Article Text

Abstract
Background The COVID-19 pandemic has drastically increased demands on healthcare workers (HCWs) leaving them vulnerable to acute psychological distress, burnout and post-traumatic stress. In response, supportive services in a central London hospital mobilised mental health support specifically for HCWs.
Aims This rapid evaluation assessed HCW psychological welfare during the acute phase of the COVID-19 pandemic and their use of supportive services made available.
Methods During the acute phase of COVID-19 (April to May 2020) all staff working for the hospital were invited to complete an online survey assessing well-being (self-rated health, moral distress exposure, symptoms of burnout and psychological distress) and use of available supportive services (awareness of, use and perceived helpfulness). Associations among personal characteristics and psychological well-being were explored using correlations and linear regression.
Results A total of 1127 staff participated in the rapid evaluation. On average, psychological distress was high (mean (SD): 22 (7.57)) regardless of role, with 84% of this sample scoring above the general population mean (14.5). Nearly half of the sample reported feeling emotionally drained and a profile emerged displaying higher levels of psychological distress and burnout in those who were younger and exposed to morally distressing situations, with this group also exhibiting greater support service use. Greater levels of burnout were associated with increased psychological distress when controlling for personal factors. During this acute phase of the pandemic, majority of staff used at least one service and rated it as helpful.
Conclusion HCWs experienced high levels of psychological distress requiring continued support as the COVID-19 pandemic evolved. Although HCWs were aware of supportive services, uptake varied. In order to mitigate the risk of burnout and post-traumatic stress, long-term, effective strategies that facilitate staff accessing support are urgently required.
- COVID-19
- healthcare workers
- psychological distress
- well-being
- supportive services
Data availability statement
Data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The WHO1 categorises COVID-19 as an infectious disease caused by a newly discovered coronavirus. In March 2020, COVID-19 was declared a pandemic2, prompting the UK government to restrict movement across the country and the National Health Service (NHS) to mobilise emergency protocols. Consequently, many staff working in the NHS were redeployed to combat the developing pandemic. Previous research has highlighted the negative impact viral pandemics can have on healthcare workers’ (HCWs) psychological well-being, thus making supporting staff a priority.3 4
Impact of pandemics on HCWs
Previous viral outbreaks serve as effective templates for understanding how COVID-19 may potentially affect HCWs. In particular, SARS, an outbreak of a coronavirus strain, has notable parallels with COVID-19. Research on HCWs working through SARS has shown identifiable patterns of those at risk of poor psychological well-being, which are informative as we work towards creating interventions to support HCWs.3 4 It is important to note that high levels of psychological distress do not automatically result in long-term affective disorders (ie, depression) or post-traumatic stress disorder. Nonetheless, an increase in compassion fatigue and a depowered workforce is a marked concern.5 6 As such, measuring rates of clinical diagnoses in the absence of factors such as psychological distress, burnout and moral distress may limit our understanding of the impact the pandemic is having on staff well-being, particularly in the early phases.
During the severe acute respiratory syndrome (SARS) pandemic, staff working in high-risk areas showed high levels of post-traumatic stress7, emotional exhaustion4 and self-imposed social isolation due to stigma and fears of contamination.8 Systematic reviews have identified that female staff, particularly nurses and more junior staff, were among those most at risk due to overwhelming workloads, having the highest exposure to infectious patients or having less experience compared with more experienced staff.6 9 10 Regardless of profession, fears of contamination were common and were concentrated on fear of transmission to others, particularly among those with children.6 It has also been highlighted that experiences such as redeployment, increased workload, social distancing, social stigma and self-imposed isolation increased the risk of psychological distress.9 10 Such factors are therefore crucial to assess during the COVID-19 pandemic.
During the SARS outbreak no difference was observed in levels of psychological distress between staff with low exposure to patients with SARS and those with high exposure.4 However, 1 year later, stress levels within the high-exposure group were significantly higher than those classed as low exposure. The perceived stress levels in the high-exposure group were associated with higher rates of depressive, anxious and post-traumatic stress symptoms even 1–2 years after outbreak.3 4 Similarly, there was little difference in terms of psychological distress between HCWs who contracted SARS and those who did not.9 After the outbreak was contained psychological distress seemed to increase; with 90% of HCWs who contracted SARS showing significant psychological distress. Up to 2 years after outbreak, levels of HCW psychological distress remained elevated.6 10 This was associated with higher levels of burnout, depressive and anxious symptoms, poor health behaviours (eg, increased drinking), increased sick leave, decreased working hours and disengagement with patient facing work.
Impact of COVID-19: what’s known
Early reports emerging from China and Italy suggested a similar and potentially more severe impact of COVID-19 on HCWs compared with the SARS pandemic.11 12 In Italy, high levels of emotional exhaustion among HCWs were reported.12 In China, reports of poor psychological well-being regardless of exposure to COVID-19 were found.13 However, HCWs with symptoms of COVID-19 display higher psychological distress than non-infected colleagues.14 The relative lack of early understanding of COVID-19’s origin, viral transmission and prevention undoubtedly contributed to HCW psychological distress.15 Moral distress and injury has also emerged as a concern among HCWs as they face psychologically distressing situations that may violate their moral/ethical code.16
High levels of psychological distress have been observed among allied health professionals exposed to patients who tested positive for COVID-19, as well as those redeployed to provide emotional support to patients, family and staff.17 Infrequent viral testing of staff has been linked to elevated stress and fears of unknowingly spreading the virus to family, friends and the general public.18 Furthermore, a seemingly universal profile of HCWs exhibiting poorer psychological well-being has been reported: younger, female, nurses, having children, being redeployed or limited access to personal protective equipment (PPE).14 17 18
Given the residual effects of SARS on HCW well-being, concerns have been raised during the COVID-19 pandemic.13 A recent study in the UK highlighted a risk of service-level burnout in the workforce should the increased clinical pressures arising from COVID-19 continue without intervention.19 Predictors of individual outcomes among HCWs during COVID-19 have yet to be explored18; however, studies have demonstrated a need for strategic and urgent psychological intervention, both on a national and international level, to prevent HCWs becoming secondary victims and leading to mass burnout in the clinical community.12 13 18 19
Current responses to COVID-19
Evidence-based recommendations have been made to protect the psychological well-being of HCWs in the wake of another pandemic which focuses on supporting and building adaptive coping responses at an individual and organisational level.3 4 10 In the early stages of the pandemic, the British Psychological Society (BPS)20 released guidance for supporting the mental well-being of HCWs. The BPS recommended a stepped approach to psychological care proposing that psychological interventions should aim to be built on a strong foundation of communication, safety and leadership. Furthermore, during the preparation and action phases of the pandemic, it was recommended to focus on effective training and support for staff, development of supportive materials and the use of transparent, decisive and effective leadership.6 10 Their approach further called for maintaining peer support networks where possible and to normalise feelings of anxiety.
The BPS guidance outlined that prolonged exposure to the stress of the pandemic may result in exhaustion, leading staff to become disillusioned with the drastic change to their work. During this period, staff may neglect their own well-being and needs, deeming themselves not to be a priority. In response to the COVID-19 pandemic, psychological support services within a London-based hospital were adapted in order to provide timely and responsive care to support HCW well-being. This was aimed to support staff during the acute action phase until a transition into a recovery phase was possible.
In line with BPS guidelines, the hospital’s psychological support services established respite areas on-site and off-site, provided support groups on the wards, offered training workshops, as well as one-to-one support to staff during the acute phase of the pandemic. Additional resources and bespoke toolkits were also developed targeting staff psychological welfare and made available online and via hard copy handouts. All hard copy toolkits and leaflets provided on-site were infection control compliant.
The impact of the COVID-19 pandemic on staff well-being, as well as uptake of supportive services put in place remains unknown. Thus, the main purpose of this rapid evaluation was to assess HCW psychological welfare at one of London’s biggest university hospitals during the acute phase of the COVID-19 pandemic, as well as their use of available supportive services. The secondary objective was to explore factors associated with psychological welfare (eg, personal characteristics) in order to identify potential at-risk groups of HCWs.
Methods
Procedures and participants
All HCWs in one central London hospital (with a workforce of approximately 9000) were invited to participate in a rapid evaluation through hospital-wide communication emails, posters displayed throughout staff areas, handouts distributed to HCWs throughout the hospital and via direct email if provided by HCWs while visiting a respite area (see figure 1, flowchart for enrolment). The bespoke survey was administered using an online survey platform (Qualtrics), accessed via an anonymous link or through a QR code from 21 April to 31 May 2020. Skip logic (ie, questions appeared based on respondent’s answers) was used to ensure that respondents were only asked questions that were relevant to their experience.
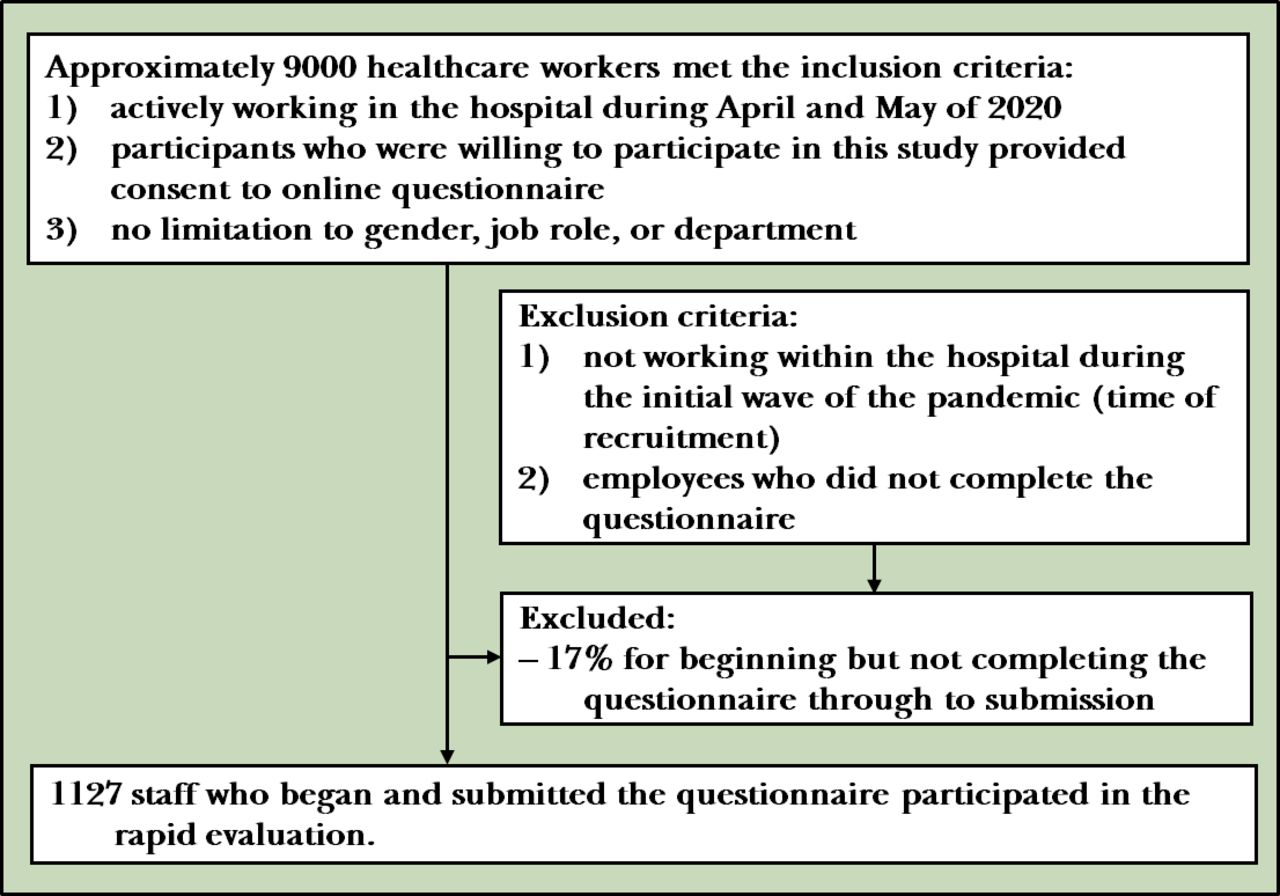
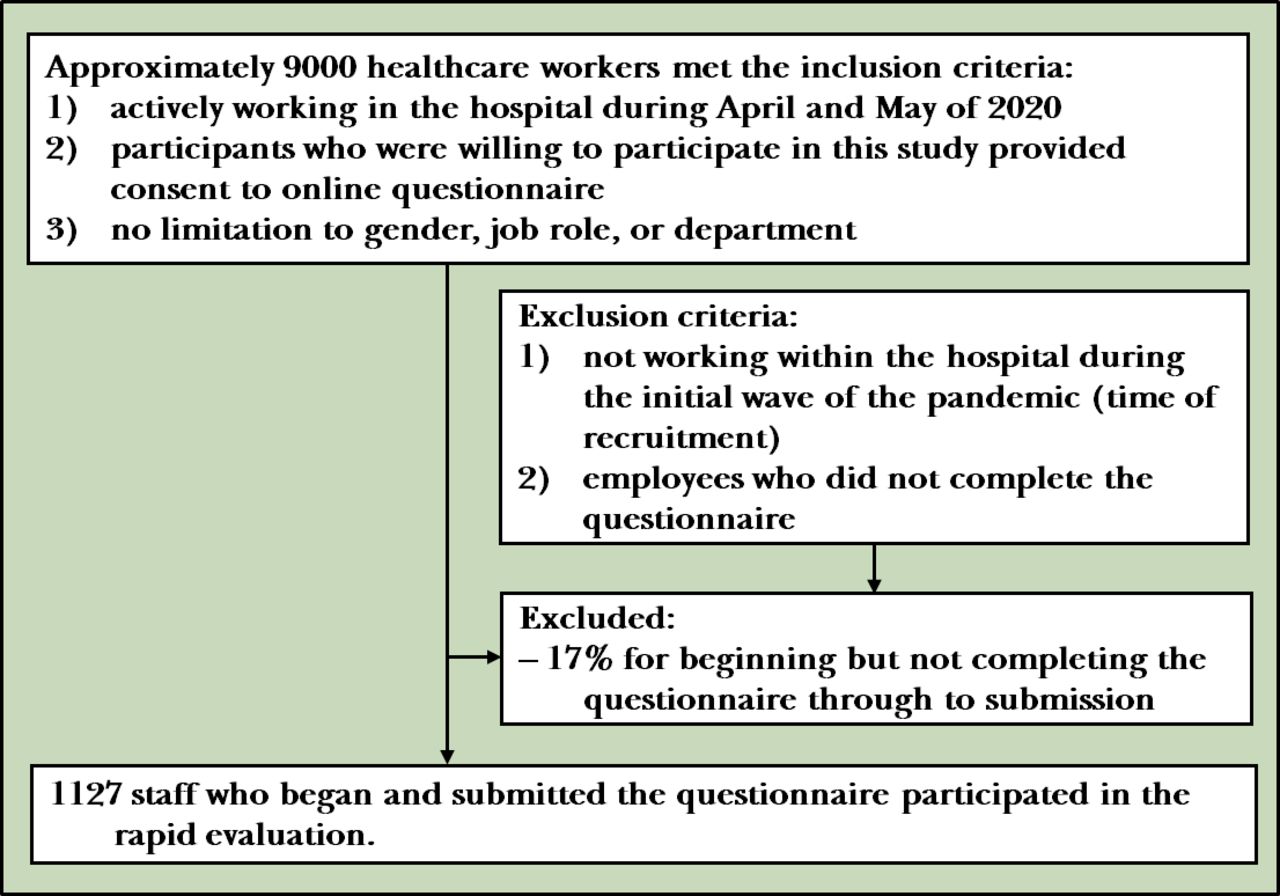{kind=link}
Flowchart for enrolment.
In line with UK regulatory guidance, this project was defined as service evaluation and therefore Health Research Authority approval was not required.21 However, approval from the head of occupational health and the director of workforce was granted, who had oversight of its implementation. Participants were informed that their responses would be kept confidential and reported anonymously, and completion and submission of the survey was implicit of consent. This evaluation is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines (see online supplemental file 1).
Supplemental material
Measures
The survey was an investigator-designed self-report questionnaire containing validated measures adapted for the purpose of evaluation, as well as purpose-built questions.
Personal and professional characteristics
Personal and professional characteristics, as well as exposure to COVID-1922, and caring for individuals defined as high risk/vulnerable by the UK government were examined (table 1).
Respondents’ personal and professional characteristics
Psychological well-being
To assess psychological well-being, four validated measures targeting aspects of moral and psychological distress, burnout and perceptions of health were adapted to fit the needs of this rapid evaluation. To reduce burden on staff it was essential that the survey was brief, so items from validated measures that were not appropriate to the current climate or exhibited small factor loadings were excluded.
Self-rated health
Perceptions of mental and physical health were measured using a single item, whereby respondents rated their health (‘In general, would you say your physical/mental health is’) on a five-point Likert scale (poor to excellent).23 To evaluate pre-COVID-19 heath status, two additional items were adapted from Kang et al22, rated on the same scale (‘In general, would you say your physical/mental health before the COVID-19 outbreak was’). Single-item self-rated health has been shown to be a reliable and valid global assessment of health, as well as an indicator of physical functioning and mental well-being.23
Moral distress
Moral distress was assessed using items adapted from the Moral Distress Scale.24 Items explored frequency of experiencing morally distressing situations (eg, ‘Be required to care for patients whom I do not feel qualified to care for’) on a five-point Likert scale (never to always). If the situation did not apply to respondents in their current role they were instructed to respond with not applicable. When respondents indicated having experienced a situation (rarely to always), they were asked how distressing it was on a five-point Likert scale (not distressing to extremely distressing). A total of seven items were adapted that focused on team communication, self-efficacy, patient workload, goals of care, team competency, administrative support, resources and PPE. Items were designed to stand alone, with no total score, which has shown to be reliable and valid for use in this population.24
Burnout
Burnout was measured using five items adapted from the Maslach Burnout Inventory.25 Items were chosen based on appropriateness and original factor loading scores25, with items for the emotional exhaustion subscale (two items), depersonalisation (two items) and personal accomplishment (one item). Items were rated on a five-point Likert scale (totally disagree to totally agree). One item assessing effective problem solving was reverse coded, allowing for a total score to be calculated whereby a higher score indicates greater symptoms of burnout. The items used have been validated among HCWs.26
Psychological distress
Psychological distress as a global construct, inclusive of symptoms of anxiety and depression, was assessed using the Kessler-10 (K-10).27 The K-10 has been widely used within the general population28, and among HCWs26, and assesses indicators of psychological distress in the past 7 days on a five-point Likert scale ranging from 1 (none of the time to all of the time). The first item was adapted to be COVID-19 specific (‘how often did you get exhausted from the current COVID-19 climate’). A total score ranges from 10 to 50, with higher scores indicating higher levels of psychological distress. Psychological distress is categorised as low (10–15), moderate (16–21), high (22–29) and very high (30–50).27
Service use
Use of available supportive resources and services was assessed using a matrix question whereby respondents indicated if they had engaged with a list of resources (yes/no/not aware of this service). Resources and services listed included those made available by the hospital as well as those provided by other external organisations (eg, NHS Hotline). If the respondents indicated that they had engaged with a specific resource or service, they were asked how helpful they found each resource or service on a five-point Likert scale (very unhelpful to very helpful). For the question related to the provision of free food, donations and care packages, respondents were asked how often they used this resource on a five-point Likert scale (rarely to daily).
Analysis
Data were analysed in R (V.3.6.1).29 Descriptive statistics were calculated (means, medians, SDs or percentages) to fulfil the main objectives. In addition, the level of psychological distress among the general population26 was plotted on the distribution of this sample for comparison. The Wilcoxon test facilitated the comparison of perceptions of self-rated mental and physical health pre-COVID to currently. To address the secondary objectives, Spearman’s r correlations and hierarchical linear regression analysis were used to identify associations among personal characteristics and psychological well-being, as well as factors associated with psychological distress among HCWs.
Results
Respondent characteristics
Table 1 displays personal and professional characteristics. A total of 1127 HCWs responded via the anonymous link (74%), QR code (25%) or personal email invitation (1%). The median time for survey completion was under 10 min and 77% completed the survey in full. Respondents were predominantly female (75%) and living with a partner (56%). Forty percent of respondents managed patients tested positive for COVID-19 in their role, 26% reported displaying symptoms of COVID-19 and <4% indicated testing positive. Overall, the proportion of respondents working in a clinical role was 60%.
Psychological well-being
Self-rated health
Descriptive statistics for perceptions of self-rated physical and self-rated mental health pre-COVID and currently are presented in table 2. Perceptions of mental health were consistently lower than perceptions of physical health. The proportion of respondents who reported their mental health as poor or fair shifted considerably from pre-COVID (17%) to current (47%), with nearly half of the sample reporting poor or fair mental health.
Perception of self-rated physical health and self-rated mental health
A Wilcoxon signed-rank test showed that current self-rated physical health was statistically significantly lower than perceptions of pre-COVID self-rated physical health (Z=−13.02, p<0.01), as was current self-rated mental health compared with perceptions of pre-COVID self-rated mental health (Z=−18.84, p<0.01).
Moral distress exposure
A total of 42% of respondents indicated that exposure to morally distressing situations was not applicable in their current role (reflective of those working in non-clinical roles), 15% indicated never experiencing any of the situations presented and 43% experienced at least one morally distressing situation. Among the most prevalent situations experienced by respondents were poor team communication (60%), insufficient competence of HCWs (50%), a lack of administrative support (48%) and unclear goals of care (48%). Furthermore, 46% of respondents reported experiencing a lack of resources, 41% experienced personal safety concerns (ie, lack of PPE), 39% experienced questioning their qualification/abilities and 35% experienced capacity concerns.
When a morally distressing situation was experienced, levels of distress were high with approximately 75% of respondents rating the situations as moderately distressing to extremely distressing for each of the morally distressing situations.
Symptoms of burnout
Emotional exhaustion was among the most prevalent symptoms of burnout, followed by personal accomplishment and depersonalisation. Emotional exhaustion comprised feeling emotionally drained, which was experienced by 49% of respondents, and feeling burnt out which 38% indicated experiencing. Less than 10% reported feeling uncaring but 23% of respondents experienced feeling hardened emotionally which collectively represent depersonalisation. Positively, 72% of respondents reported feeling able to effectively problem solve at work.
Prevalence of psychological distress
Overall, high levels of psychological distress (mean (SD): 22 (7.57)) were observed in respondents. Psychological distress is categorised from low to very high; 21% of respondents reported low levels of psychological distress, 36% moderate, 27% high and 16% very high. Furthermore, 84% scored above the general population mean (14.5) for psychological distress.26
Service use
Table 3 displays awareness of supportive services, usage and perceived helpfulness. A total of 913 (81%) HCWs responded to these questions, 84% (n=767) indicated having engaged with at least one resource or service. The most commonly used resource was free food, followed by donations and care packages and an off-site respite centre. When these were removed, 58% of respondents indicated having used at least one of the remaining resources or services. Although variability existed on use of each service, proportions of respondents who reported not being aware of a service or resources were consistently low (eg, less than 3% reported not knowing about the hospital’s psychological services). When used, services were perceived as helpful by the majority of staff (eg, 82% of respondents rated the staff support YouTube channel as helpful).
Resources use and perceived helpfulness among respondents
Associations among personal characteristics, service use and psychological well-being
Bivariate Spearman’s r correlations can be found in table 4. Perceptions of health, symptoms of burnout and psychological distress were all significantly correlated with age, gender and years worked at the hospital. Experiencing morally distressing situations was significantly associated with age and years worked at the hospital.
Spearman’s correlations with CIs for the study variables
Being younger was significantly associated with better self-rated physical health, worse mental health, exposure to morally distressing situations and higher levels of psychological distress and burnout (emotional exhaustion and depersonalisation). Identifying as male was significantly associated with better mental health yet higher levels of depersonalisation, whereas identifying as female was significantly associated with greater emotional exhaustion and higher levels of psychological distress. Lastly, being newer to the hospital was significantly associated with poorer self-rated mental health, higher levels of psychological distress, higher levels of depersonalisation and exposure to morally distressing situations.
A significant relationship between service use (exclusive of free food, donations and well-being areas) and identifying as female was observed. The negative relationship between age and service use indicated that being younger was associated with greater engagement with available services. There was a positive relationship between service use and both exposure to morally distressing situations and psychological distress, indicating that the greater the exposure to morally distressing situations and higher levels of psychological distress experienced, the more engaged respondents were in support services.
Hierarchical linear regression model of psychological distress
A hierarchical regression analysis was conducted to determine factors associated with psychological distress (see table 5). In model 1, age, gender and years worked at the hospital were entered as predictor variables for psychological distress. These personal factors statistically significantly predicted psychological distress, F(3, 838)=15.9, p<0.001, R2=0.06. Psychological distress was negatively and significantly predicted by age (β=−0.18, p<0.001; β=−0.09, p<0.01) and positively by gender (0=male; 1=female) (β=0.12, p<0.001; β=0.09, p<0.01). However, years worked at the hospital was not significant.
Hierarchical regression analysis of psychological distress
In model 2, symptoms of burnout, exposure to morally distressing situations and services use (exclusive of free food, donations and well-being areas) were added as predictors. Psychological distress was positively and significantly predicted by symptoms of burnout specific to emotional exhaustion (β=0.36, p<0.001), depersonalisation (β=0.22, p<0.001) and personal accomplishment (β=0.18, p<0.001) but not exposure to morally distressing situations or service use after controlling for age, gender and years worked at the hospital, F(8, 833)=57.88, p<0.001, R2=0.36.
Discussion
This rapid evaluation assessed staff well-being and their use of supportive services during the first acute phase (spring 2020) of the COVID-19 pandemic at a central London NHS Hospital.
Main findings
Engagement from staff, a traditionally difficult population to engage30, was high, as were completion rates. The level of engagement achieved during such unprecedented times suggests that members of staff were keen to engage with this topic, dissemination efforts were effective and the survey was adequately brief. Results showed that perceptions of mental health during the acute phase of the pandemic were poorer compared with pre-COVID-19 and on average psychological distress was high. Nearly half of the sample experienced feeling emotionally exhausted and were exposed to morally distressing situations, which were highly distressing. A profile emerged of possible at-risk populations of staff (younger, female, newer to the hospital) who showed greater levels of psychological distress and symptoms of burnout. Symptoms of burnout predicted greater levels of psychological distress when age, gender and years working at the hospital were controlled for. The majority of staff engaged with at least one support service and ratings of perceived helpfulness were high.
The SARS pandemic has been referred to as a ‘dress rehearsal’10, providing an outline of the impact a pandemic can have on HCW health and well-being acutely and long term. The high levels of psychological distress observed in our sample are consistent with emerging COVID-19 reports suggesting that levels of psychological distress surpass those observed during past pandemics.11–17 In addition, unlike SARS, levels of distress did not differ based on role. Given the circumstances of the COVID-19 pandemic, it may be expected, to some degree, that the negative impact may be greater on HCWs. Further reflecting the unprecedented nature of COVID-19, 84% of our sample of HCWs scored above the general population mean for psychological distress. The widespread impact highlights the need for continued resources for all HCWs regardless of role.
A notable finding emerged specific to perceptions of physical and mental health pre-COVID and during the pandemic. Staff’s explicit perceptions of physical and mental health significantly declined from pre-COVID during the acute phase of this pandemic. Although the proportion of those reporting poor or fair physical health increased from 13% to 24%, the shift in proportions for mental health was more drastic, with an increase from 17% to 47% rating their mental health as poor or fair. This supports the mounting evidence that although physical health is impacted, supporting staff mental health is increasingly important to HCWs.
Exposure to morally distressing situations traditionally associated with burnout and psychological distress30 was reported in less than half of this sample, which represented those working in clinical roles. Of those exposed, poor team communications were among the most prevalent situations experienced. The reason for this is unclear; however, this may be impacted by changes to team dynamics due to redeployment.3 There were also challenges to communication when working in full PPE. Job stress related to redeployment, either from deployment to new teams, areas or specialties, was shown to be a key risk factor for increased levels of distress during SARS.3 4 6 10 Lack of PPE and compromising patient numbers were less prevalent, reflecting the local efforts made to manage these concerns. However, it is important to note that when moral distress was experienced (eg, lack of PPE), the levels of distress experienced were high, as were levels of psychological distress and burnout.
Consistent with the literature on SARS, HCWs reported experiencing feeling emotionally drained and burnt out.3–6 This is a pervasive symptom associated with psychological distress. However, the majority indicated that they also felt able to effectively problem solve at work despite feeling emotionally fatigued. This reflects the acute action-based phase of the pandemic where HCWs may experience an increase in energy and focus engaging in the task at hand, which the BPS cautions expose HCWs to high psychological health risk which could lead to burnout during the recovery phase of the pandemic if unaddressed.20 Interestingly, symptoms of burnout (emotional exhaustion, depersonalisation and personal accomplishment) were significant indicators of psychological distress even after controlling for age, gender and years working at the hospital, whereas exposure to morally distressing situations was not significant. These findings support the need to address burnout as an antecedent to psychological distress among HCWs. Interactions with support services may provide a protective factor for burnout when transitioning into the recovery phase.
This evaluation showed that during the acute phase, the majority of respondents used at least one support service and found it helpful. This is of interest given that engagement with support services is often low in hospital environments.30 Engagement with resources was associated with poorer psychological well-being and higher levels of burnout, suggesting that those who required support were accessing it. This demonstrates a positive paradigm shift in engagement from HCWs around self-care and support of well-being. The most used resources and services (free food, donations and care packages) represent accessible (offered to HCWs working on-site), practical and potentially less stigmatised supports when compared with engaging with other services. Given the nature of free food and respite areas, they were removed leaving 58% of respondents indicating having used at least one of the remaining resources or services. In addition, awareness of available services and resources was high, signifying that efforts to signpost staff to available supports were effective. The protective effect of this in the long term warrants further investigation.
Limitations
In line with existing literature3, a profile emerged of potential at-risk populations of staff, this being those who were younger, female and exhibiting signs of burnout. Encouragingly, staff in at-risk categories were more likely to engage with support services, which is contrary to what was observed in the initial evaluations of the staff at the epicentre of the pandemic in Wuhan.14 15 While we know there are certain risk profiles, this evaluation did not account for the effect of the pandemic on black, Asian and minority ethnic (BAME) HCWs. The risk to BAME staff had been less known when data were collected and warrants further investigation in order to understand potential interactions with psychological well-being and service use. Further key demographic characteristics which warrant investigation include professional (eg, working from home) and well-being constructs (eg, impact of COVID-19 on other life domains that may impact psychological distress, such as childcare). In addition, some clinical and non-clinical groups were under-represented (eg, doctors, cleaners, porters), thus these findings may not represent the experience of all HCWs in the UK.
Implications
Following SARS, the need to support HCW psychological well-being was explicitly emphasised through evidence-based approaches that support and build resilience at an organisational level.3 6 10 As COVID-19 advanced, recommendations made by the BPS to support HCWs were implemented to varying degrees.11–13 19 20 Further work should be undertaken to educate staff on the signs and symptoms of burnout and how to combat this alongside organisational reviews of stressors that impact on staff such as poor intermanagement/team relationships, lack of resources, lack of supervision and training (with protected time for these). While there is currently a renewed interest in support services, historically there has been low engagement from staff. Practical consideration should be taken by leadership alongside modelling engagement to ensure equal access to support services for staff and outreach for those working from home continue with high visibility and accessibility.
In conclusion, the rapid evaluation highlights the high levels of psychological distress experienced by HCWs working during the COVID-19 pandemic. These findings support the need to continue to engage staff in available services aimed at reducing psychological distress in order to mitigate symptoms of burnout long term. Reports following the SARS pandemic3 4 7–9 14, and early COVID-19 reports11–17, warn that symptoms of burnout are expected to increase over time if levels of psychological distress are sustained and there is a lack of intervention. Endorsement of consistent and visible support for HCWs aimed at maintaining physical and mental well-being while in this state of liminality will help keep the workforce strong in the current phase and will aim to mitigate the residual impact of the pandemic on HCWs following its resolution. Thus, continued monitoring of the impact of COVID-19 on HCWs during such an uncertain and unprecedented time is warranted.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Ethics statements
Acknowledgments
Thank you to the research funding bodies for their flexibility during the pandemic to enable researcher time to support this evaluation, including the National Institute for Health Research (NIHR; AP and RMT), Economic and Social Research Council (ESRC; LH) and Teenage Cancer Trust (LAF). Thank you to all the staff at University College London Hospitals who distributed the survey. We are grateful and would like to thank the participants who took the time to complete the survey during a time of unprecedented increased clinical care and pressure.
References
Dr. Anika Petrella obtained her PhD from the University of Toronto in Canada in 2019 and began her post-doctoral research fellowship at the University College London Hospitals (UCLH), Cancer Clinical Trials Unit in the UK in 2020. Working as a Research Associate, Dr. Petrella works with the BRIGHTLIGHT study team on the largest longitudinal study of young people (aged 13-24) with cancer worldwide. This National Institute for Health Research (NIHR) funded study is evaluating teenage and young adult cancer services in England. During COVID-19, Dr. Petrella and her colleagues were redeployed to assist the Staff Psychology and Wellbeing Service (SPWS) at UCLH in evaluating the delivery and use of resources provided by SPWS during the pandemic and the impact of COVID-19 on UCLH staff wellbeing. Dr. Petrella is a Registered Psychotherapist with experience in supportive care program development and evaluation, with a specific clinical interest in helping individuals coping with life stressors.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AP: study design, questionnaire construction, recruitment, data collection, data interpretation, data analysis, literature search, writing. LH: study design, questionnaire construction, data collection, data curation, data interpretation, literature search, writing. LAF: study design, questionnaire construction, data interpretation, writing, editing. LM: study design, recruitment, writing, editing. BH, AW: study design, recruitment, editing. RMT: study design, questionnaire construction, recruitment, data interpretation, writing, editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NIHR, ESRC and Teenage Cancer Trust.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.