Article Text

Abstract
Wilson disease (WD) is an uncommon recessive genetic disorder affecting copper metabolism. Cardiac, neurological, hepatic and renal manifestations are well defined, nevertheless approximately 30% of patients debut with neuropsychiatric symptoms. These psychiatric alterations resulting from the accumulation of this heavy metal in the basal ganglia are some how less specific. We present a short review of psychiatric symptoms of WD and describe a case of a 37-year-old woman diagnosed with WD who presented neuropsychiatric symptoms and had a consequent delay in diagnosis and causal treatment. Patients who develop WD starting with a predominance of neuropsychiatric symptoms tend to manifest hepatic symptoms later, therefore have a longer delay of diagnosis and a poorer outcome than patients with hepatic symptoms. An early diagnosis of WD can avoid irreversible neurological damage.
- Wilson disease
- neuropsychiatric symptoms
- psychiatric manifestations
- copper metabolism
- extrapyramidal side effects
- Etnicity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Wilson disease
- neuropsychiatric symptoms
- psychiatric manifestations
- copper metabolism
- extrapyramidal side effects
- Etnicity
Introduction
Wilson disease (WD) is a recessive inherited disorder caused by a reduced incorporation of copper into ceruloplasmin resulting in the accumulation of this metal in different tissues especially in the liver, central nervous system, heart and kidneys.1
WD was first described by Kinnear Wilson as a familial, lethal neurological disease accompanied by chronic liver disease leading to cirrhosis: it was first called ‘progressive lenticular degeneration’.2
Hepatic, neurological, cardiac and renal damages occurring in WD have been widely studied.3 During the last few years researches have focused on establishing the genetic basis of this disease, finding the origin of a defect at the level of the ATP7B gene which causes the mentioned alteration in the metabolism of copper.4
Ceruloplasmin level (<20 mg/dL), baseline hypercupriuria (>100 µg/24 hours), elevated urinary copper excretion after oral administration of D-penicillamine and mutation analysis of the ATP7B gene are helpful for the diagnosis of WD.5 6
The psychiatric alterations resulting from the accumulation of this heavy metal in the basal ganglia are somehow less specific.
Review of psychiatric features of WD
Psychiatric and behavioural alterations in WD are very variant in frequency and type as they encompass a wide spectrum of symptoms. Psychiatric symptoms usually occur in 2–3 years after the first hepatic and neurological manifestations and approximately in 30% of patients.7 Patients often develop behavioural and psychiatric abnormalities such as depression, paranoia, delirium, hallucinations, irritability, sexual disinhibition, difficulties and worsening results at school or work . Changes in personality and behaviours such as irritability and aggressiveness are the most well-described symptoms. Cognitive and behavioural symptoms can be reversed after 1–2 years of continuous treatment.8 Psychotic symptoms are uncommon in WD. These psychotic symptoms normally represent a typical paranoid schizophrenia and are associated with very severe extrapyramidal signs, but these signs are normally interpreted as secondary to the use of antipsychotics so it causes a delay in diagnosis.9 10 Neuropsychiatric presentations are more associated with the presence of dysarthria and incongruent behaviour instead of patients presenting neurological symptoms exclusively.11 Some studies had reported a higher prevalence of Kayser-Fleischer ring (copper accumulation in the cornea) in individuals with neuropsychiatric manifestations.12
In some cases, although it is less frequent, the psychiatric symptoms can be the first manifestation of the disease.13
The prevalence of psychiatric disorders in patients diagnosed with WD has been measured in small samples of individuals.
In 1989, Dening and Berrios reported a series of 195 cases of WD. Fifty-one per cent displayed evidence of any psychopathology and twenty percent had a psychiatric intervention before being diagnosed with WD. Abnormal behaviours, personality changes, depression and cognitive impairment were the most common psychiatric features. Psychiatric symptoms were related to neurological rather than hepatic symptoms.11
There is a recent wide review about the psychiatric symptoms of WD published in 2014. They conclude that psychiatric symptoms can occur before, concurrent with or after the diagnosis and treatment of WD. Approximately 30%–40% of patients display psychiatric manifestations at the time of diagnosis. When psychiatric symptoms preceded neurological or hepatic symptomatology, the average time between the occurence of psychiatric symptoms and the diagnosis of WD was extremely long(an average of 864.3 days). Some gene mutations of ATP7B may correlate with specific personality traits changes.14
We found another retrospective natural study with a sample of 350 individuals with an average age of 18.8 years that had psychiatric symptoms. Diagnosis of WD was studied in this sample and it turned out that 15 of them met the criteria. History of jaundice, family history of neuropsychiatric manifestations and sensitivity to neuroleptics were the most common findings in those who met the criteria.15
In sum, in clinical practice there is a lack in recognition of psychiatric symptoms as being due to WD although there is a higher prevalence than it has previously been thought. It leads to a delay in diagnosis and treatment of this disorder and increases the probability of irreversible neurological damages.16
Case report
The patient is a 37-year-old gypsy woman with basic schooling, possibly with learning difficulties. She has no medical or psychiatric background. Family history includes a sibling with schizophrenia, another diagnosed with acute polymorphic psychotic disorder and alcoholism, and a sister with intellectual disability.
Disease debases 4 months ago with depressive symptoms (apathy, anhedonia) accompanied by social isolation, fatigability, bradypsychia, bradylalia, psychomotor slowing and distal tremor. There were no psychotic symptoms. Weight loss was up to 6 kg. The patient related that the disorder started due to physical mistreatment that she received from her current partner.
She was diagnosed with reactive depression and treated with selective serotonin reuptake inhibitor (fluoxetine started at 20 mg which increased to 40 mg) for 3 months. Depressive symptoms did not improve and the patient made a suicide attempt by a punctual drug ingestion (levomepromazine 300 mg) and was admitted to a psychiatric hospital because of persistent suicide ideation. During her stance in the emergency room, general evaluation was made with no alterations in haemogram, basic biochemistry and coagulation exams. Neuropsychiatric exploration revealed sadness, crying, apathy, anhedonia, fatigability, bradypsychia, bradylalia, psychomotor slowing and distal tremor. All of these symptoms were accompanied with histrionic behaviour.
During the first 3 days, she presented with a sudden change in behaviour starting with mutism and very striking alterations in gait that were considered as possible dissociative symptoms and began treatment with antipsychotics (quetiapine 200 mg/24 hours for a week). This temporary diagnosis was based on the recent stressful life events that occurred and her personality traits, before an extended neurological study was made with more specifical laboratory and image tests. Treatment was not effective and caused significant extrapyramidal side effects such as increased psychomotor slowing, hypertonia and tremor.
In later physical and neurological examinations hypomimic face and hyperpigmented complexion (it can be explained by her constitutional origin) were the highlighted signs as well as other neurological symptoms such as cognitive alterations due to motor coordination, ataxic march with inability to march in tandem, extrapyramidal axial hypertonia, akinesia and tremor.
New behavioural alterations appeared, including potomania, impulsive food intake and mutism accompanied by psychotic symptoms such as auditory hallucinations ‘voices that give orders’.
Complementary exams
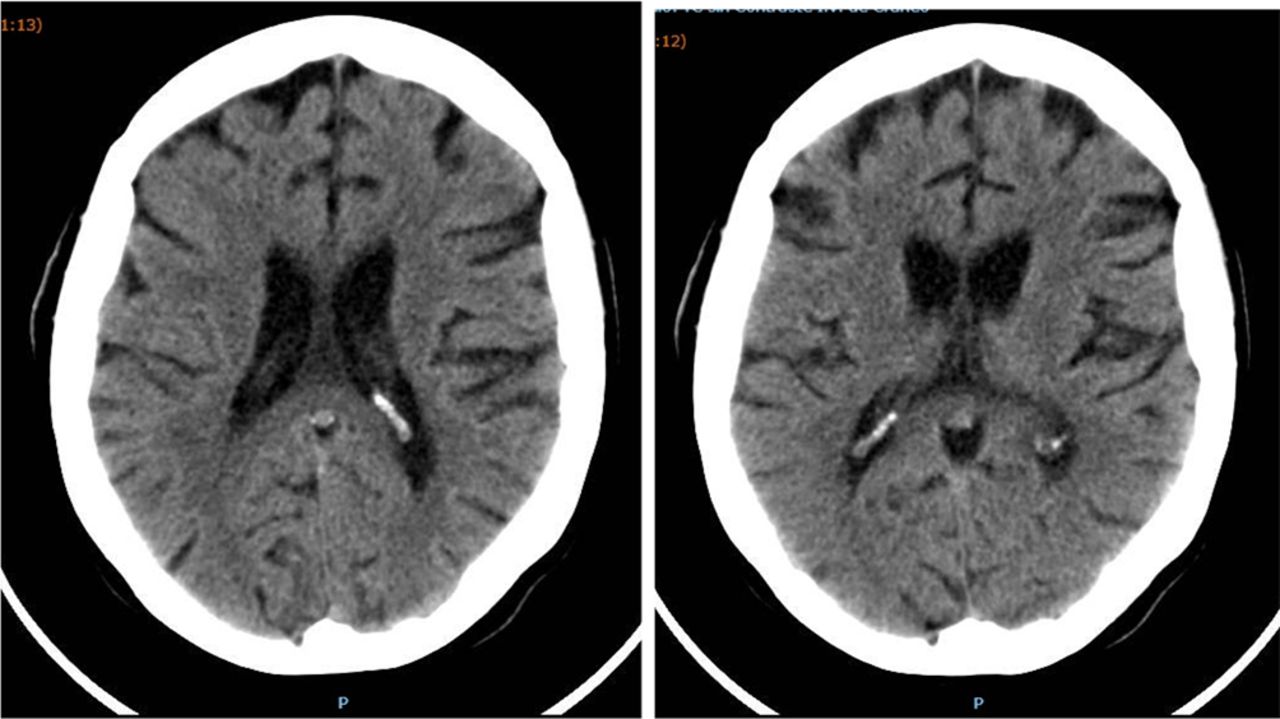
Cranial CT showed moderate subcortical and cortical atrophy, which does not correspond to the patient’s age (see figure 1).

Cranial CT of Wilson disease showed moderate subcortical and cortical atrophy, which does not correspond to the patient’s age.
MRI skull: density increased in posterior protuberance and mesencephalon suggestive of WD (see figure 2).

{kind=link}
{kind=link}
MRI showed increased density in posterior protuberance and mesencephalon suggestive of Wilson disease.
Blood analysis: ceruloplasmin levels were low in blood, copper in urine 70 (normal <70), ceruloplasmin 16.6 (normal >20).
Ultrasound examination: there was no kidney or hepatic damage.
Ophthalmology: no Kaiser-Fleischer ring.
Evolution
WD was diagnosed and started treatment with D-penicillamine 250/6 hours.
Psychiatric symptoms were first resolved in the first 3 weeks of treatment with progressive resolution of the motor symptoms during the next 12 months (and without concomitant antipsychotic drugs) that required antiparkinsonian treatment with L-3,4-dihydroxyphenylalanine 100/carbidopa 25. The patient was discharged after 2 months of hospitalisation and referred to the neurological outpatient department. Eighteen months later there remained an ataxic march and ceruloplasmin levels normalised. No renal or hepatic damage was detected.
Genetic screening for the disease was recommended to her relatives with negative results.
Discussion
Literature reviewed according to the present patient shows that patients who develop WD starting with a predominance of neuropsychiatric symptoms tend to manifest symptoms later, and have a longer delay of diagnosis and a poorer outcome than patients with hepatic symptoms.17
WD is one of the few inherited disorders, which can be successfully treated with pharmacological agents (if diagnosed early). This is a very important point because psychiatric manifestation of WD often leads to diagnosis delay, and often to wrong prognosis. Worse prognosis18 as well as treatment with D2 antagonist (neuroleptics) often leads to irreversible early neurological deterioration19, maybe due to decrease of D2 receptors20.
Ethnicity and mistreatment played an important role in this patient. Constitutional coloured skin could mask/overlap possible dermatological changes. Mistreatment was explained as the main cause of a reactive depressive syndrome joined to a familiar history of mental disease. Low neurological signs as bradypsychia, movement retardation and fatigability were considered to be associated with the depressive state as well. A diagnosis of WD was only considered when important neurological signs appeared, such as ataxia, tremor, akinesia and extrapyramidal symptoms.
When neuropsychiatric symptoms are detected, brain MR or CT may detect structural abnormalities in the basal ganglia. Increased density on CT and hyperintensity on T2 MRI in the basal ganglia are the most frequently found abnormalities as we can also see in our patient’s images.21 22
A prospective study of major depression in WD reported an incidence of 27%.23 Although it is not clear what mechanism is involved in this depression, it is thought that it can be a double mechanism: reactive type (by disease) and direct type (due to alterations in different brain structures). Manic episodes have also been reported.
In terms of treatment, the direct effect of copper chelates on depressive symptoms is known. Therefore, a combination therapy (copper chelators plus antidepressant) may be a good approach for those patients24 but in the present case it is not needed.
In sum, psychiatric manifestations are common in WD and can be present at any point in the course of the illness. When they occur not associated with hepatic or neurological symptoms, there is a high risk of misdiagnosis. Diagnosis and appropriate treatment can solve psychiatric symptoms in a very short period of time. An early diagnosis of WD can avoid irreversible neurological damage.16 Sometimes, treatment with copper chelates is enough to resolve psychiatric symptoms.
References
Margarita Guerrero Jimenez completed her medical training at the University of Granada. She has made four university degrees from the University of Alcalá de Henares in Mental Health Emergencies and Affective Disorders, University of Granada in Neuroscience and Pain, International University of Valencia in Third Generation Psychotherapies and University of La Rioja in Sanitary Management and Direction. Currently she is developing her PhD in Clinical Medicine and Public Health under the line of research: Clinical Neuroscience and Health. She is also working as a psychiatrist specialist in the Virgen de las Nieves Hospital (Granada). She has performed the specialization via MIR in psychiatry in the Granada Sur Clinical Management Area, working a posteriori in the Community Mental Health Unit in this área for one year and in the Virgen de las Nieves Hospital in Granada Later for two years.

Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.