Article Text

Abstract
A seizure is one of the most uncommon severe adverse side effects of antipsychotics. Clinical recognition rates for it are low, especially for psychomotor seizures. The authors present a case of psychomotor seizure caused by amisulpride to treat schizophrenia. A 60-year-old male patient in our hospital experienced a recent onset of repetitive, stereotyped involuntary and unconscious movements that began with amisulpride use. All of the symptoms disappeared following amisulpride withdrawal. His Naranjo Adverse Drug Reactions Probability Scale Score was 5 points. The case sheds light on the clinical risk of seizures related to antipsychotics.
- Schizophrenia
- Psychology, Medical
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
A seizure is a severe potential adverse effect of antipsychotic therapy. While antipsychotic-induced seizure is uncommon, it is not rare. Reports have indicated that antipsychotics can cause clinical seizures in 0.5%–1.2% of patients without a history of epilepsy and can produce isolated electroencephalogram (EEG) abnormalities in 7% of patients.1 2 The low rates of clinical recognition of antipsychotic-induced seizures can be partially attributed to the peculiarities of psychiatric illness and the complexity of symptoms. However, the diversity and atypicality of psychomotor seizures further confuse and complicate the diagnosis.
Though uncommon, identifying epilepsy caused by antipsychotics is critical. Epileptogenic side effects could lead to potentially extreme consequences, such as ictal and interictal cardiac arrhythmias, respiratory derangements (including asphyxia), eventual death, or even sudden unexpected death in epilepsy.3 Understanding how such problems can be avoided and successfully managed is essential. This article reports on a case of psychomotor seizure caused by amisulpride.
Case report
The patient was a 60-year-old man with schizophrenia who had been continuously hospitalised for 8 years because of persecutory delusions and disorganised behaviour. He had no history of overt brain disease, drug intoxication or withdrawal, and there were no apparent abnormalities in his physical examination, blood examination or electroencephalogram (EEG). His diagnosis was based on the International Classification of Diseases, Tenth Revision (ICD-10).4 The patient had remained stable throughout much of the hospitalisation and was generally quiet and passive with oral medication treatment. However, he displayed some new, involuntary movements that occurred irregularly from twice weekly to once a month in the past 6 months. The psychomotor seizures would often begin with his suddenly staring into space, and this behaviour would last from half a day to one day and a half.
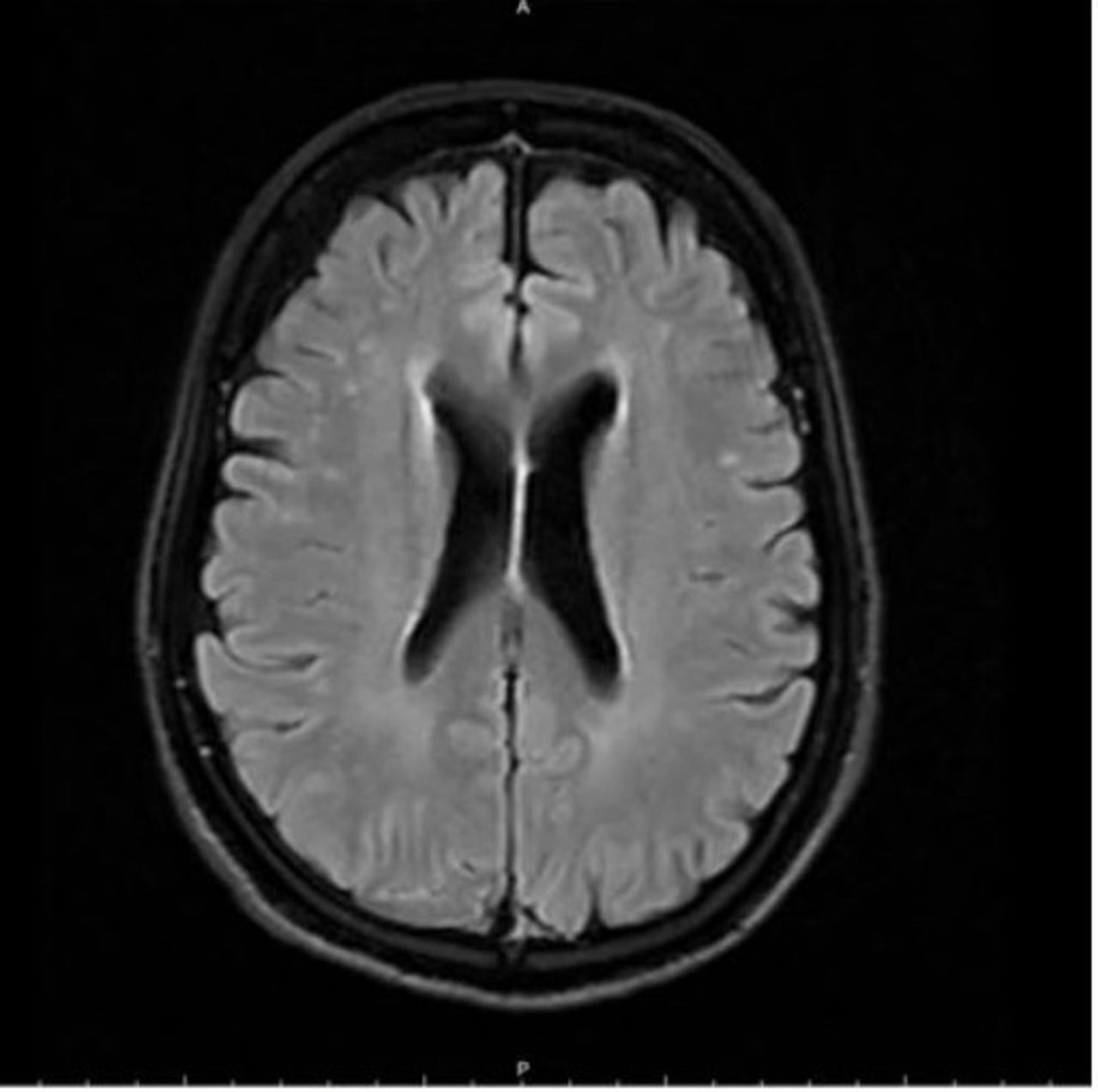
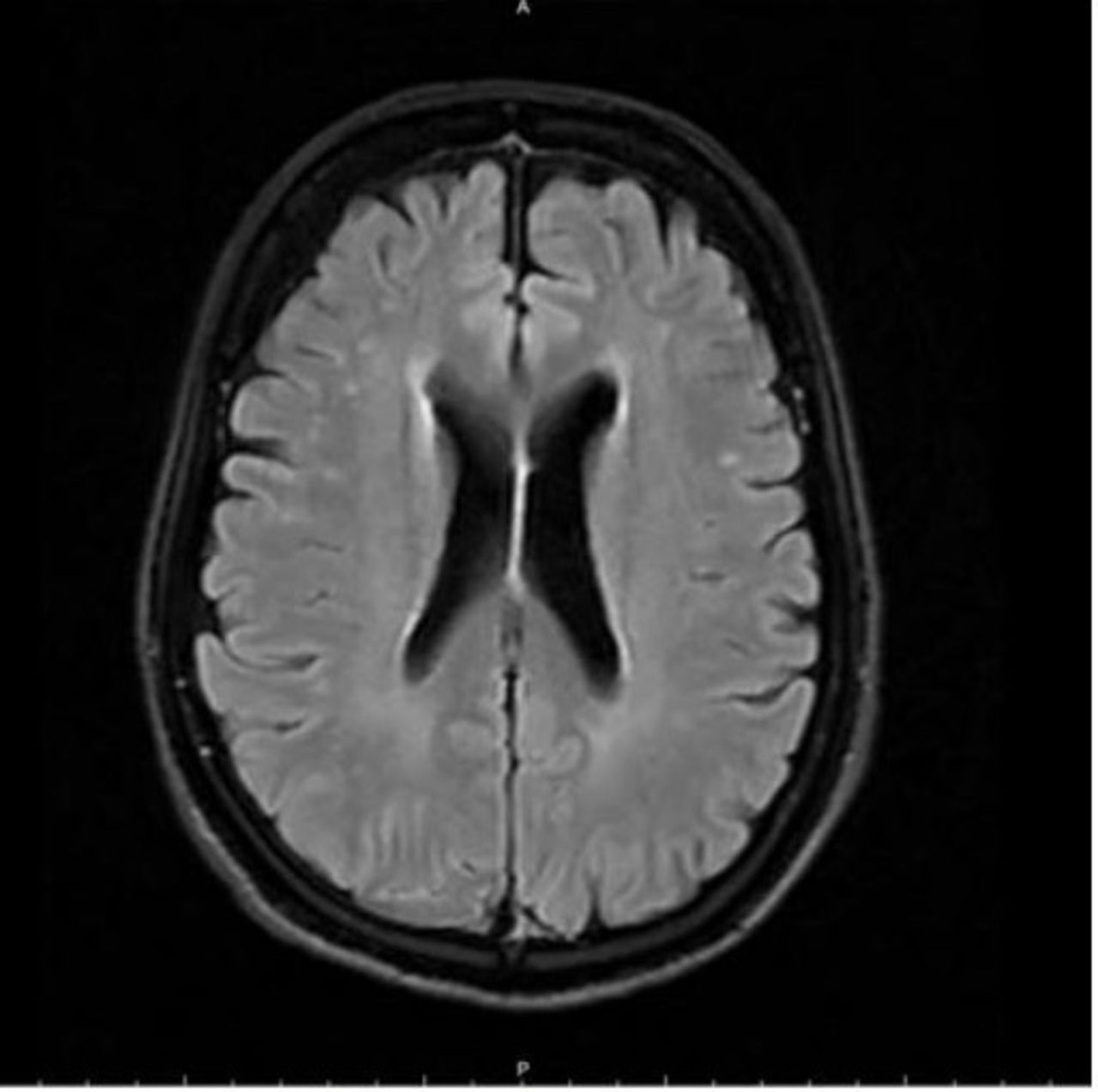
Before the onset of the attacks, he often showed some warning signs: strange behaviours, such as buttoning and unbuttoning his clothes, picking at his clothes, or searching for some objects. The duration of the attacks gradually increased from 20 s to 30 min or even longer. Over time, his movements simplified into a pattern: first, he turned his neck to the left, raised his head, and then, with his eyes staring to the left, used his left hand to search for his belt; second, he turned his neck to the right, raised his head, and then, with his eyes staring to the right, used his right hand to search for his belt; next, he paused for a break, slightly panting with increased respirations; and then, he continuously repeated this sequence of behaviours. During the intervals between the episodes, the patient remained conscious and was able to answer simple questions. But during the attacks, he appeared to be unresponsive and occasionally was incontinent of urine; both pupils were dilated and slow to react to light. Due to his stereotyped behaviours and involuntary movements, a magnetic resonance imaging (MRI) of the head and an EEG were organised to rule out any organic pathology, despite the absence of a history of seizures, as shown in figures 1 and 2. Neither the EEG nor the MRI scan showed any anomalous change.

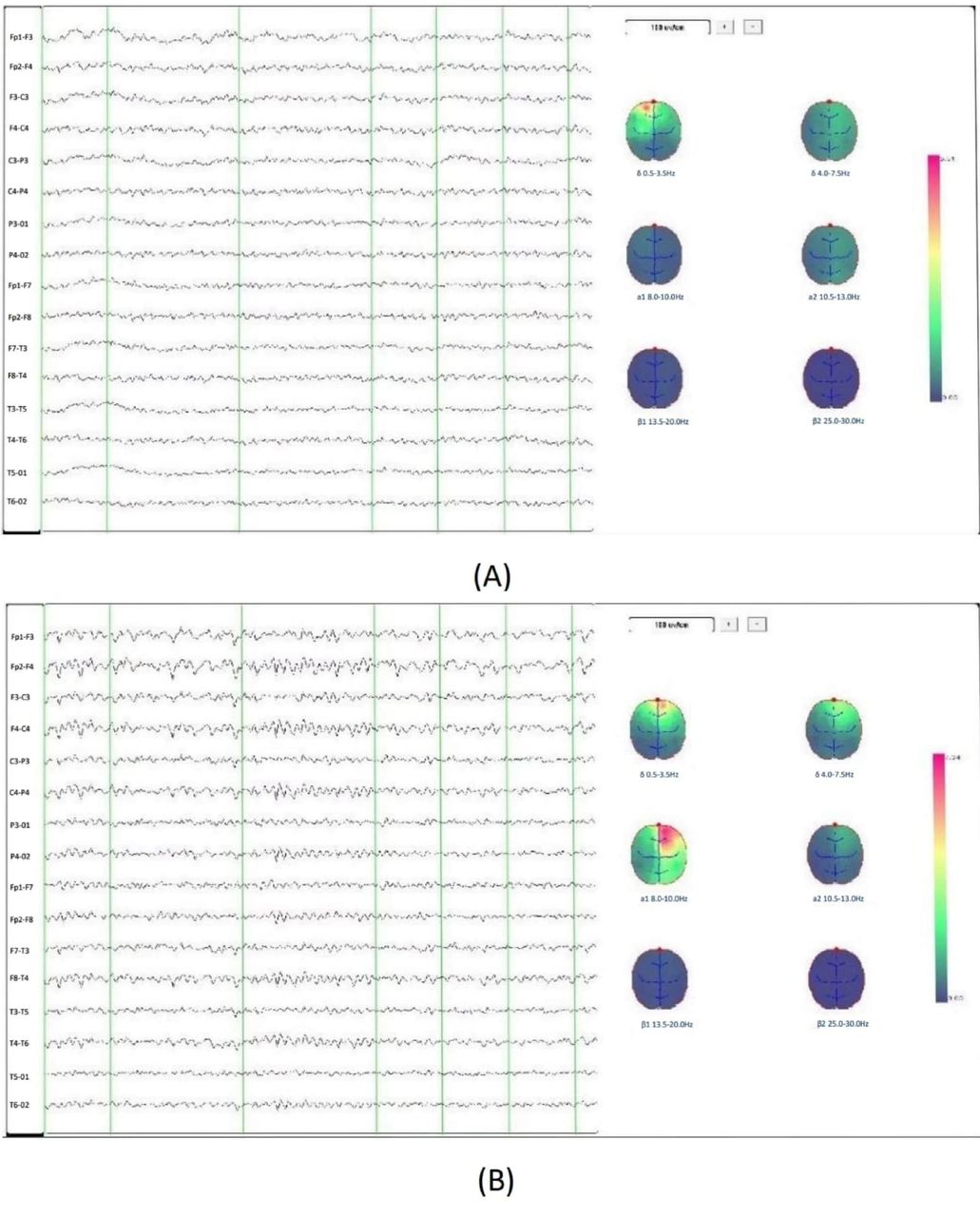
EEG of the patient. (A) EEG without amisulpride use. Increased delta and theta rhythms with no epileptiform discharge; (B) EEG with amisulpride use. Increased delta and theta rhythms with no epileptiform discharge. EEG, electroencephalogram.
{kind=link}
{kind=link}
Normal MRI scan of the patient with antipsychotic-induced psychomotor seizures. MRI, magnetic resonance imaging.
In the past 2 years, olanzapine tablets and amisulpride were administered successively to control his psychotic symptoms. A summary of the medication use is shown in the online supplemental figure 1. The patient had taken olanzapine for a prolonged time to stabilise his mental symptoms. However, at the end of 2018, his creatine kinase and creatine kinase isoenzymes began to increase slowly. Starting in early 2019, his physicians gradually reduced the olanzapine dosage so they could later introduce the antipsychotic drug amisulpride. By March 2020, the olanzapine dosage had been successfully reduced to 10 mg/day, and the patient’s creatine kinase and creatine kinase isoenzymes returned to normal levels as expected. His physicians then started amisulpride and increased it gradually. With the increasing dosage, the patient’s creatine kinase and creatine kinase isoenzyme levels again began to rise, and almost simultaneously, the patient started frequently exhibiting the abovementioned involuntary movements. However, there was no obvious abnormality in the EEG.
Supplemental material
Because of the significant time correlation between the onset of the patient’s epileptiform seizures and his amisulpride use, the clinicians considered the possibility of adverse antipsychotic reactions and that the patient could be harbouring covert epilepsy. His amisulpride dosage was gradually reduced to cessation, while at the same time, the amount of olanzapine was increased to 10 mg/day to stabilise the patient’s mental symptoms. Within 1 week after implementing the above medication regimen, the patient’s seizure frequency had decreased to once every 2 weeks; the duration of seizures decreased to a span of several hours up to 1 day. The creatine kinase and other indicators steadily reduced to stable levels (205 U/L), and the patient’s mental symptoms were well controlled. To date, the patient has been followed up for 5 months; he has had none of the involuntary repetitive movements in the recent 2 months. Also, no obvious abnormality was found in a retest of the EEG. The Naranjo Adverse Drug Reactions Probability Scale was used for monitoring adverse drug reactions;5 the patient’s score of 5 points showed that the causal relationship between amisulpride and his psychomotor episodes was ‘probable’ (table 1).
The Naranjo Adverse Drug Reactions Probability Scale and the patient’s score*
Discussion
The patient described in this case had used olanzapine for a lengthy period to stabilise his mental symptoms; no apparent drug side effects were seen except for an elevated creatine kinase. The patient began to have repetitive, stereotyped involuntary and unconscious movements within half a year after starting amisulpride. These behaviours were accompanied by aura symptoms and disturbances in consciousness, which the patient could not recall after the episodes. The attacks usually lasted several hours to several days. However, the psychomotor seizures disappeared after the slow cessation of amisulpride when olanzapine was increased. By excluding other possible neurological diseases, it was reasonable to consider that the patient’s psychomotor seizures were caused by amisulpride.
It is well known that antipsychotics lower the seizure threshold, but until now, research that focuses on the epileptogenic side effects of psychotropic drugs has been limited. Thus, we can only postulate about the cause-and-effect relationship between amisulpride (or any other type of antipsychotic) and epileptogenic side effects. Isbister found a 4% likelihood of seizure in patients with schizophrenia or schizophrenia-like psychosis who overdose on amisulpride.6 Eli Lilly, the pharmaceutical company that produces antipsychotic drugs such as Zyprexa and Symbyax, showed an approximate seizure rate of 0.88% in patients in its product data sheet.7 Bloechliger investigated 60 121 patients with psychiatric illnesses selected from the 1998–2013 British Clinical Practice Research Database: 90.8% had an affective disorder or dementia, and 3% had schizophrenia. He estimated that the incidence rate of seizures per 10 000 person-years for patients currently receiving monotherapy with amisulpride was 39.8 (95% CI: 4.9 to 74.7), and for all patients using any single antipsychotic was 38.0 (95% CI: 31.1 to 44.9).8
There are few rigorously controlled studies that focus on a single disease and a single drug, limiting the confidence necessary to draw firm conclusions. Most information on antipsychotic-induced seizures has come from spontaneous reports, pharmacovigilance systems and poorly controlled clinical practice research databases. Though current data are insufficient to strictly compare the adverse reactions of different psychotropic drugs, results consistently show that second-generation antipsychotics carry a higher average risk of seizures than first-generation antipsychotics, even when eliminating the one with the black box warning—clozapine.9
Considering the low incidence rate of psychomotor seizures induced by antipsychotics, they are particularly challenging to identify. Complex partial seizures (formerly called psychomotor seizures) are characterised by impairment in consciousness and bizarre, repetitious movements called automatisms. The likelihood of recording a seizure during a routine EEG is small. Data from general hospitals showed EEGs have a low yield in identifying epilepsy, estimated between 25% and 56%.10 To recognise epileptic events in individuals with schizophrenia is further complicated as they may be less able to communicate changes in consciousness and perception. However, detecting such changes by observation alone is difficult, particularly regarding partial epilepsies. Experts solely using visual clues could only get a 30% accuracy success rate for establishing the diagnosis of epilepsy versus non-epilepsy.11 12 Diagnostic sensitivity can be enhanced by using suggestion techniques based on hyperventilation and photic stimulation during an EEG. In addition, intensive observation with video-EEG monitoring can often help determine a diagnosis in confusing situations, like those with stereotyped behaviours and involuntary movements, but the monitoring is carried out in an expensive, artificial environment. But even with these technological advancements, research findings indicate that the atypical symptoms and the low rate of incidence limit seizure identification.13 Successful detection was related to events characterised predominantly by motor manifestations, whereas failure was characterised mainly by subjective sensory symptoms with few or no motor manifestations. Thus, the clinical observation of clinicians still occupies a crucial role.
The relationship between epilepsy and psychosis is very complex: they are independent of each other, but their high rates of comorbidity cannot be ignored. For centuries, it was thought that epilepsy and psychosis may each arise out of some form of neuropathological or physiological dysfunction common to both. The psychoses of epilepsy represent an important medical model for understanding the pathophysiology of psychosis.14 Both epilepsy and psychosis share a common anatomical substrate with neurodevelopmental abnormalities involving the mesial temporal lobe.15 Structural and functional neuroimaging showed frontal-limbic dysfunction in schizophrenia-related and epilepsy-related psychosis. Butler describes a theoretical framework in which frontal hypoactivity and intermittent medial temporal hyperactivity play critical roles in the aetiopathology of psychosis—whether or not is it associated with epilepsy—and proposes a 'two hit' model of psychosis in epilepsy, requiring both aberrant limbic activity and impaired frontal control.16 Research on these related mechanisms is scarce. However, one study suggested that amisulpride exerts a seizurogenic effect on mice possibly via an opioid receptor activation-dependent.17
The defect, in this work, is mainly due to equipment limitations. Other objective methods, such as lumbar puncture and psychological evaluation, would assist in investigating the aetiology. Moreover, studies about therapeutic drug monitoring (TDM) of atypical antipsychotics have shown that adverse reactions, such as extrapyramidal symptoms or epilepsy, may be drug concentration-dependent; their recommendations include the use of TDM for the following drugs: amisulpride, clozapine and olanzapine. By regular TDM, psychomotor seizure can be identified earlier and treated more promptly.18 While diagnosis and management of antipsychotic-induced psychomotor seizures remain challenging, specific evidence-based guidelines exist to optimise patient care. For example, monitoring the drug concentration, starting small doses of drug titration, increasing the dosage slowly and paying attention to high-risk groups can be helpful.19
This case report sheds light on the risk of seizures related to antipsychotics. For many years, adverse seizure reactions had been considered unique to clozapine.20 Few studies have reported cases of psychomotor seizures caused by other antipsychotics used to treat schizophrenia. We have described the cause-effect relationship between amisulpride and seizures and detailed the challenges of recognising the risk for this adverse severe side effect. Recommendations for future studies include obtaining serum levels of antipsychotic medication to measure seizure risk and compiling more data attained from video EEGs. In conclusion, we emphasise that although epilepsy caused by antipsychotics is uncommon, awareness of its clinical manifestation can lead to earlier identification and more timely intervention.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but ethical approval was exempted for this study. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors thank the patient presented in this case report and his family.
References
Yanqun Zheng completed her medical graduation from Jinan University, Guangzhou, China, in 2016. She received a master's degree with Prof. Xiaohua Liu in psychiatry at Shanghai Jiao Tong University School of Medicine in 2019. Since then, she has worked at the Shanghai Mental Health Center and is currently undertaking her psychiatry training (residency). Her main research interest includes the biomarker research in schizophrenia and mood disorder.

Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors YZ wrote the manuscript and performed initial and follow-up psychiatric care. Author XL offered many constructive opinions on this study and provided a critical revision for the manuscript. Author MJ provided overall supervision of psychiatric care of the patient. All authors contributed to and approved the final manuscript.
Funding This work was supported by projects from National Natural Science Foundation of China (81971273, 81000588). Project of Shanghai Municipal Health Commission (GWV-10.2-XD28).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.