Article Text

Statistics from Altmetric.com
Novel zoonosis COVID-19 first emerged in Wuhan, China, but rapidly spread to the other regions in China. The spread of this severe acute respiratory syndrome led to the quarantine of 60 million Chinese citizens. Such isolation measures have been associated with increased depression, stress and emotional disturbance.1–3 However, major traumatic events can amplify both positive and negative aspects of interpersonal relations, leading to competing narratives of both harm and enhancement.4 5 Quarantine can create family dependencies, threaten livelihoods and lead to the stigmatisation of those infected.3 6 School closures and disruption of family care seriously disrupt regular domestic practices.2 7 Domestic abuse may burgeon in a situation of forced confinement.1 2 Community relations may become strained as individuals fear infection from others. Anxiety may quickly spread through social networks via a process of ‘emotional contagion’ in which people ‘catch’ the worry of others.8 At the same time, however, large-scale containment may promote common solidarities.3 6 Romantic relationships can provide a sense of security during a time of existential concern.9 New liaisons may arise within and across communities, with community-level support associated with lower levels of distress.10 At present, it is unclear the extent to which relationship enhancement or decline will apply across different forms of relationships. In this forum, we report early work where we explore the associations between quarantine and reported changes across a range of relationships while controlling for psychological distress.
Data from China during the pandemic
We conducted research to examine this important issue. Following the approval by the ethics committees of the funding institution (Ariel University), a leading market survey company employed a series of internet panels in China to recruit a national stratified sample (4–10 March 2020, n=1134; mean (SD) age of 30.99 (6.82), 53.5% female, see table 1). The sample was collected following an invitation to a number of randomly chosen panellists with recruitment procedures following those established by the ICC/ESOMAR International Code on Market and Social Research. We selected our sample from Hubei Province, Beijing, Shanghai and Guangdong. Two hundred and fourteen participants (19%) were from the Hubei region with 128 from Wuhan city, with deliberate oversampling to include the exposed area in quarantine at the time of the study. One hundred and forty-one respondents began the survey but did not complete it. Figure 1 outlines the sample selection and analysis.
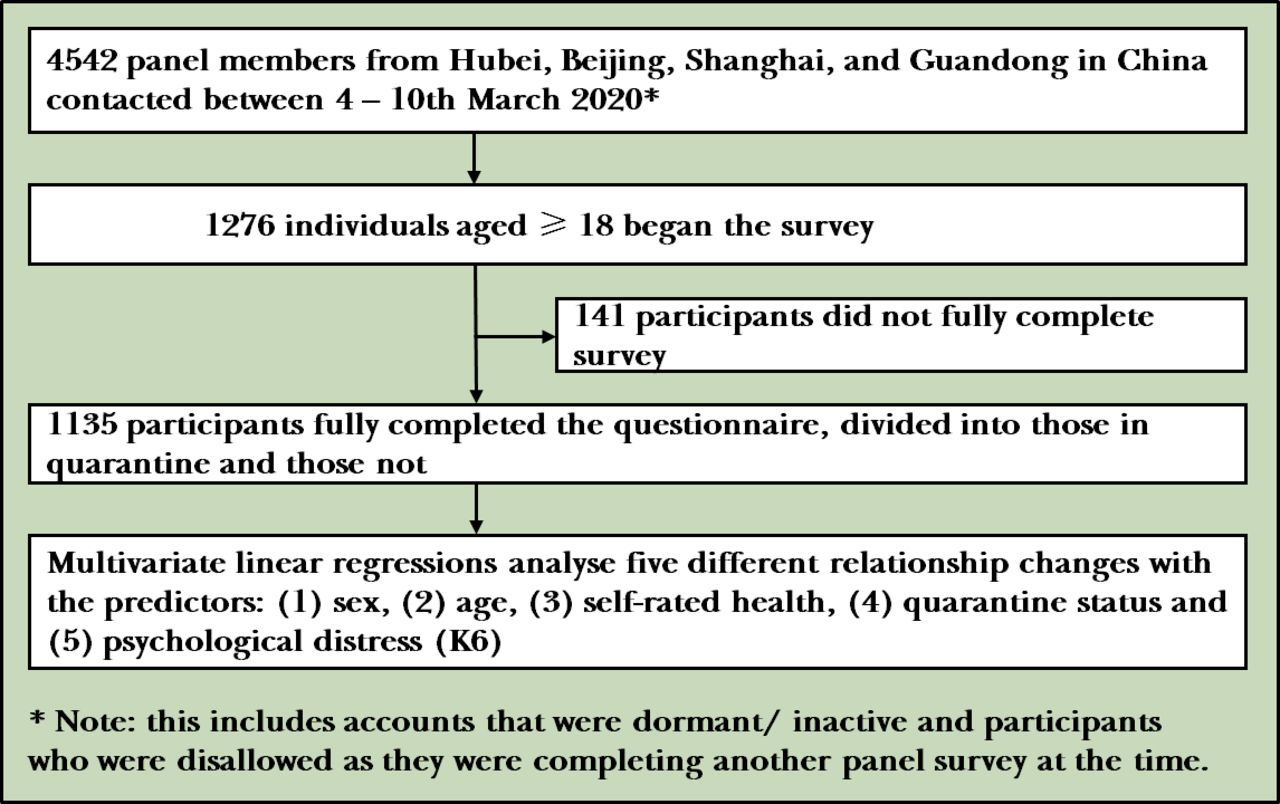
Flowchart of sample selection.
Participant characteristics, COVID-19-related aspects, relationships and psychological distress
We employed a self-report questionnaire and asked respondents to indicate if they were in an intimate relationship, were currently in quarantine (yes/no) and their perceived general health from very bad (1) to excellent (5). Individuals in an intimate relationship were asked to rate the quality of that relationship from extremely unhappy (0) to perfect (6). Perceived changes since COVID-19 were assessed separately for five different relationships: intimate partners, friends, local community residents, Chinese within China and Chinese outside the country (5-point scale; from much more distant than before (1) to much closer than before (5), with 3 indicating no change). Psychological distress was measured using the six item Kessler distress scale (K6, Cronbach’s α 0.90).11 Scores ranged from 0 to 24, with a cut-off of ≥13 indicating risk of severe mental illness. Online consent was obtained for all participants.
For our analysis, descriptive statistics described improvements or decline in each partnership type since COVID-19 (namely, relations with partners, friends, the local community, Chinese in China and Chinese outside China). Five multivariate linear regressions were conducted through SPSS (V.25) with the following predictor variables: (1) sex, (2) age, (3) self-rated health, (4) quarantine status and (5) psychological distress (K6, Kessler distress scale) and with each of the relationship changes as outcome variables. Additional analyses of variance compared each relationship change by quarantine status (yes or no), after controlling for age and sex. Of the 1276 participants who saw and commenced the survey, 1135 (89%) completed the questionnaire. One hundred and forty-two respondents were in quarantine at the time of the study, and 893 participants were in a partnership. Two hundred and seventeen respondents (19.1%) were judged to be at risk of severe mental illness (K6 ≥13). Across the sample, respondents were most likely to say their partnership improved (better or much better) since the COVID-19 outbreak (53%), while a decline (worse or much worse) was the most cited answer for relationships with friends (37%), local residents (46%), other Chinese in China (38%) and Chinese internationally (50%; figure 2).
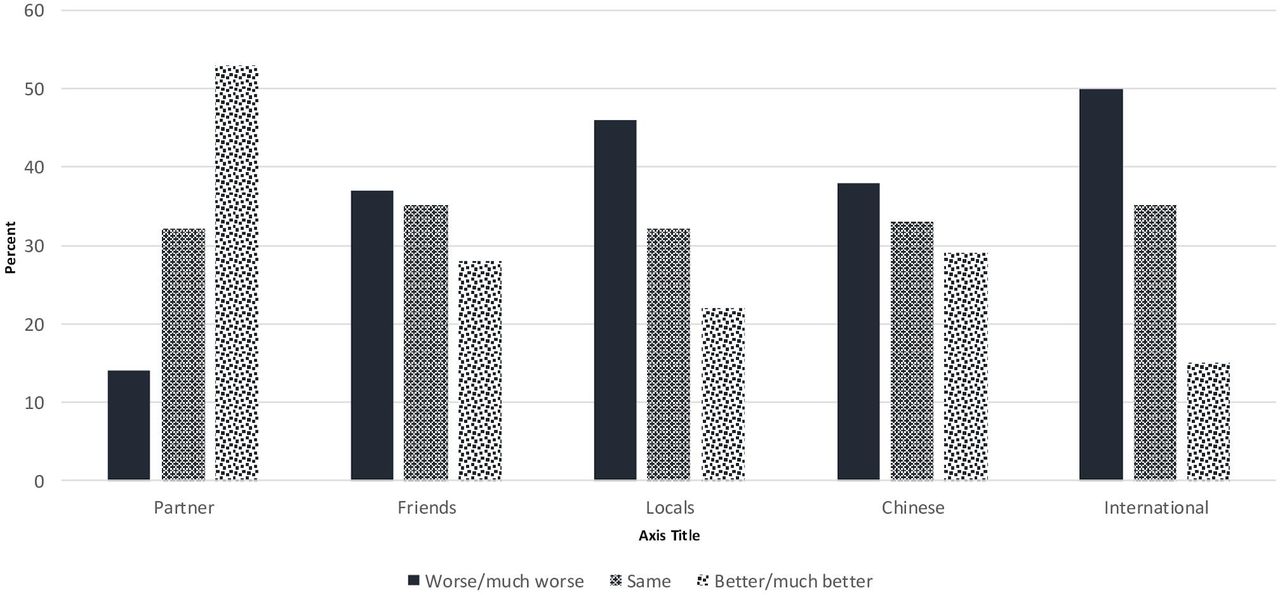
Perceived relationship change since the onset of COVID-19 (percent).
Using regression analyses, we found that being in quarantine was associated with relationship improvement for all except intimate partnerships, for which there was no significant effect (table 2, figure 3). Elevated psychological distress was negatively associated with relationship improvement for partnerships but positively associated with the improvement in relationships with friends, the local community and Chinese internationally (table 2). Good self-perceived health was positively associated with improvements with local communities and Chinese within China. Younger respondents reported improved relationships with all but their partners, for which there was no statistical association (p=0.76); male respondents reported improved relationships with local community and Chinese internationally.

{kind=link}
{kind=link}
{kind=link}
Relationships by quarantine status. Controlling for age and sex. Bars indicate SEs. Scored on a five-point scale from much worse (1) to much better (5); 3 indicates ‘no change’ in relationship.
Associations between relationship change, distress and quarantine status (multivariate regressions)
Interpretations and implications
COVID-19 provides an important challenge for interpersonal relationships across societies. The introduction of lockdown restrictions has provided alternative narratives, raising concern over domestic violence but also suggesting greater societal cohesion. In our preliminary study, we found that although relationships in general did not improve during the outbreak, psychological stress and being in quarantine had mixed effects, depending on the relationship type. For intimate partnerships, high levels of stress were associated with relationship decline. However, for relationships beyond the partnership, psychological stress and being in quarantine had a positive impact. Younger respondents were more likely to report relationship enhancement with friends, the local community and Chinese internationally as a whole; good general health was also associated with improved friendships and relations with the Chinese community locally and internationally.
How can we interpret these findings? First consider our findings on intimate relationships. Mortality salience can lead to a desire for long-term, committed relations and the avoidance of conflict during times of anxiety.9 Those already in close interpersonal relationships may benefit from negotiating the challenges of COVID-19 as a couple. A decrease in divorce rates has been reported following other shared traumas.12 More than half of our sample reported an improvement in their partnerships as a consequence of COVID-19. However, this benefit was not evident for the most stressed individuals, whose partnerships declined. Supplementary regression analysis, which included the item on partnership quality (rather than change), found a negative correlation between distress and positive relationship change, which persisted when controlling for relationship quality, with no significant curvilinear effect (online supplemental table 1: quadratic term for K6: B=0.002, t=1.67, p=0.10). For those confined with their partners, domestic abuse has become a particular concern, as individuals have little possibility of escaping the home.1 2 Further research could explore this risk using more detailed questions on dyadic interactions during the pandemic. This work should also include further potential contextual contributors (eg, size of residence and number of inhabitants).
Supplemental material
We also discovered that an overall positive change in relationship was less evident for relationships beyond the intimate partnership. This may reflect a deterioration in perceptions of the reliability of others over time, with the aid received being below expectations as health and support systems became overburdened.13 This could also result from anger or distrust towards official information sources6 and the strains of having to maintain physical health while continuing other daily activities. However, the impact of quarantine or psychological distress per se did not negatively impact relationships. Quarantine creates new dependencies. For those unable to leave their homes, social support can provide a critical resource during collective trauma.14 Social media, such as WeChat and Weibo, can play a vital support role in providing emotional and informational support,6 while practical support (eg, for shopping) meant the establishment of new voluntary and commercial interactions. These novel associations extended beyond regular routines, ranging from new medical procedures (eg, telemedicine) to online teaching resources and even the provision of voluntary house-care for pets. Almost one-fifth of our respondents reported high levels of psychological distress, scoring above the K6 cut-off for severe mental illness. This prevalence is higher than that reported after natural disasters (eg, Japan, a year after the Great East Japan Earthquake).15 Enhanced levels of stress were associated with relationship growth for all relationships beyond the intimate dyad. Faced with significant threat, perceived vulnerability may lead to the appreciation of benefits provided by wider communities.
We recognise this early work had several limitations. Only 142 respondents in our study reported they were currently in quarantine. Data were self-reported, and we lacked data on pre-existing conditions that may exacerbate quarantine anxiety and post-quarantine adjustment.6 Many potential participants to the survey had dormant or inactive accounts or were disallowed as they were completing competing tasks for their survey panel, limiting response rates. We also lacked data on relationship quality before the outbreak or wider contextual factors (eg, occupation, potential exposure to the virus). We did not assess viral status of the respondents or others in their household. Our study was cross-sectional; support availability and relationship dynamics are likely to change as any quarantine period continues.
We do believe, however, that this work has important implications, as well as raises important questions for further research. The mortality and morbidity resulting from SARS-CoV-2 will no doubt have a long-lasting psychological toll. Lockdown and quarantine measures may continue to increase depression and distress.3 For those suffering domestic abuse, there is an urgent need to identify and provide means of support for those confined to the home.1 Social media may provide valuable support,2 as can national programmes that draw on community response.16 Despite this, for those facing the most serious restrictions, relationships may provide valuable tangible and emotional support. Existing ties with family and friends can be profitably consolidated.17 Regularised virtual interpersonal interactions, and new preventive routines, can help attenuate the initial psychosocial impact of the epidemic. This may be particularly important for older individuals and those in poorer health, the least likely to report a positive relationship change. The long-term efficacy of such support on mental health needs further evaluation, alongside physical and cognitive daily activities to promote mental health.6 Further work should consider the impact of different forms of quarantine arrangements, both voluntary and involuntary, in different physical environments and across nations.1
Acknowledgments
The survey research conducted in this paper was carried out by Asia Opinions using their established panels.
References
Robin Goodwin is a professor in Psychology, University of Warwick, and former Chair of the Warwick Psychology Department. His research focuses on the impact of large-scale societal transitions and threats on our relationships with others and our everyday psychological processes. Recent projects include a Leverhulme Trust sponsored six-wave prospective study of refugees from the Great East Japan Earthquake (with Tohoku University), an investigation of the impact of the 2015 terror attacks in Paris on interpersonal relationships with family, friends and the wider Muslim community and a cross-cultural investigation on the relationship between the everyday social interactions of poultry farmers and the spread of avian influenza in India and China (with Shiv Nadar and Fudan Universities). He is currently working with colleagues at the WHO/OECD on public health responses to major radiation emergencies and collaborating with universities in Thailand, US, Malaysia, Israel and China on SARS-Cov-2/COVID-19.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RG and MB-E designed and supervised the study. MB-E acquired funding and the study data. RG, MB-E and SS analysed and interpreted the data. RG, MB-E and WKH drafted the manuscript with further critical revision by SS. Further administrative and technical support was provided by SS and WKH.
Funding This work was supported by an internal fund from the Research Authority in Ariel University (RA2000000106).
Disclaimer The sponsors had no role in the preparation of the data or the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Participants gave their written informed consent online and the study protocol was approved by Ariel University’s ethics committee on human research.
Provenance and peer review Not commissioned; externally peer reviewed.