceived threat.1–4 Perhaps the most well known of these theories is David Clark’s cognitive model, which posits that panic attacks arise when a person misinterprets bodily sensations (eg, increased heart rate) as a sign of impending danger (eg, a heart attack).5 These ‘catastrophic misinterpretations’ lead to a perception of threat which, in turn, increases physiological arousal, thereby feeding into a positive feedback loop that culminates in a panic attack.
Recently, Robinaugh and colleagues6 formalised these ‘vicious cycle’ theories in a computational model of panic disorder: a syndrome characterised by recurrent panic attacks, persistent concern about those attacks and avoidance of situations in which they may occur. One of the key advantages of formalising theories in this way is that it allows researchers to simulate the behaviour implied by the theory, thereby providing a tool to evaluate what the theory can explain and what it cannot. The simulated behaviour of the computational panic disorder model suggests that it is able to explain key phenomena observed in panic disorder, including individual differences in the propensity to experience panic attacks and phenomenological characteristics of those attacks.
The computational model also makes several novel predictions. One such prediction is that the vulnerability of the system to panic attacks and panic disorder can be indexed by how it responds to perturbation. In particular, vulnerability (or, conversely, resilience) can be indexed by the duration of time to respond to a perturbation (an index known as ‘engineering resilience’ in the dynamical systems literature).7 In the panic disorder model, when the positive feedback loop between arousal and perceived threat is weak, perturbations to arousal cause only a brief and modest increase in arousal and perceived threat. However, when this positive feedback is strong, it takes longer to recover from perturbation. In other words, the time taken to respond to perturbations is an indicator of vulnerability to panic attacks.
This prediction is noteworthy because there is a large literature examining how individuals with panic disorder respond to just such a perturbation. These perturbations, known as ‘biological challenges’, entail the administration of standard procedures, typically the injection or inhalation of a substance (eg, lactate infusion8 or CO2 inhalation9), in order to induce arousal-related bodily sensations.10 11 That is, these challenges perturb the system by increasing arousal and then evaluate how the system responds.
The panic disorder model suggests that these biological challenges could thus serve two valuable purposes. First, the challenges can be used to evaluate the cognitive–behavioural theories embodied in the computational model. The model explicitly predicts that psychological and physiological reactivity during biological challenge procedures reflects vulnerability to panic attacks and, thus, should be predictive of subsequent spontaneous panic attacks and panic disorder. Second, if this model prediction is supported, it would suggest that biological challenges have clinical value as objective measures of vulnerability to panic attacks.12
In this paper, we reviewed empirical studies evaluating the relationship between response to a biological challenge and subsequent panic-related outcomes. We had two overarching aims. First, we aimed to identify the challenge procedures and measures of psychological and physiological reactivity that have been studied as predictors of subsequent panic attacks and panic disorder. Second, we aimed to evaluate whether response to a biological challenge is indeed predictive of subsequent panic attacks and panic disorder.
Methods
Search strategy and selection criteria
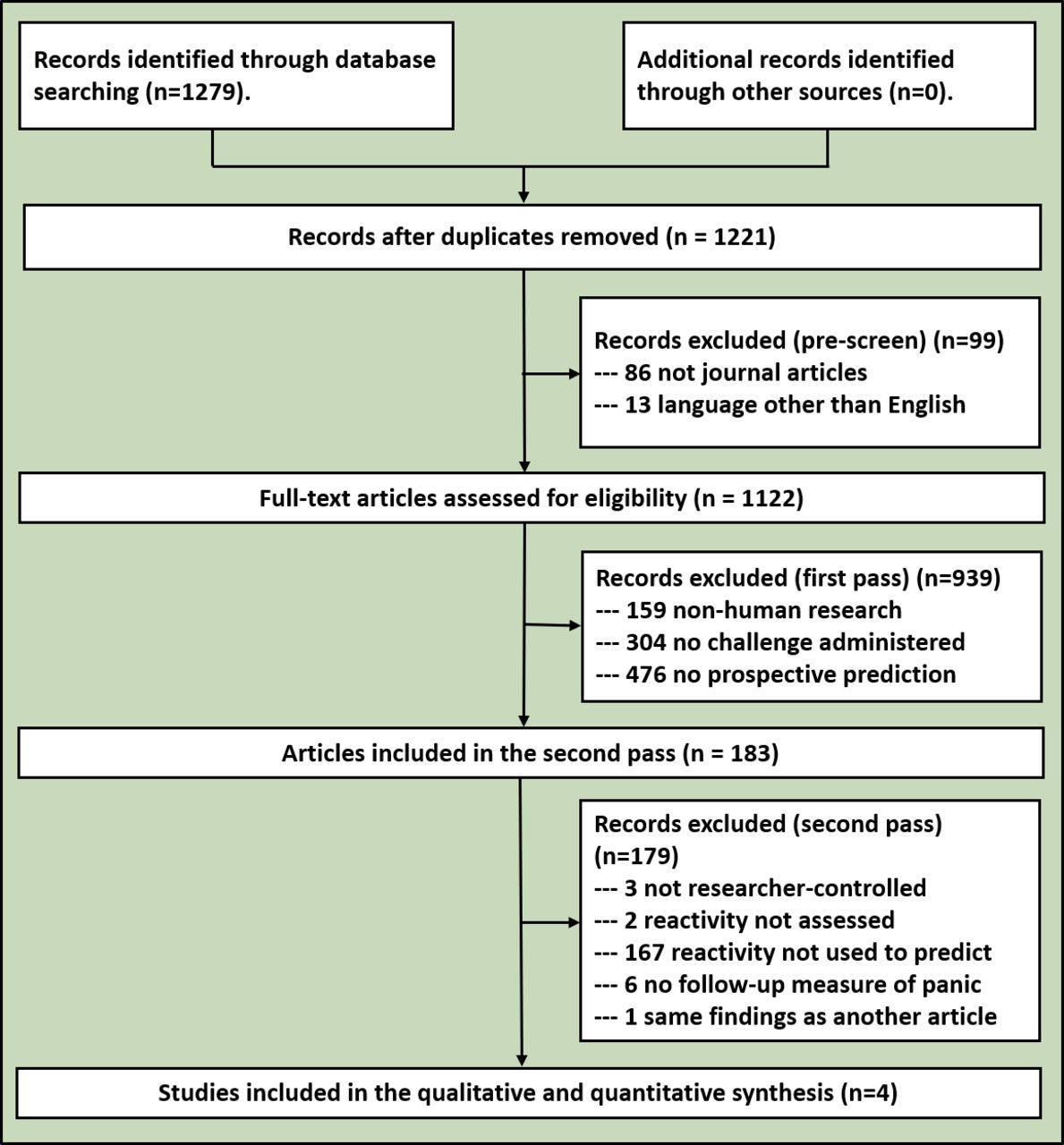
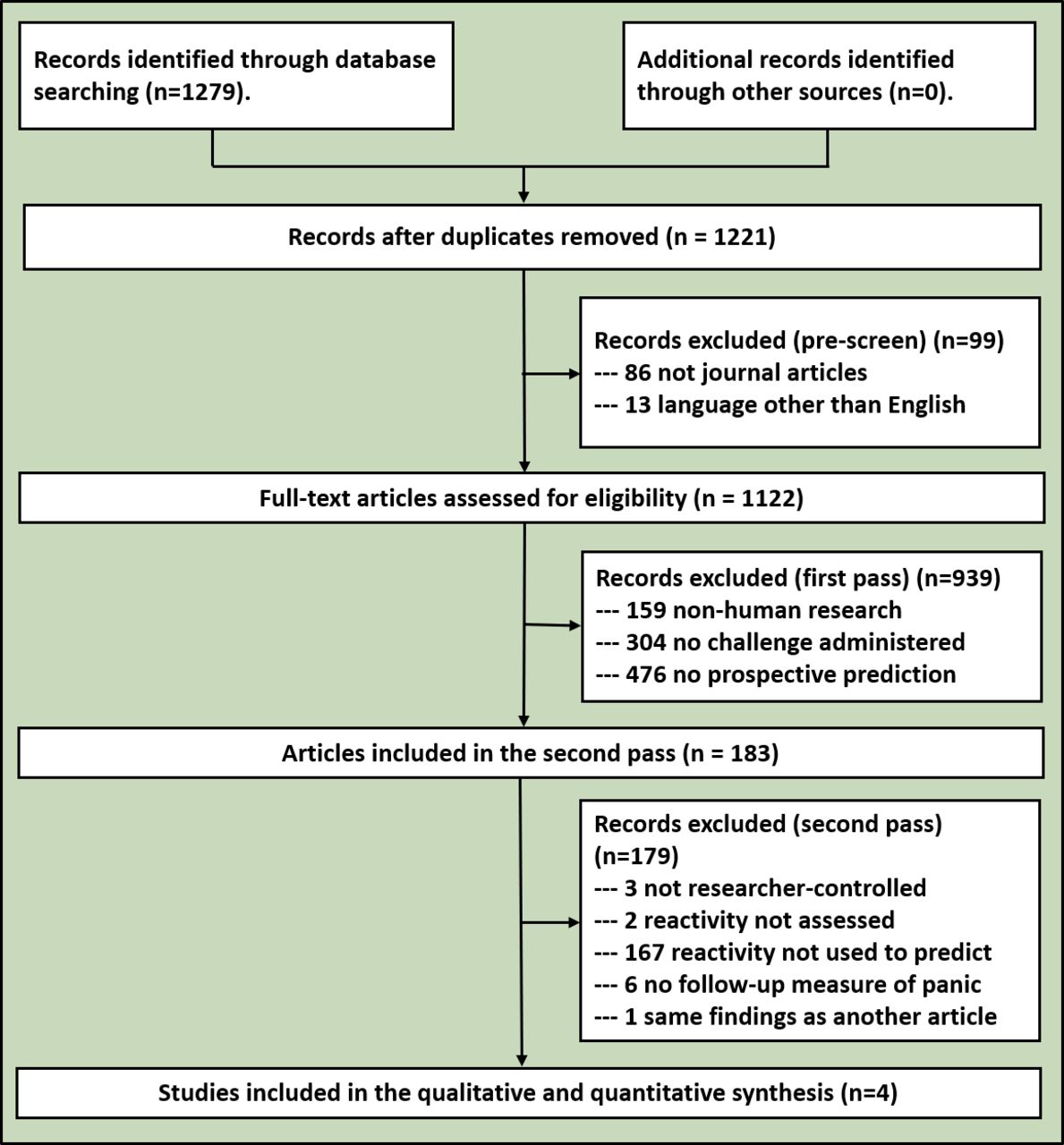
We conducted a systematic review in accordance with the guidelines presented by the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P)13 and the International Prospective Register of Systematic Reviews (PROSPERO).14 The review protocol (registration number 135908) was submitted to PROSPERO on 23 May 2019 and last updated on 11 September 2019 to clarify our data analytic strategy. Database searches were conducted using PubMed, Web of Science and PsycINFO between 1 June and 2 June 2019. Search terms consisted of provocation agents (eg, CO2, sodium lactate, cholecystokinin) and procedures (eg, challenge, inhalation, infusion) combined with keywords relevant to panic disorder (eg, anxiety, panic, fear). When conducting our literature search, terms were grouped in quotations (eg, ‘CO2 challenge’ AND ‘panic’) to identify articles that examined biological challenge procedures in the context of anxiety disorders. A PRISMA diagram for this search appears in figure 1.
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram.
Screening and data extraction were completed by four authors of this paper (ERT, MJW, MLB and OML). All results from the literature search were uploaded into a shared Excel spreadsheet and divided among the coders. Records were prescreened and excluded if they were duplicate entries, non-journal articles or written in languages other than English. Eligibility screening was conducted in two phases. First, we excluded articles without human subjects, without administration of a biological challenge or without follow-up time points. Second, we excluded articles in which: (A) the challenge procedure was not researcher controlled (ie, if the challenge was subject to varying degrees of participant engagement, such as breath holding), (B) measures of psychological or physiological reactivity were not obtained, and (C) reactivity measures were not specifically used to predict the future panic-related outcomes. Thus, eligible studies needed to report follow-up outcomes that directly pertained to panic attacks or panic disorder. Throughout the screening process, disagreements and inconsistencies were brought to the attention of the first author and discussed as a group until reaching a resolution.
Our screening process identified five articles that met full eligibility criteria. Among these, two articles15 16 reported the same set of findings. We omitted the second reporting of these findings from our review.15 From the remaining four articles, we extracted sample size, sample characteristics, biological challenge characteristics, measurements obtained during and/or in response to the challenge, mean follow-up time frame and panic-related outcomes (eg, the number of participants who subsequently experienced spontaneous panic attacks or panic disorder). Finally, we extracted relevant statistics regarding the relationship between biological challenge reactivity and follow-up measures of panic attacks or panic disorder.
Statistical analysis
In our preregistered review protocol, we proposed to quantitatively synthesise the data from our review using the ‘metan’ procedure in STATA,17 calculating pooled effect size estimates using a random effects model. In the spirit of transparency, these planned analyses are reported in the online supplementary appendix. However, the number of eligible articles identified in our literature search (n=4) is below the recommended minimum (n=5) for random effects models18 and two studies reported multiple indices of reactivity, thereby introducing dependency in the effect size data that our planned analyses were not equipped to address. Accordingly, we revised our analyses to use fixed effects models and conducted analyses in two groups based on how researchers assessed response to the biological challenge procedure: (A) response assessed using panic attack symptoms and (B) response assessed using subjective anxiety or distress. A third type of response index (objective indices of physiological response) was reported in one study.19 The effect sizes were reported as correlation coefficients (r) with 95% CI. Although there is still debate over what constitute a small, moderate and large effect,20 we will adopt the convention that correlation coefficients of 0.10, 0.30 and 0.50 correspond to weak, moderate and strong associations, respectively.
Supplemental material
Bias assessment and quality of evidence
We used the Cochrane Collaboration’s bias assessment guidelines to evaluate risk of performance bias, detection bias, attrition bias and reporting bias in each eligible study. Performance bias denoted systematic differences between ‘groups’ (ie, those who exhibited an elevated response to the biological challenge relative to those who did not) in exposure to factors other than the response to the biological challenge (eg, if responders were provided treatment, but non-responders were not). Detection bias denoted systematic differences between groups in outcome assessments (eg, if those conducting follow-up assessments were aware of the participant’s responder status, they may be biased in their assessment of panic attacks and panic disorder). Attrition bias denoted differences between groups in withdrawal from the study (eg, if responders were more likely to drop from the study during the follow-up period). Reporting bias denoted selective outcome reporting (eg, if two measures of panic attacks were administered during the follow-up period, but only one is reported). In addition, we used the Grading of Recommendations Assessment, Development and Evaluation guidelines to consider the quality of evidence in favour of the hypothesis that response to a biological challenge is predictive of subsequent panic attacks and panic disorder.
Results
Study characteristics
The results of our literature search appear in table 1. Each of the four studies included participants vulnerable to panic attacks, either due to elevations in anxiety sensitivity16 21 or by their relationship to someone with panic disorder.19 22 Two studies also included healthy controls not vulnerable to panic attacks.19 21 Sample sizes ranged from 31 to 295, with a median sample size of 71 (mean n=119.5). Follow-up assessments occurred between 1 and 4 years following the biological challenge (mean and median follow-up=2.5 years). The biological challenge in all studies was CO2 inhalation. In three studies, researchers administered 35% CO2, with one study also administering a subsequent 5% CO2 challenge following recovery. In one study,16 researchers used a 20% CO2 challenge.
Biological challenge response and subsequent panic attacks
Prediction of panic attacks
Across these four studies, researchers examined seven estimates of the relationship between biological challenge reactivity and subsequent panic attacks during long-term follow-up. Response to the biological challenge was assessed using panic attack symptoms, subjective anxiety or distress, or an objective index of physiological response. We examined these types of response separately. We first examined studies in which researchers assessed symptoms of a panic attack elicited by the biological challenge, using either the Acute Panic Inventory or a similar assessment of self-reported symptoms of panic attack. In two of these studies,19 21 researchers dichotomised this assessment to reflect the presence versus absence of a panic attack. A third study16 reported the sum severity of these panic symptoms. Across these three studies, the I–V pooled effect size of the association between panic symptoms in response to a challenge and subsequent panic attacks during the follow-up period was 0.414, 95% CI 0.331 to 0.497. There was heterogeneity across the three studies (I2=82.5%, p=0.003). We next examined the studies in which researchers assessed response by measuring change in anxiety from prechallenge to postchallenge using a visual analogue scale of anxiety19 22 or another self-reported rating of subjective distress.16 The I–V pooled effect size of the association between subjective anxiety or distress in response to a challenge and subsequent panic attacks was 0.443, 95% CI 0.370 to 0.516. There was again heterogeneity across the three studies (I2=95.0%, p<0.001). Finally, in the one study that included a physiological measure,19 researchers reported a small association (r=0.211 (−0.066 to 0.457)) between abnormal minute ventilatory slope during 5% CO2 exposure and subsequent panic attacks. Further description of our analyses and results appears in online supplementary appendix.
Prediction of panic disorder
Three of the four studies we reviewed assessed panic disorder over the course of the follow-up period. Two of these studies reported that no participants developed panic disorder, thereby precluding any examination of predictors of this disorder. In the one study for which a subset of participants did develop panic disorder,16 researchers reported that neither subjective distress nor self-reported psychological symptoms predicted subsequent panic disorder (r=0.03 and r=−0.01, respectively). Because only one study examined this association, no data synthesis was performed.
Bias assessment and quality of evidence
We found overall low risk of bias across the four studies (see online supplementary appendix for a complete description). However, we did identify one study19 in which the researchers reported analyses for only two of the four CO2 challenge response indices that were assessed in the broader study without a rationale provided for limiting the analyses in this way, indicating a high risk of reporting bias. In addition, there were areas where risk could not be determined, including two studies that did not specify whether the clinical interviewers who assessed panic attacks and panic disorder at follow-up were blind to biological challenge response, thereby making the risk of detection bias unclear.
We evaluated the strength of evidence in favour of the hypothesis that biological challenge response is prospectively associated with panic attacks. We considered the overall risk of bias to be low and the pooled effect size sufficiently precise so as to warrant some confidence in these findings. However, the inconsistency of results across studies lowers our certainty in this evidence. Accordingly, we regard the quality of the evidence to be moderate: further research is likely to impact our confidence in this effect and may change the estimate of this association.
Discussion
In this review, we first aimed to determine which biological challenge procedures, measures of psychological and physiological reactivity, and outcome assessments have been studied as predictors of subsequent panic attacks and panic disorder. We found that only one biological challenge paradigm has been used to investigate this association: the inhalation of air with elevated concentrations of CO2. Across four studies using this procedure, researchers examined reactivity in three broad categories: (A) using assessments of panic symptoms present following the induction, often dichotomised to reflect the presence versus absence of a panic attack, (B) change in subjective distress or anxiety as indicated by response on a visual analogue scale of anxiety or subjective units of distress scale, and (C) objectively assessed minute ventilation response. Although three of the four studies assessed the onset of panic disorder, only one study included at least one participant who developed panic disorder during the follow-up period. Together, these findings suggest that despite the considerable number of studies in the panic disorder literature using a biological challenge, few have examined response to these challenges as a prospective predictor of panic attacks or panic disorder. Moreover, those that have examined this association have used a single procedure, a limited number of reactivity measures, and typically have not included a sufficient number of participants to assess whether reactivity predicts the development of panic disorder. Of particular relevance, no study examined the duration of recovery from the biological challenge as a predictor of panic attacks. Accordingly, our review of the literature suggests that there remains a great deal of work to be done to further evaluate biological challenge as indicators of vulnerability to panic attacks and panic disorder.
Main findings
Prospective prediction of panic attacks
Despite this, we did identify four studies that could be used to evaluate the hypothesis that reactivity to biological challenge can be used to prospectively predict panic-related outcomes. Together, the results of these studies provide qualified support for this hypothesis. The pooled effect sizes suggest a moderate significant association between response to biological challenge and subsequent panic attacks. This was true both when assessing panic attack symptoms and when assessing subjective anxiety or distress in response to the challenge. However, it is important to note that the pooled effect sizes were driven largely by a single study. This study reported a strong association between both subjective distress and panic attack symptoms during a biological challenge using 20% CO2 inhalation and subsequent panic attacks. Other studies reported smaller, and in one case negative, associations.
In three studies specifically examining panic attack symptoms elicited by a CO2 challenge, there was evidence for a relationship with subsequent panic attacks across all three studies.16 19 21 This effect was substantially larger in the one study that did not dichotomise these symptoms to indicate the presence versus absence of a panic attack, but instead reported the sum severity of panic attack symptoms.16 It may be that dichotomising panic attack occurrence during a CO2 challenge results in loss of information that is relevant to predicting vulnerability to subsequent panic attacks. Indeed, the simulated biological challenge paradigms that motivated the current review6 suggest that not all individuals vulnerable to panic attacks will necessarily experience a full panic attack following a given perturbation. Accordingly, a dichotomised index may fail to identify some individuals who are, indeed, vulnerable to panic attacks. Consistent with this possibility, in Harrington et al’s21 study the biological challenge exhibited low sensitivity as a predictor of subsequent panic attacks (33%). Sensitivity was higher (65%), though still poor, in Coryell et al’s19 study. Notably, although the effect size for reactivity as a predictor of subsequent panic attacks was consistent between these two studies, there were differences in the proportion of individuals identified as having experienced a challenge-induced panic attack (64% in Coryell et al’s study; but only 21% in Harrington et al’s study). This finding may be due to the higher proportion of females in the study by Coryell and colleagues. Few other differences between studies are apparent, although it is possible that the difference in sensitivities may be attributable to how challenge-induced panic attacks were assessed. Regardless, these analyses suggest that researchers interested in using the biological challenge paradigm as an indicator of vulnerability to panic attacks may be better served by a continuous measure of panic attack symptoms.
Differences in the timing of when these surveys are administered may also contribute to variability across studies. Latent class analyses suggest three patterns of response to CO2 challenge: (A) low anxiety, which comprises the majority of participants whose anxiety remains low before, during and after the challenge; (B) acute anxiety, which reflects anxiety that is low prechallenge and postchallenge, but spikes substantially during the challenge itself; and (C) persistent anxiety, which reflects anxiety that is elevated before, during and after the challenge.23 Individuals showing the persistent anxiety pattern may be especially vulnerable to panic disorder. They report greater anxiety sensitivity, agoraphobic avoidance, stress and a propensity towards escape behaviour during the challenge procedure. This pattern of response suggests that some individuals vulnerable to subsequent panic attacks may exhibit high anticipatory anxiety before the biological challenge and, consequently, may exhibit less change in subjective anxiety following the induction. In Schmidt et al’s16 study, the researchers allowed for a 5 min adaptation period after affixing the CO2 apparatus before completing the preinduction assessment of distress, potentially allowing anticipatory anxiety to diminish before administering the prechallenge assessment of subjective distress. No such procedure is explicitly noted in the other studies. In future research, researchers should ensure an appropriate baseline assessment period that is not confounded by anticipatory anxiety in those especially vulnerable to panic attacks.
Prospective prediction of panic disorder
In the one study to examine prospective prediction of panic disorder, researchers found that neither self-reported panic attack symptoms nor subjective distress in response to a biological challenge predicted subsequent panic disorder.16 Accordingly, while biological challenge response may indicate vulnerability to panic attacks, other factors may be responsible for the transition from panic attacks to panic disorder. For example, some individuals may have experienced panic attacks but did not develop panic disorder because they chose not to engage in subsequent avoidance behaviour. Researchers interested in examining biological challenge response as a marker of vulnerability should thus consider incorporating additional assessments beyond response to biological challenge alone (eg, a propensity to use avoidance behaviour as a strategy for emotion regulation), as such responses may be needed to fully account for the development of panic disorder in those vulnerable to experiencing panic attacks.
Limitations
There were several limitations to the extant literature and to our analysis that should be noted. First, our review was limited to English language articles, potentially omitting other studies examining the association of interest. Second, the small number of articles and inconsistency of findings across studies suggests that some caution is warranted when interpreting our pooled effect sizes and emphasises the need for further research. Third, in an examination of the risk of bias in the reviewed studies, we broadly found low risk of bias, but did identify some areas where the risk of bias was uncertain and one study19 where the risk of reporting bias was high (see online supplementary appendix for further details). Fourth, it is important to note that although the pooled effect sizes are consistent with the hypothesis that biological challenge response may prospectively predict panic attacks, the strength of this effect was moderate and below what would be required for this challenge to have genuine clinical utility. Accordingly, the findings presented here should be taken as an indicator only of its potential utility as an objective indicator of vulnerability pending further research and development.
Implications
Consistent with the predictions of a recently developed formal theory of panic disorder,6 we found qualified support for the hypothesis that reactivity to a biological challenge procedure is predictive of subsequent panic attacks. We found no evidence that reactivity is predictive of subsequent panic disorder. The results of our systematic review inform theoretical models of panic attacks and panic disorder and provide preliminary support for the possibility that biological challenge reactivity could be used to indicate vulnerability to panic attacks. For theoretical models of panic disorder, it will be necessary to account for the possibility that biological challenge response may predict panic attacks but not panic disorder. For researchers interested in further investigating whether responses to biological challenges can provide panic attack vulnerability markers, the empirical literature points in several promising directions. First, researchers should refrain from dichotomising variables, instead using the continuous measures of panic attack symptoms or subjective distress to prospectively predict panic attacks. Second, researchers should ensure an appropriate baseline period for assessing prechallenge anxiety and physiological arousal so as to avoid confounding this period with anticipatory anxiety. Third, researchers should examine alternative procedures and indices of response. Future research would especially benefit from examining common objective indices of physiological response, such as heart rate and skin conductance, and other indicators of response (eg, time to recovery). Indeed, perhaps the most fundamental conclusion from this review is that much more work is needed to further investigate the biological challenge paradigm as a prospective predictor of panic attacks in order to determine whether reliable and clinically useful markers of vulnerability to panic attacks and panic disorder can be identified.
References
Dr. Donald J. Robinaugh received his PhD from Harvard University in 2015 under the mentorship of Dr. Richard McNally. Since 2018, he has worked as a clinical psychologist at the Center for Anxiety and Traumatic Stress Disorders and Complicated Grief Program in the Department of Psychiatry at Massachusetts General Hospital and as an assistant professor of psychiatry at Harvard Medical School. Dr. Robinaugh’s research is primarily focused on using computational psychiatry and the tools of network science to investigate mental disorders as complex systems. He is especially focused on applying these tools in the context of anxiety disorders and complicated grief.

Footnotes
Contributors DJR, ERT and SPO conceptualised the present review. ERT wrote the PRISMA-P protocol that provided the framework for this review with edits from DJR. MLB conducted the literature review based on the eligibility criteria, information sources and search strategy detailed in the protocol. MJW, MLB, OML and ERT conducted the first pass eligibility screening and MJW completed the second pass screening. EB, DJR and MJW contributed to data extraction, statistical analyses and interpretation of study findings. ERT and MJW wrote the Methods section of the manuscript. DJR wrote the remainder of the first draft of the manuscript. DJR, MJW and ERT contributed to the revision of the manuscript.
Funding This study was supported by a National Institute of Mental Health Career Development Award (1K23MH113805-01A1).
Disclaimer The NIMH is not involved in any other aspect of the project, such as the development of the protocol or the interpretation of study findings. No funding has been received for this study specifically.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement There are no data available