Article Text

Abstract
Background Hyperprolactinaemia is a common adverse effect of antipsychotics (APs). The results of Peony-Glycyrrhiza decoction (PGD) as a potentially useful adjunctive treatment for hyperprolactinaemia are inconsistent.
Aim This meta-analysis of randomised controlled trials (RCTs) examined the efficacy and safety of adjunctive PGD therapy for AP-induced hyperprolactinaemia.
Methods English (PubMed, Embase, Cochrane Library, PsycINFO) and Chinese (Chinese National Knowledge Infrastructure, Wanfang Data) databases were systematically searched up to 10 June 2018. The inclusion criteria were based on PICOS—Participants: adult patients with schizophrenia; Intervention: PGD plus APs; Comparison: APs plus placebo or AP monotherapy; Outcomes: efficacy and safety; Study design: RCTs. The weighted mean difference (WMD) and risk ratio (RR) along with their 95% CIs were calculated using Review Manager (RevMan) V.5.3 software.
Results Five RCTs (n=450) were included and analysed. Two RCTs (n=140) were double-blind and four RCTs (n=409) reported ‘random’ assignment with specific description. The PGD group showed a significantly lower serum prolactin level at endpoint than the control group (n=380, WMD: −32.69 ng/mL (95% CI −41.66 to 23.72), p<0.00001, I 2=97%). Similarly, the superiority of PGD over the control groups was also found in the improvement of hyperprolactinaemia-related symptoms. No difference was found in the improvement of psychiatric symptoms assessed by the Positive and Negative Syndrome Scale (n=403, WMD: −0.62 (95% CI −2.38 to 1.15), p=0.49, I 2=0%). There were similar rates of all-cause discontinuation (n=330, RR 0.93 (95% CI 0.63 to 1.37), p=0.71, I 2=0%) and adverse drug reactions between the two groups. According to the Grading of Recommendations Assessment, Development and Evaluation approach, the level of evidence of primary and secondary outcomes ranged from ‘very low’ (14.3%), ‘low’ (42.8%), ‘moderate’ (14.3%), to ‘high’ (28.6%).
Conclusions Current evidence supports the adjunctive use of PGD to suppress elevated prolactin and improve prolactin-induced symptoms without significant adverse events in adult patients with AP-induced hyperprolactinaemia. High-quality RCTs with longer duration are needed to confirm these findings.
Trial registration number 42016037017.
- prolactin
- peony-glycyrrhiza decoction
- antipsychotics
- meta-analysis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Introduction
Hyperprolactinaemia induced by antipsychotics (APs), defined as an abnormally high serum prolactin level of greater than 25 ng/mL for men and 20 ng/mL for women,1 2 is a common adverse drug reaction (ADR).3 APs induce hyperprolactinaemia by enhancing prolactin secretion through their dopamine-blocking action in the tuberoinfundibular system.4 The prevalence of hyperprolactinaemia is up to 76%–86% in patients receiving AP treatment.5 Hyperprolactinaemia could result in severe menstrual irregularities, including amenorrhoea, gynaecomastia, galactorrhoea, sexual dysfunction, infertility and decreased bone mineral density, all of which would contribute to poor treatment adherence and reduced quality of life.6 7
Several treatment strategies have been suggested to suppress hyperprolactinaemia and improve the associated symptoms, although some of these strategies remain controversial. The frequently used treatment options include (1) dopamine agonists, such as bromocriptine (BMT), amantadine and cabergoline, all of which could induce abnormal involuntary movements;1 8 (2) metformin, which may cause gastrointestinal symptoms;9 (3) aripiprazole, which may cause sedation, insomnia and headache;10–12 (4) using the lowest possible therapeutic dose of AP; however, this strategy may increase the risk of relapse;13 and (5) switching to another AP, risking the occurrence of other ADRs, such as metabolic syndrome and sedation.14 15
In the past two decades growing evidence has suggested that Peony-Glycyrrhiza decoction (PGD), an herbal medicine formula consisting of Paeonia and Glycyrrhiza radices (shaoyao-gancao-tang in Chinese and shakuyaku-kanzo-toin in Japanese, TJ-68), can significantly improve prolactin-induced symptoms in patients with AP-induced hyperprolactinaemia.1 16–22 A number of case reports,21 22 observational studies17–20 and randomised controlled trials (RCTs)16 23–26 of adjunctive PGD for AP-induced hyperprolactinaemia have been published with mixed results.
This meta-analysis set out to assess the efficacy and safety of adjunctive PGD in the treatment of AP-induced hyperprolactinaemia, including recent studies published in Chinese-language and English-language journals.
Methods
Inclusion and exclusion criteria
Two independent investigators (WZ, D-BC) assessed and screened the eligibility of studies based on the following criteria of PICOS: Participants: adult patients with schizophrenia; Intervention: PGD plus APs; Comparison: APs plus placebo or AP monotherapy; Outcomes: the primary outcome measures were efficacy of treatment (serum prolactin level and prolactin-related symptoms: reduction in the severity of galactorrhoea, amenorrhoea and oligomenorrhoea)—key secondary outcomes were improvement of psychiatric symptoms assessed by the Positive and Negative Syndrome Scale (PANSS)27 or the Brief Psychiatric Rating Scale,28 ADRs assessed using the Treatment Emergent Symptom Scale (TESS),29 and all-cause discontinuation; Study design: only RCTs examining the efficacy and safety of adjunctive PGD for AP-induced hyperprolactinaemia. Case report/series, observational studies and meta-analyses and systematic reviews were excluded.
Search strategy
Two reviewers (WZ, D-BC) independently searched PubMed, Embase, Cochrane Library, PsycINFO, Chinese National Knowledge Infrastructure and Wanfang Data for trials evaluating adjunctive PGD for AP-induced hyperprolactinaemia from inception of these databases until 10 June 2018. The keywords used for the searches included the following: (“Peony-Glycyrrhiza” (MeSH) OR paeonia lacliflora and Glycyrrhiza uralensis OR shakuyaku-kanzo-to OR shaoyao gancao OR glycyrrhiza OR paeoniae) AND (“prolactin” (MeSH) OR hyperprolactinemia OR prolactin OR amenorrhea OR menstrual irregularities OR oligomenorrhea OR galactorrhea OR gynecomastia). Reference lists from relevant review articles for additional studies were hand-searched. The two reviewers (WZ, D-BC) independently assessed all trials by judging their clinical, methodological and statistical heterogeneity to decide which ones to include in the qualitative or quantitative synthesis. Any disagreement was discussed with a third reviewer (Y-TX).
Data extraction
Data of each study were independently identified, checked and extracted by the two reviewers (WZ, D-BC). Results based on intention-to-treat were preferred to observed cases data. Inconsistencies were resolved by consensus involving a third reviewer. In addition, missing information was obtained by contacting the first or corresponding authors, or was extracted from graphs or figures of included RCTs if possible.
Evaluation of quality of included studies
The included RCTs were assessed by two reviewers (WZ, D-BC) using the Cochrane risk of bias with seven dimensions as follows: (1) random sequence generation; (2) allocation concealment; (3) blinding of the subjects and the treatment providers; (4) blinding of the result evaluators; (5) incomplete results data; (6) selective reporting; and (7) other potential risks.30 The quality of evidence and strength of recommendations of outcome measure of PGD for hyperprolactinaemia were assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system as ‘very low’, ‘low’, ‘moderate’ or ‘high’.31 32
Statistical methods
The meta-analysis was performed according to the recommendations of the Cochrane Collaboration using Review Manager (RevMan) (V.5.3) (http://www.cochrane.org). For continuous outcomes and dichotomous outcomes, weighted mean differences (WMDs) and risk ratios (RRs) with their 95% CIs were reported, respectively. The heterogeneity of meta-analytic pooling was measured using the χ 2 (p<0.1) or I 2 (<50%) statistics. A random-effect model by DerSimonian and Laird33 was used in all cases. One RCT16 with three study arms was included in the meta-analysis, and in order to include each of the two adjunctive PGD arms separately we included the AP monotherapy condition twice in the analysis, but assigned half of the total patients randomised to each PGD arm in order to not inflate the number of AP monotherapy patients, as recommended by prior studies.34 35
Publication bias was assessed using funnel plots and the Egger’s test.36 All analyses were two-tailed, with alpha set to 0.05.
Results
Search results
Figure 1 presents the flow chart of study selection. Altogether 241 potentially relevant published studies from English (142 trials) and Chinese (99 trials) databases were identified. Of them, three RCTs that compared PGD with BMT,1 Guifu Dihuang pill37 or biperiden,38 respectively, were excluded. Finally, five RCTs16 23–26 were included in this meta-analysis.
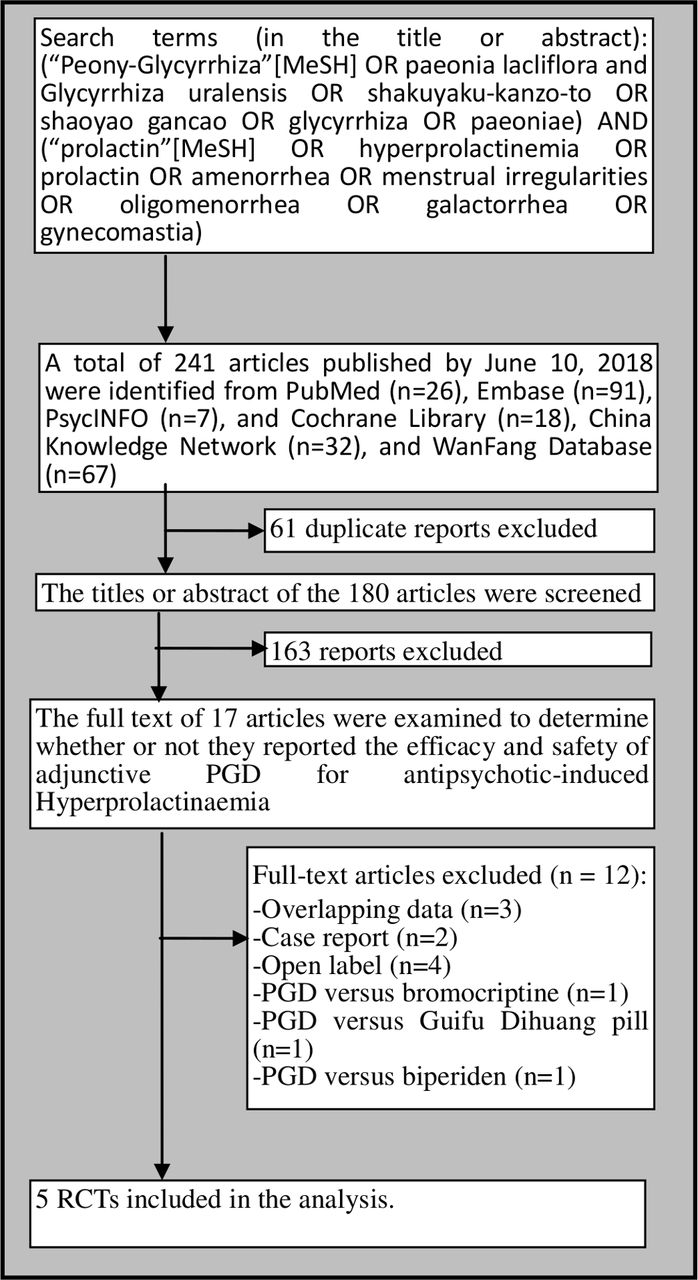
Flow chart of identification of studies. PGD, Peony-Glycyrrhizadecoction; RCT, randomized controlled trial.
Study characteristics
All five RCTs16 23–26 (n=450) were conducted in China (table 1). These RCTs had a sample size of 90.0 (30.6) (range=41–120, median=99) and an average length of 9.6 (4.1) (range=4–16, median=8) weeks. Participants were 30.4 (1.5) (range=28–32, median=30) years old and 80.4% were female. Only one RCT24 mentioned PGD fixed dose (45.0 g/day) (table 1).
Characteristics of the included studies
Quality assessment
Although 80% (4/5) of the RCTs16 23 24 26 reported randomisation methods with a specific description, only one RCT was rated as low risk regarding allocation concealment (table 2). Similarly, 60% (3/5) of the RCTs16 25 26 were rated as low risk in terms of incomplete outcome data. Based on the GRADE approach, the quality of evidence presented for each outcome ranged from ‘very low’ (14.3%), ‘low’ (42.8%), ‘moderate’ (14.3%), to ‘high’ (28.6%) (table 3).
Evaluation of risk of bias in the included studies
GRADE analyses: adjunctive Peony-Glycyrrhiza decoction for antipsychotic-induced hyperprolactinaemia
Efficacy
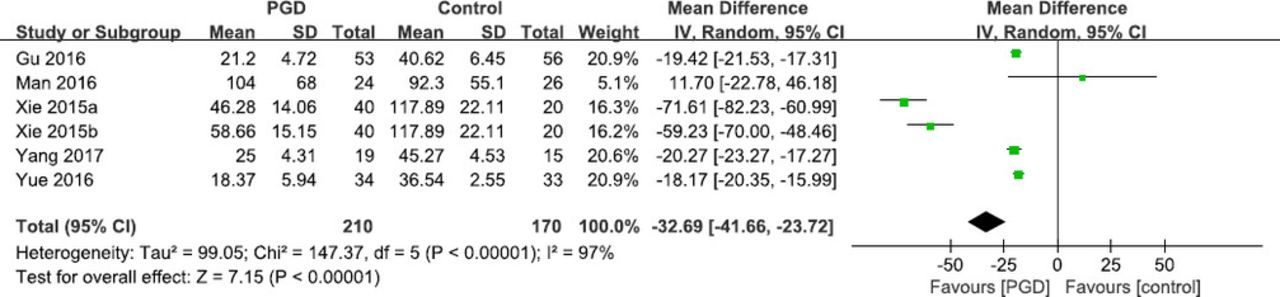
The PGD group had a significant decrease in the serum prolactin level at endpoint compared with the control group (5 RCTs, n=380, WMD: −32.69 ng/mL (equivalent to 693.03 mIU/L) (95% CI −41.66 to 23.72), p<0.00001, I 2=97%; figure 2). Only two RCTs24 25 reported hyperprolactinaemia-induced symptoms. In one RCT,25 79% of patients in the PGD group and 0% in the placebo group reported improvement in hyperprolactinaemia-induced adverse effects. In another RCT,24 68% of patients on PGD and 54% on placebo reported improvement in hyperprolactinaemia-induced adverse effects.

{kind=link}
{kind=link}
Adjunctive Peony-Glycyrrhiza decoction (PGD) for antipsychotic-induced hyperprolactinaemia: forest plot for serum prolactin level at endpoint (ng/mL). IV, inverse-variance.
Psychiatric symptoms
Meta-analysis of PANSS total scores (5 RCTs, n=403, WMD: −0.62, 95% CI −2.38 to 1.15, p=0.49, I 2=0%) showed no significant difference between the PGD augmentation and AP monotherapy groups (table 4).
Adjunctive Peony-Glycyrrhiza decoction for antipsychotic-induced hyperprolactinaemia: secondary outcomes
ADRs and discontinuation rates
Meta-analysis of akathisia, constipation and headache (p=0.53–0.78) found no significant difference between the PGD group and control group (table 4). Similarly, meta-analysis of TESS total score showed no significant difference (n=187, WMD: 6.95, 95% CI −1.23 to 15.14, p=0.10, I 2=99%; table 4).
There were similar rates regarding discontinuation due to any reason between the two groups (4 RCTs, n=330, RR: 0.93, 95% CI 0.63 to 1.37, p=0.71, I 2=0%; table 4).
Discussion
Main findings
To the best of our knowledge, this was the first meta-analysis examining the efficacy and safety of adjunctive PGD for AP-induced hyperprolactinaemia. The main finding was that adjunctive PGD significantly suppresses elevated prolactin and improved prolactin-induced symptoms, which was consistent with the results of case reports,21 22 observational studies17–20 and a systematic review.40 PGD was safe and well tolerated in patients with AP-induced hyperprolactinaemia.
Implications
There are a few possible reasons for the therapeutic effect of PGD on hyperprolactinaemia. First, PGD may directly suppress the elevated prolactin and testosterone production by affecting their conversion processes and the relevant enzymes.1 Second, PGD may modulate the expression of D2 receptor and dopamine transporter.2 41 A recent study42 found that paeoniflorin and liquiritin, both major constituents of PGD, are associated with the improvement of hyperprolactinaemia. Third, PGD may inhibit P450 enzymes that metabolise APs.43 However, the mechanisms underlying PGD for hyperprolactinaemia need to be further explored.
In clinical practice, the prevalence of AP-induced hyperprolactinaemia has been often underestimated due to lack of visible signs of hyperprolactinaemia-related symptoms, patients’ embarrassment with the symptoms and clinicians’ lack of awareness.42 There are no therapeutic strategies approved by the Food and Drug Administration in the treatment of AP-induced hyperprolactinaemia, although meta-analyses12 44 have found that adjunctive aripiprazole and metformin may be effective augmentation strategies reducing elevated prolactin and improving hyperprolactinaemia-induced symptoms. We could not locate any head-to-head trials to compare PGD and aripiprazole/metformin in treating AP-induced hyperprolactinaemia.
Adjunctive PGD appears to be relatively safe and well tolerated. Unlike BMT, a dopamine agonist, adjunctive PGD does not exacerbate psychosis.1 Ota 38and colleagues have found that adjunctive PGD significantly improved extrapyramidal symptoms.
Strengths and limitations of this study
The majority strength of this study is the inclusion of Chinese database in the search. The results of this study need to be interpreted with caution due to several limitations. First, only five RCTs met the inclusion criteria and were included in the study. In addition, the sample sizes were relatively small and the methodology of the RCTs was heterogeneous. Second, half of quality of evidence was rated as ‘very low’ or low’ according to the GRADE approach. However, Guyatt 45and colleagues suggested that low-quality evidence may still result in strong recommendations as strong recommendations are not always based on high-quality evidence. Third, the dose–response effect of adjunctive PGD in suppressing the elevated prolactin was not analysed due to missing information. Fourth, only English and Chinese databases were searched in this review, while relevant studies may have also been published in other languages.
Conclusion
There has been no effective pharmacotherapy for hyperprolactinaemia, a frequent side effect of AP treatment. Evidence from this meta-analysis supports the use of adjunctive PGD in AP-induced hyperprolactinaemia, which has important clinical implications for the treatment of hyperprolactinaemia. Adjunctive PGD is not associated with increased ADR and exacerbation of psychosis. High-quality RCTs of PGD for hyperprolactinaemia are warranted.
References
Dr Wei Zheng obtained a bachelor’s degree from Hebei Medical University in 2012 and a master’s degree in psychiatry and mental health from the Capital Medical University in Beijing in 2015. Since then he has been working as a resident physician in the Department of Psychiatry in the Guangzhou Huiai Hospital. He is currently a PhD Candidate at the Affiliated Brain Hospital of Guangzhou Medical University (Guangzhou Huiai Hospital). His main research interest is depression and schizophrenia.

Dr Dong-bin Cai obtained a bachelor’s degree from Guangzhou University of Chinese Medicine in 2015 and a master’s degree in clinical foundation of Chinese Medicine from Guangzhou University of Chinese Medicine in 2018. His main research interest is depression and schizophrenia

Footnotes
WZ and D-BC contributed equally.
Contributors WZ and Y-TX designed the study and were assisted by D-BC in the search for papers, data extraction and analysis. WZ and D-BC drafted the manuscript. GSU, CHN and Y-TX made critical revisions to the manuscript. All authors approved the final version for publication.
Funding The study was supported by the University of Macau (SRG2014-00019-FHS; MYRG2015-00230 FHS; MYRG2016-00005-FHS) and the Affiliated Brain Hospital of Guangzhou Medical University (2016YFC0906302; 81671334; 2014Y2-00105; 2015BAI13B02). The University of Macau and the Affiliated Brain Hospital of Guangzhou Medical University had no role in the study design, generation or interpretation of the results, and publication of the study.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data statement All the relevant data has been presented in Tables and Figures.