Article Text

Abstract
Background Despite high relapse rate among methamphetamine (MA) abusers, there still have been little empirical data to date detecting the risk factors related to craving and relapse from the perspective of MA abusers. Therefore, the aim of this study was to use qualitative research methods exploring the strengths, weaknesses, opportunities and threat factors that could facilitate or impede individuals’ abstinence in a real-life context from the perspectives of MA abusers.
Aim To use qualitative research methods exploring the strengths, weaknesses, opportunities and threat factors relating to individuals’ abstinence in a real-life context.
Method Semistructured interviews were conducted with 32 MA abusers recruited in Shanghai guided by open-ended questions on narrating the real-life catalysts and inhibitors related to craving, initiation, relapse and abstinence. All data were transcribed verbatim and analysed using a strengths, weaknesses, opportunities and threats (SWOT) analysis.
Results The results of the SWOT analysis revealed that contextual factors including peer influence, prevalence and availability of MA, familiar venue of MA use, discrimination, sexual behaviours, alcohol, emotional states and their attitudes towards smoking MA were important factors that contribute to reinitiation and relapse. Surveillance systems, antidrug social workers, vocational skills trainings, moving to another city and family responsibility might serve as counter measures targeting those mentioned weaknesses and threats above.
Conclusion This SWOT analysis highlights the complex nature of relapse. Comprehensive interventions strengthening coping skills such as virtual reality techniques are desperately needed to facilitate individuals’ sustained abstinence.
- methamphetamine
- qualitative research
- relapse
- abstinence
- SWOT analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Methamphetamine (MA) has long been one of the most abused drugs worldwide.1 While in China, it has become the most popular illicit drug since 2015.2 MA use is associated with individuals’ poor physiological and psychological well-being, increased HIV/AIDS infection and increased crime rates,3 and currently is a major public health issue both in mainland China and worldwide. Previous follow-up studies have shown that approximately 50% of patients relapsed within 6 months of treatment and developed the addiction again.4 In addition, nearly 80% of patients would enter into a vicious cycle of ‘treatment-abstinence-relapse-addiction’,5 thereby seriously affect their health and quality of life. As for MA, it was estimated that nearly 36% of abusers failed to remain abstinent during the first 6 months after treatment.6 In mainland China, generally more than 90% of patients relapsed within 1 year after discharge from treatment.7 According to the United Nations Office on Drugs and Crime, China has become one of the main markets and principal flows of MA worldwide.8 With its severe addictive effect and neurotoxicity, MA has brought serious effects and economic burden to the whole society in China and presents a great challenge to public health. Unfortunately, until now, there is no effective medical treatment for MA addiction, and finding new treatment approaches for MA addicts is still an urgent matter.9
Qualitative and quantitative studies have indicated that a great number of internal and external risk factors, such as positive and negative life events, social contexts, socioeconomic conditions, craving, peer pressure and lack of social support,10 were related to individuals’ attrition from treatment and relapse. Additionally, craving reflects a strong desire to take drugs and terminate withdrawal symptoms or unpleasant feelings immediately,11 and is one of the most important predicting factors and highly correlated with continuous drug abuse and relapse.12 Moreover, craving is a subjective experience and therefore better understanding of the causes of craving from the patients’ viewpoint may have potential value to the development of new therapeutic approaches.
Many current intervention studies on addiction mainly focus on reducing and helping patients better manage their craving13 and show promising results. These studies have already indicated that multiple promising treatment approaches such as pharmacotherapy, cognitive–behavioural therapy, cognitive remediation therapy, cognitive bias modification, mindfulness-based treatment and repetitive transcranial magnetic stimulation can help patients better reduce their self-reported craving, enhance their impaired impulse control abilities and contribute to a much longer period of abstinence.14 Unfortunately, despite these efforts, attrition and relapse rates are still high among patients, and none of these mentioned medication treatments have been officially approved to treat MA addiction.15 As such, it would be both highly important and urgent to develop better relapse prevention and management strategies for these patients.
Thus far, most of these studies were quantitative. However, studies focusing on patients’ experience and response to these risk factors contributing to individual’s craving in real-life circumstances are still insufficient, especially studies using a thematic analysis strategy to systematically analyse factors covering both internal and external aspects related to strengths, weaknesses, opportunities and threat factors contributing to abstinence or relapse. This makes it difficult to understand exactly how these factors facilitate or prevent craving and relapse based on one’s living experiences. What’s more, patients’ opinions and experiences of craving and smoking MA are critical in tailoring treatment systems and facilitating the best practices. Thus, qualitative studies using in-depth interviews with these patients would provide researchers important information about how these high-risk factors in a certain natural context may contribute or prevent individuals’ craving and relapse.
Thus, we conducted a qualitative study using the strengths, weaknesses, opportunities and threats (SWOT) approach to examine the personal experiences about factors that may facilitate or impede abstinence in a real-life context from the perspectives of MA abusers. SWOT analysis is one of the world’s most widely used methods for strategic planning. It was designed to assess strengths (S) and weaknesses (W) as internal capabilities, while opportunities (O) and threats (T) are posed by the external environment.16 Through SWOT analysis, covering both internal and external environments, our focus was mainly on illuminating MA addicts’ experiences during abstinence and relapse periods, as this would help us understand the real-life catalysts and inhibitors contributing to one’s sustained abstinence, and hoping to inform future interventions for MA-related problems.
Methods
Participants
According to the Chinese antidrug law, compulsory isolated rehabilitation, community-based rehabilitation and voluntary detoxification treatment are three major drug rehabilitation modalities in China. If individuals were found abusing illicit drugs and diagnosed with drug addiction for the first and second time, they were required to receive either community-based rehabilitation or voluntary detoxification treatment. However, if they were found using drugs for more than three times or refuse to receive community-based rehabilitation, they are going to receive a two-year-long compulsory isolated rehabilitation. Furthermore, before the end of the compulsory isolated rehabilitation, participants were assigned with an antidrug social worker to ensure the continuous rehabilitation treatment in the community. Based on this situation, in this qualitative study, participants were also recruited from compulsory isolated rehabilitation centres, communities or hospitals. Eligibility criteria were: (1) meeting diagnostic criteria for MA dependence in accordance with the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition;17 (2) had a history of abstinence after MA addiction treatments and then relapsed at least once; (3) patients mainly used MA before receiving the latest detoxification rehabilitation treatment; (4) no language difficulties; and (5) no severe mental health problems. The exclusion criteria included: (1) current medical diseases that required hospitalisation or regular monitoring; (2) serious physical or neurological illness that required pharmacological treatment affecting cognitive function; and (3) IQ <70 (figure 1).

Flow chart of the study
Procedures
A total of six semistructured in-depth interviews were performed. Participants were interviewed using a semistructured discussion guide developed from issues identified in previous literature related to abstinence and relapse, themes emerging from antidrug social worker interviews and in consultation with some senior professors of psychiatry at the Shanghai Mental Health Center. The interview guide was piloted with four MA addicts in another area, with minor amendments made before the interviews were formally conducted. The final topic guide covered five domains, as follows:
Histories of MA initiation.
Histories of treatment attempts and relapse.
Experiences on each abstinence attempt.
Important catalysts and inhibitors related to craving and relapse in the social environment.
Important factors facilitating or deteriorating abstinence.
For the purpose of privacy protection, participants were asked to use the given code names instead of their real names during the interview. They were encouraged to share their own stories related to MA smoking, especially the significant milestones when they relapsed or successfully overcame withdrawal and craving symptoms in accordance but not limited to the core topics. Sharing other interesting stories related to MA was also welcome. However, during the interview, participants could refuse to answer any topics or questions they were not interested in or felt uncomfortable with and they could also quit the interview at any time. One leading author together with three trained notetakers carried out all interviews and group discussions. Participants also signed a consent form before the interview. This qualitative research was carried out from April to November 2016 in Shanghai, China. Every interview and focus group discussion lasted about 1 hour and were conducted in private rooms at the Shanghai Mental Health Center.
Data analysis
Interviews were audio recorded with the permission of all the participants. Digital audio records were fully transcribed verbatim in Mandarin Chinese by two researchers independently before SWOT analysis. The SWOT analysis strategy aimed to summarise and develop themes and subthemes by generation of keywords, phrases, opinions, thoughts and attitudes of the participant towards external and internal factors in the social environment affecting abstinence. Because the transcribed data were in Mandarin Chinese, an inductive hand coding process was employed to help researchers derive potential themes. First, through an open coding procedure, transcribed data were first decomposed into many data units. These data units were then summarised and assigned a concept by the researchers, and appropriate codes were given according to the data unit concepts.7 Second, based on the principles of system analysis, all possible key influencing factors are closely related to those achieving abstinence or restarting to abuse MA. Third, these key factors were further synthesised and organised into themes as internal and external factors. Subsequently, through a discussion meeting, identified factors were organised, synthesised and classified together into categories referring to strengths and weaknesses as internal capabilities, opportunities and threats posed by the external environment according to the SWOT analysis strategy by all authors.
Results
Participant characteristics
A total of 32 participants were recruited and completed the interview (figure 1). The mean (sd) age was 34.16 (7.13) years, average length of MA use was 4.22 (2.71) years, average years of education received was 8.84 (2.17) years, average abstinence/admission before the interview was 9.88 (8.77) months; 14 participants were unemployed before admission, 13 participants were married and 19 participants were unmarried (9 single and 10 divorced). Detailed demographic characteristics of the sample are displayed in table 1.
Characteristics of participants
Themes related to SWOT analysis
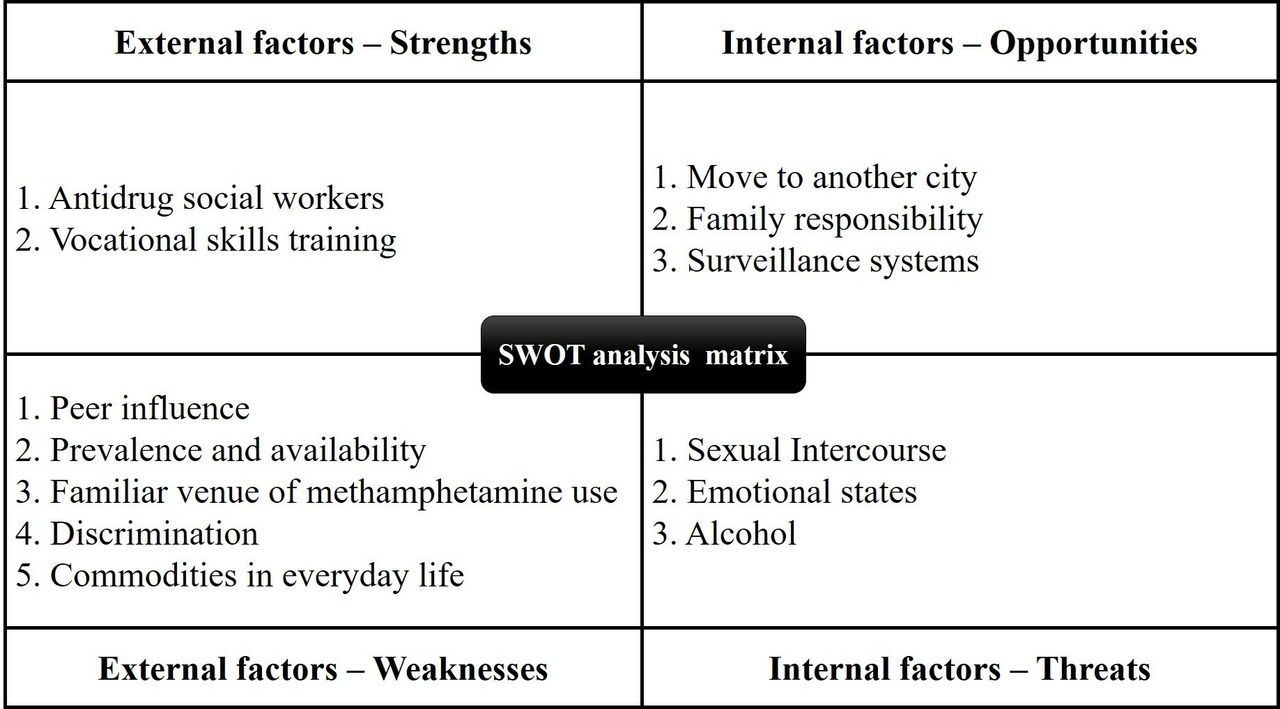
Themes and subthemes were identified as strengths, weaknesses, opportunities and threats based on the SWOT analysis model. The subthemes derived from the collected data were arranged under the themes found in figure 2.

{kind=link}
{kind=link}
SWOT analysis matrix
External factors: strengths
Antidrug social workers
Patients receiving community-based detoxification treatment, were assigned a social worker right before the end of compulsory isolation detoxification treatment. In Shanghai, there are a number of well-established rehabilitation social worker organisations helping patients sustain abstinence after drug addiction treatment. Participants agreed that these well-trained staff can provide good psychological counselling services, persuade them to do urine tests regularly and assist them in finding new jobs by arranging vocational skills training for them.
Vocational skills training
Some participants expressed that vocational skills training during detoxification treatments was crucial for them. These respondents described that with the skills they have learnt, they have successfully found a new job and been able to maintain abstinence longer.
I learned hairdressing skills, and with the help of my social worker and these skills, I finally found a new job and got a steady income.
I have learned embroidery during compulsory isolation detoxification, and now am selling my hand-embroidered works through my own online store.
External factors: weaknesses
Peer influence
Participants’ stories highlighting peer influence were still an important external driving force for relapse. More seriously, some participants even admitted that these ‘friends’ were their only remaining social relationships after chronic MA abuse and detoxification treatment, and they admitted that it was very difficult to refuse their friends, for fear of losing their remaining friends. Some participants also claimed that, after they finished their rehabilitation treatment, some of their ‘friends’ would ‘visit’ and persuade them to retry these drugs for celebration, and they did not know how to refuse them. More seriously, family and social supports were affected during treatments and their relationships were limited to other drug abusers that further worsen the effects of peer influence.
Prevalence and availability
Participants explained that they could get MA from their ‘friends’ and could even get MA in the communities where they were living. In addition, these patients admitted that, when facing real MA, they could hardly control the strong desires and craving for MA even if they have remained abstinent for a long time.
I initially tried MA in the community where I was living, and I could still purchase MA in the community even after two years of compulsory isolation detoxification treatments.
Familiar venue of MA smoking
Some participants complained that MA-related craving and memory could be evoked when participants went back to the place where they used to smoke and enjoy MA. These familiar places include the same hotel room, chamber in their home, offices and nightclubs.
After detoxification and rehabilitation treatments in a compulsory isolation center, I had to tell my family to rearrange the decoration of my bedroom where I used to smoke MA, because the moment I came into that room, I recalled the memory of a fun experience of using methamphetamine and the craving was aroused and became uncontrollable.
Discrimination
Participants complained that despite being abstinent for a long time, they were still judged by the people around them. They could still feel being looked down on by the residents in the community where they were living and even by their relatives, or when they were looking for a job.
My neighbors and relatives often looked down on me, and they would never believe I had quit smoking MA.
Discrimination even exists during the job interview. Once the interviewers know I had a drug abuse history, they would hardly consider hiring me, and regard me as having low self-control, and could never stop taking MA.
Commodities in everyday life
Several participants claimed there were a number of commodities that can trigger craving in their daily lives. They described that rock candies, especially the brown crystal sugar in pieces, which they called ‘huang bing tang’ (in Chinese), produce more craving, and could lead to a powerful craving for MA. Second, auxiliary equipment used to smoke MA, such as tinfoil, lighters and colourful drinking straws, when put together, could also trigger their craving for MA. Third, participants also agreed that food and beverages that have excitation effects, such as coffee, maltobiose and tea, could also lead to a desire for MA, and should never be touched again.
Internal factors: opportunities
Moving to another city
Some of these participants suggested that moving to a new place can also facilitate a longer abstinence.
After I finished the compulsory isolation detoxification treatments the second time, my parents decided to move to another city, the neighbors did not know I used to be a MA abuser, none of my friends were MA abusers, and I’ve kept sustained abstinence till now.
Moving to a new city means I can better say goodbye to what I had been and live a normal life. My ‘friends’ can never affect me, and no one would discriminate against me because I used to be a drug abuser.
Family responsibility
Some participants mentioned that greater awareness of their family responsibility was a strong internal factor for staying abstinent.
The main reason I quit smoking MA was that my father was badly ill, and needed me to look after him, I finally realised that if I continued to use MA, I could lose my beloved father.
When I was receiving the compulsory isolation detoxification treatment, the responsibilities of looking after my child and parents were all put on my wife, I felt regret for them.
Surveillance systems
In mainland China, surveillance systems mainly include ID card registration, police enforcement and antidrug social workers. If people were found smoking MA through urine test by police and diagnosed with MUD (methamphetamine use disorder) by psychiatrists, they were registered into the surveillance system and assigned with an antidrug social worker. They were required to take community-based detoxification treatments or voluntary detoxification treatments, and urged to receive urine tests regularly as well as spot checks through the help of an assigned social worker. However, when they were found smoking MA for the third time, they received compulsory isolation drug rehabilitation therapies. Some participants complained about how the surveillance system disrupted their everyday lives, resulted in their loss of job opportunities, made their MA abuse history more public and led to being judged by others. However, they admitted that the surveillance system works as a reminder for them to stay away from restarting smoking MA. Some participants found surveillance systems to be burdensome on their lives; however, participants also agreed that it can serve as a strong external driving force for participants to maintain abstinence.
Shortly after I had checked into a hotel, the local police came to my room and asked me to do a urine test. This reminded me that if I was found smoking MA again, I would be forced to receive two years of compulsory isolation detoxification.
Internal factors: threats
Sexual behaviours
Sexual-related behaviours were important catalysts for craving among many male abusers. Whoring, making love with sex partners, sex parties and online video chat rooms were the most frequently mentioned occasions. Interestingly, according to these participants, sexual behaviours were more common among male abusers. For male participants, they also regarded MA as an aphrodisiac. Moreover, an uncontrollable craving was often induced when they were having sex with their partners.
Sexual desires and related behaviours were very common among male abusers, and MA may also be used as an aphrodisiac to help them when making love with their partners.
We would much prefer enjoying methamphetamine with female friends, while males were not welcomed. This is because most of them would often demand sex after smoking MA.
Emotional states
Participants also described that their emotional states were related to relapse and could be intensified by stressful events, stigma and discrimination, and considered that smoking MA could help them cope with these feelings.
When I felt stressed or anxious, the first thought that would come to my mind was to enjoy MA to help release these negative feelings.
The joy of a party often makes me think of enjoying MA to celebrate it.
Alcohol
Some participants reported that alcohol could exacerbate their craving to smoke MA. Apart from using MA, some participants also reported a high incidence of alcohol use. Alcohol was treated as ‘a good friend’ when using MA. They said they often felt the craving for MA when they were drinking alcohol during a party or dinner. However, participants revealed that they did not prefer smoking any cigarettes when enjoying MA.
When I saw alcohol or after drinking alcohol, I often thought about using methamphetamine and the feeling was always very strong. However, there were few people who chose to smoke cigarettes before or after using methamphetamine. We did not smoke after using methamphetamine, because smoking would give us a headache and it would be impossible to tolerate the foul atmosphere of the room.
We do not smoke cigarettes after enjoying methamphetamine, because cigarettes were ‘hot things’ and smoking could affect the floaty euphoria of methamphetamine.
Attitudes towards smoking MA
Many patients did not think smoking MA and MUD were serious problems or mental health disorders. On the contrary, they thought that using MA was fashionable, entertaining and recreational in their everyday lives. ‘Playing with MA’ and ‘enjoying MA’ were the most used phrases when describing using MA. It seems that MA has already become one of their common daily entertainments, just like playing video games or mahjong, gambling, smoking, drinking, and so forth.
Discussion
Main findings
Craving reflects the individual’s strong desire for smoking drugs in order to alleviate the withdrawal symptoms, and is one of the most important factors that leads to relapse after treatment.12 Even after a long period of treatment, a variety of intrinsic and extrinsic drug-related cues in daily life can still induce patients’ craving and cause relapse. Better understanding of the causes of craving from the patients’ viewpoint would have potential value to the development of new therapeutic approaches. In this qualitative research, we used SWOT analysis to analyse the internal factors (opportunities and threats) and external factors (strengths and weaknesses) that are closely related to one’s craving and relapse. Overall, our findings are consistent with previous qualitative studies of drug abusers’ experiences about real-life catalysts and barriers contributing to drug-related behaviours during abstinence periods. Regarding barriers to MA abstinence, the main weaknesses and threats identified by participants were peer influence, prevalence and availability of MA, familiar venue of MA use, discrimination, sexual intercourse, alcohol and emotional states, which were in accordance with the studies in New Zealand18 and USA19 However, patients’ feedback on the main strengths and opportunities for maintaining abstinence were the surveillance system, antidrug social workers, vocational skills training, moving to another city and family responsibility. These could serve as count measures targeting those mentioned weaknesses and threats above.
Training patients to better cope with high-risk situations might be of great value. As this SWOT analysis has revealed, patients reported a variety of social and contextual reinitiation-related triggers. These high-risk situations, both internal and external, were very common and almost inevitable in patients’ everyday lives, which also means craving was unavoidable. Considering that many treatments now involve focusing on reducing individuals’ cravings, newly developed interventions targeting improvement of individuals’ coping skills in their social context might be a possible way out.7 However, epidemiological and experimental studies are needed to confirm this hypothesis.
Furthermore, timely follow-up after treatment during the first few months was important, as the participants regarded most of their friends had relapsed during the first 3 months. Similar studies using an electroencephalography technique with cocaine dependent patients also highlighted the first month and sixth month of abstinence as the most vulnerable period.20 Moreover, counting on the highly addictive nature and widespread availability of MA, following up and intensive care via surveillance systems and antidrug social workers might be effective methods to prevent reinitiation of MA.
Even unreal drug stimulus, such as drug-related pictures, can induce patients’ addition bias and craving for drugs.21 To our knowledge, this study was the first to report that patients’ craving could be induced through re-encountering a familiar venue of MA smoking, commodities in everyday life, such as rock candy (‘huang bing tang’ in Chinese), auxiliary equipment used to smoke MA, such as tinfoil, lighters, colourful drinking straws and sexual-related behaviours, by using the SWOT analysis technology. These important findings could provide useful information when screening drug-related cues to optimise craving and MA-related bias assessment and new exposure treatment approaches, such as virtual reality (VR) therapy programmes. VR therapy often uses computer video techniques to simulate the high-risk substance abuse scenes to better induce the desires and cravings,22 before combining psychotherapy and biofeedback treatments23 24 to better help patients cope with the high-risk situations. These key findings could provide useful information when simulating high-risk situations through VR techniques. Moreover, avoiding going back to one’ s most familiar situation of MA smoking, such as the bedroom, hotels or KTVs, is also important for patients when keeping sustained abstinence. Re-encountering these scenes can lead to craving and deterioration of individuals’ abstinence.
Alcohol abstinence treatment is also important, especially for those with comorbidity with alcohol use disorder. Because simultaneous alcohol consumption was common among amphetamine-type stimulant abuse behaviours,25 studies have suggested that alcohol and MA combinations may lead to greater harm, and may even link to aggression.26
MA may affect men and women differently. An interesting finding lies in sexual behaviours. MA abuse and its association with heightened sexual desire, arousal, pleasure, loss of inhibitory control of sexual behaviour and increased sexual behaviours have long been a concern.27 In this pilot study, male abusers turned out to have a much stronger sexual desire as well as sexual fantasies, and are more inclined to have sexual behaviours after smoking MA. Animal experiments have revealed that MA treatment in male rats causes maladaptive sex behaviours.28 However, studies investigating sex difference on sexual motivation have lagged behind.29 Studies investigating the nexus of sex and drug addiction in female and male patients are needed and will help to better advance our understanding of how amphetamine-type stimulants, such as MA, affect males and females differently.30
Limitations
Findings of this study need to be interpreted in light of certain limitations. First, data were self-reported and retrospective, and accuracy of the information may be affected. Second, the study was limited to Shanghai, where socioeconomic status may be different from other parts of mainland China, and thus may not be representative of the patients in other areas. Third, most of the participants were recruited from compulsory isolation detoxification centres; however, according to Chinese antidrug law and their own experiences, they have all received community-based detoxification treatment or voluntary inpatient treatment before receiving compulsory detoxification treatments, which means they have already relapsed at least twice. Therefore, their experience could still effectively compensate for the insufficiency of the other two types of patients.
Implications
This study provides further understanding of why people continue using MA after treatment from the perspectives of abusers. Our study indicated that the first few moments confronting cue-related situations and the first 3 months after therapies have the highest risk for relapse, highlighting the role of self-control abilities and follow-up treatments in helping patients keep sustained abstinence. Moreover, peer influence, widespread availability of drugs, psychological states and combination with alcohol are among the most related factors, and may provide useful insights for preventative and rehabilitative interventions. Specifically, our findings suggest that some articles for daily use such as brown sugar candy, tinfoil paper and appliances used for smoking MA can be applied for harm reduction therapies such as visual reality and cognitive remediation therapy.
References
Footnotes
Contributors YZ and NZ are responsible for the statistical analysis and the writing of the paper. HS and JD are responsible for English language editing. XR, JB and LZ are in charge of transcription interview data. DX, RD and KX help organise the interviews. MZ is responsible for the scientific design of the study. JD and MZ are responsible for the data checking and literature evaluation of the paper.
Funding The study was funded by the National Key R&D Program of China (2017YFC1310400), National Nature Science Foundation of China (U1502228, 81501148), Shanghai Municipal Health and Family Planning Commission (2014ZYJB0002), Shanghai Health and Family Planning Commission Clinical Research Project (20184Y0134), Program of Shanghai Academic Research Leader (17XD1403300), Shanghai Key Laboratory of Psychotic Disorders (13DZ2260500) and Qihang Project of Shanghai Mental Health Center (2018-QH-02).
Disclaimer The funders have no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval All protocols and materials were approved by the Institutional Review Board of Shanghai Mental Health Center.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.