Article Text

Abstract
Background Methamphetamine (MA) is one of the most commonly abused illicit psychostimulant drugs and MA use disorder constitutes a universal health concern across the world. Despite many intervention approaches to MA use disorder, the indicator of addiction severity is mainly limited to subjective craving score to drug-related cues, which is influenced by many factors such as social approval and self-masking.
Aim The present study investigates whether self-reported craving for drug use in response to MA cues is a reliable indicator for addiction severity in MA users, and then tests the validity of the cue-induced attention bias test in addiction severity assessment.
Methods Fifty-two male MA users completed the cue-induced craving test and attention bias task, and were required to report clinical characteristics of addiction severity. For the attention bias test, subjects were required to discriminate the letter superimposed onto MA use-related or neutral scenes. The reaction time delay during MA-use condition relative to neutral condition was used as an index of the attention bias.
Results The results showed that 24 of the 52 MA users rated non-zero in cue-induced craving test, and they showed a significant attention bias to drug-related pictures. However, the other 28 users who rated zero in cue-induced craving evaluation showed a similar attention bias to drug-related cues. In addition, the attention bias to MA use-related cues was significantly and positively correlated with the clinical indexes of addiction severity, but the relationship was absent between subjective craving evaluation and the indexes of addiction severity.
Conclusion These results suggest that attention bias to MA cues may be a more reliable indicator than experiential craving report, especially when subjective craving is measured in the compulsory rehabilitation centre.
- methamphetamine
- addiction severity
- subjective craving
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Methamphetamine (MA) is one of the most commonly abused illicit psychostimulant drugs.1 MA user disorder is associated with paranoia, behavioural impulsivity and cognitive impairment.2 However, neither medication nor psychosocial treatment has been proven to effectively treat MA use disorder with regard to vulnerability for relapse.3 A number of factors are thought to contribute to relapse, including exposure to drug cues and addiction severity.4 Drug cues refer to things, people or situations that are associated with drug use, which may trigger drug seeking behavior.5 Despite many intervention approaches to MA use disorder, the indicator of addiction severity is mainly limited to the subjective craving score to drug-related cues,6 7 which is obscured by many factors such as social approval and self-masking.8
Cognitive models, such as the expectancy model, the dual-affect model and the cognitive processing model, all hold that external environmental events serve as triggers for drug use.9 For an individual addicted to a specific substance, stimuli associated with that substance will automatically capture attention whereas this is not evident in normal subjects. It has been indicated that the attention bias (AB) towards drug-related cues has a predictive role for drug relapse10 and may be an important factor in predicting drug abuse treatment outcome.11 Attention bias for drug-related cues can be measured directly by monitoring eye movements,12 or indirectly inferred with reaction time or other indicators.13 14 Indirect measures of attentional bias have largely made use of either of two tasks: the modified Stroop task and visual probe (dot-probe) task.15 16 Attentional bias is indicated by faster reaction times to probes that replace drug-related images, which has been generally applied in tobacco, opiate and cocaine use disorder studies. However, few studies have focused on the attention bias of methamphetamine users.11 Although direct measurement of attention bias may be done using eye-tracking, simple measures may be preferred for practical purposes and ease of administration (such as the high cost of eye-tracking equipment).
Furthermore, as subjects do not need to overtly assess how they are craving for drug use, the attention bias test should be independent of subjects’ attitude towards MA use or sociocultural influences. Consideration of these potential obscuring factors is particularly important in assessing addiction severity in MA users, as MA use is illegal across the world. In this regard, attention bias to drug cues may be a more objective and sensitive index for addiction severity. Currently, we use a modified visual probe task, which employs attentional bias as an indicator, to test how attention bias to drug cues may predict addiction severity in MA users.
Specifically, this study directly compared the results of self-report craving and drug-related attention bias, and we examined whether self-reported craving for drug cues is a reliable index for the detection of addiction severity in subjects with a long history of MA use disorder, and then tested whether the severity of addiction can be more sensitively and reliably assessed by the cue-induced attention bias test.
Methods
Participants
Fifty-two male individuals (aged 23–57 years, mean=35.54; SD=8.18 years) from Nanjing Compulsory Rehabilitation Center who met the Diagnostic and Statistical Manual of Mental Disorders criteria for MA use disorder (mean (MA use history)=4.55; SD=2.72 years) participated in this study.17 The inclusion criteria were (1) aged 20 to 60 years; (2) normal vision and hearing; (3) received no medications during treatment; (4) in compulsory abstinence from drug use for more than 1 month. The exclusion criteria were (1) serious physical or mental illness; (2) history of epilepsy. All the subjects participated in the study voluntarily.
The experimental procedure was in accordance with the ethical principles of the 1964 Declaration of Helsinki (World Medical Organization, 1996).
Data collection and measurements
Each subject completed a questionnaire (see figure 1), which included demographic characteristics and clinical characteristics of addiction severity involving MA use duration (years), maximum amount (g) and weekly amount (g). All the subjects completed the visual probe task and the cue-induced subjective craving evaluation with an inter-task interval for 5 minutes. Visual probe task preceded cue-induced craving paradigm in order to avoid potential amplifying effects of attention bias by prolonged presentation of MA-use scenarios.

Flowchart of the study. MA, methamphetamine; RT, reaction time.
Modified visual probe task
We used a modified visual probe task to assess MA-related attention bias (see figure 2). The modified visual probe task consisted of 60 trials. Each trial started with a jittered fixation varying from 800 to 1200 ms, which was followed by the presentation of task stimulus. The task stimuli contained 10 pictures (five neutral and five drug-related scenes) superimposed by a letter (W or M) in three different positions (top, centre, bottom). The two letters were presented with equal probability. The subjects were instructed to press ‘1’ or ‘2’ quickly and accurately for letter classification, regardless of the background picture. Attention bias to MA use relative to neutral scenes could be obtained by the reaction time delay between MA-related and neutral conditions.

Behavioural procedure of the modified visual probe task.
Cue-induced craving paradigm
In the craving test, a block-wise method was used to continuously present six MA use–related pictures (eg, MA-intake utensils, tools and the scenarios of MA intake) for 24 s (4 s each). The six pictures used in the cue-induced craving paradigm were not presented in the visual probe task. Participants were instructed to pay close attention to the picture and rated their level of craving after watching these pictures. Craving was assessed by visual analogue scales (VAS), with 0 (not at all) to 100 (extremely intense).
Data analysis
Subjective craving for MA use was measured as the score obtained on the VAS (possible range: 0–100). According to the subjective craving score, 52 subjects were divided into two groups (subjective craving score=0; subjective craving score >0), which signals diverse outcomes from subjective craving measurement.
As for the modified visual probe task, only the response time (reaction time; RT) on the correct trial was considered to be taken into the analyses of RT. RTs exceeding 3 SDs of the means of a given condition for a given participant were trimmed. We compared RT separately for the two groups (subjective craving score=0; subjective craving score >0) between neutral and drug-related scenes to verify the consistency of results between attention bias and subjective craving methods.
In addition, to assess the relationship among addiction severity, subjective drug craving and drug-related attention bias, we conducted tests of Pearson correlations, separately, between the clinical characteristics of addiction severity (MA use duration (years), maximum amount (g) and weekly amount (g)) and the two addiction measurements (subjective craving and attention bias).
The data were presented as mean (SD), and statistical analysis was performed with SPSS V.16.0 software. Repeated measures analysis of variance (ANOVA) model was used and p value <0.05 was considered statistically significant. We used two-tailed p values for these comparisons.
Results
Attention bias to drug-related situations in all subjects
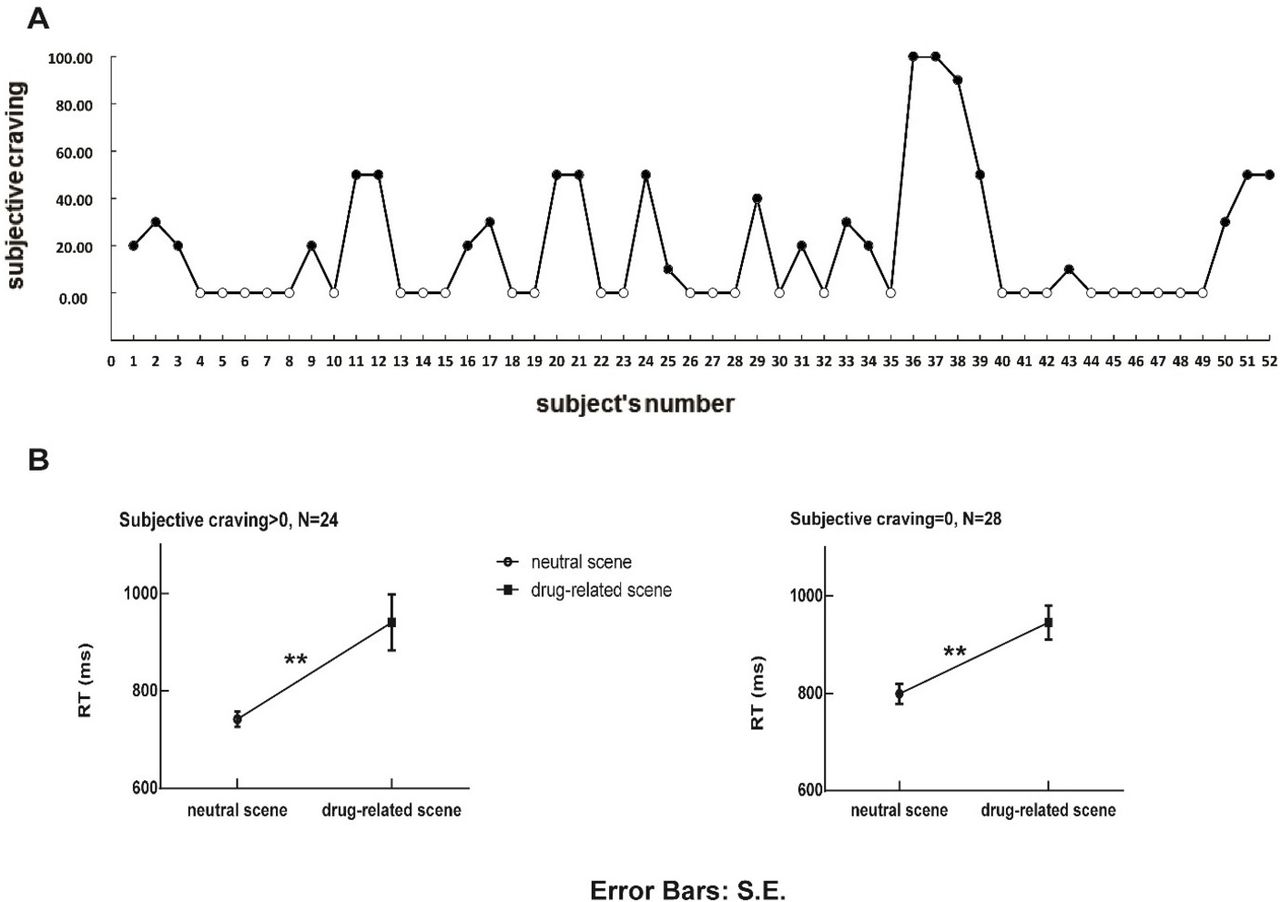
Fifty-two MA users rated subjective craving score after exposure to drug-related scenes, among whom 28 users rated zero in the subjective craving scale (see figure 3A). Users who rated zero were not distinct from users who rated non-zero in age, impulsiveness, emotion stability and clinical characteristics of addiction severity including MA use duration, maximum amount and weekly amount (see table 1).
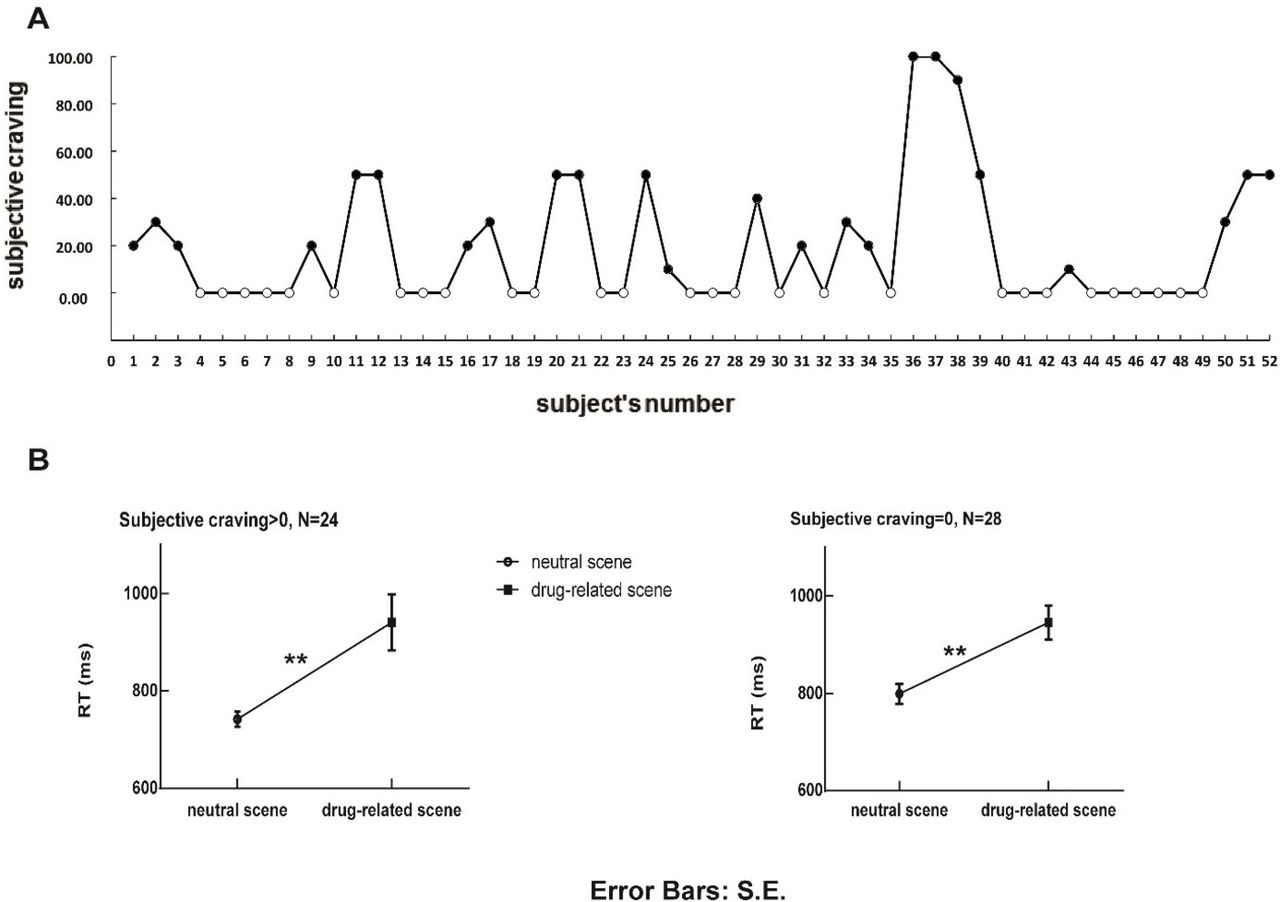
Data of all subjects in the subjective craving scale (N=52; A) and reaction time (RT) data in two groups (zero craving, non-zero craving) for each condition (neutral and drug-related situations) in the visual probe task (B). It is notable that methamphetamine users with non-zero craving (N=24) and zero-craving (N=28) both showed a significant attention bias, of a similar size (p=0.373), to drug-related cues (ps<0.001).
Demographic and clinical characteristics of methamphetamine dependents with zero and non-zero craving reports
The other 24 participants reported a craving score above zero (mean (SD)=41.25 (25.59)). The mean RTs (only from trials with correct responses) are shown in table 2. We performed an ANOVA of RTs with background scenes (two scenes: neutral, drug-related) as the repeated factor. The results showed a significant attention bias to drug-related scenes (mean (neutral)=742 (75.77) ms; mean (drug)=941 (279.25) ms; F(1,23)=16.76, p<0.001, η²p=0.42; see figure 2B). In addition, the subjects who reported zero (see figure 3B) in subjective craving scale, however, still showed a significant attention bias to drug-related situations in the visual probe test (mean (neutral)=799.21 (109.32); mean (drug)=945.50 (183.73); F(1,27)=18.14, p<0.001, η²p=0.40).
Reaction time data in two groups (zero craving, non-zero craving) for neutral and drug-related conditions in the visual probe task
Furthermore, the independent-samples t-test showed that the magnitude of attention bias to drug-related scenes was similar between users who rated zero and non-zero in cue-induced craving evaluation (t(50)=−0.89, p=0.373).
Relationship among craving, attention bias and addiction severity
Pearson’s product-moment correlation (see figure 4) was used to assess the relationship between subjective craving score, attention bias and addiction severity. The magnitude of the RT differences between drug-related and neutral conditions was used as the drug-related attention bias measure. The results (see table 3) showed that the attention bias measure was significantly correlated with all the clinical indexes related to addiction severity, involving MA use duration (r=0.336, p=0.015), maximum (r=0.388, p=0.005) and weekly amount of MA use (r=0.390, p=0.004). In contrast, there was no significant correlation between subjective craving score and drug use duration (r=−0.001, p=0.996), maximum amount (r=0.148, p=0.295) or weekly amount of MA use(r=0.107, p=0.449).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between the attention bias measure and addiction severity in methamphetamine use duration (history), maximum amount (one time) and weekly amount (A); and the association between subjective craving and addiction severity (B).
Correlation between index of two measures and addiction severity
Discussion
Main findings
Previous studies of addiction intervention mostly focused on reducing cue-induced subjective craving in drug users. However, subjective craving rating is susceptible to quite a few obscuring factors,18 19 such as self-report bias, and is easily subject to conscious self-control due to sociocultural influences. In addition, it is common that addicted persons fail to report cue-induced craving.20 In this study, we consistently found that more than half of the MA users reported no cue-elicited craving, but they showed a significant attention bias to MA-related scenes in the modified visual probe task. Attention bias for drug-related cues, an information processing bias for drug-related stimuli, has been reported to result in craving and substance use.21 In the current study, we directly compared the results between self-reported craving and RT delay for drug-related cues, but we failed to observe the consistency between attentional bias and subjective craving.
In addition, attention bias to drug cues was strongly correlated with MA use duration, and maximum and weekly amount of MA use, which are central indexes of addiction severity.22 However, the positive correlation was absent between subjective craving score and all the three clinical indexes of MA use disorder used in this study. It prompts that attentional bias test may be applied as a more reliable indicator than rated subjective craving in future addiction studies.
At present, there is evidence with other stimulant drugs,23 but not MA, that interventions aimed at manipulating attention biases do influence future drug use.24 In the current study, our findings further our understanding of attentional bias to MA-related cues in MA use disorder. Attention paid to drug-related cues could distract individuals from effective therapies and prohibit them from the employment of abstinence-oriented coping skills. Measurement of MA-related attention bias is of high clinical importance because of their close relation with addiction severity, indicated by the current correlation analyses.
Limitations
Several limitations need to be acknowledged. First, we used MA use duration, maximum amount and weekly amount to represent addiction severity. However, these three indexes may only represent addiction severity in part. There are multiple methods to assess addiction severity. For example, McLellan and colleagues22 invented the Addiction Severity Index to measure the severity of drug use disorder. However, this instrument gathers information on several addictive areas that participants experienced within the last 30 days. In the current study, we conducted the experiment in Nanjing Compulsory Rehabilitation Center, and all the participants were in compulsory abstinence from drug use for more than 1 month. Thus, instruments that assess addiction severity like this may be unfit for measuring addiction severity in our study. Future studies are still needed to establish standard and recognised instruments to assess addictive severity of MA subjects in compulsory detoxification institutes. Second, subjective craving is susceptible to social approval, especially when measured in a compulsory rehabilitation centre. We did not assess craving before picture presentation, based on the consideration that repeatedly measuring craving may enhance demand effect, which potentially contaminates the true cue-induced craving. However, we cannot assure that this is cue-induced craving because pretest craving was lacking. Third, in the current study, we used six MA-related pictures to induce subjective craving, which may be too short to induce intense craving. This may also explain why a large portion of subjects rated zero in their craving report. Nonetheless, given the robust attention bias effect in these zero-craving subjects, this explanation, again, suggests that attention bias test is a more sensitive index than craving report in assessing addictive severity. Lastly, MA-related pictures used in subjective craving paradigm and visual probe task were not standardised and recognised. Future studies are still needed to establish unified and effective stimulus datasets to induce craving.
Implications
On the one hand, future studies need to examine electrophysiological correlates of attention bias for MA use scenarios. In addition, attention bias tasks need to be performed during fMRI scan to find its neural underpinnings. On the other hand, the results of this study demonstrated a dissociation between the attentional bias and subjective craving, and we found a predictive role of attention bias for addiction severity, more specifically, in MA use disorder, which may contribute to the clinical use of attentional bias. Future studies should also explore why attention bias serves as a more reliable indicator of addiction severity than experiential craving.
References
Qiongdan Liang, a first year PhD student in Tsinghua University, major in psychology.She got bachelor’s degree in Shaanxi Normal University and a master’s degree in South West University (China). Her research interests include drug addiction and behavioral inhibition.

Footnotes
Contributors QL contributed to the experiment conduction, data analysis, and manuscript preparation. TY contributed to the manuscript revision. JYu contributed to study design, data analysis, manuscript writing and supervised the whole project. XC contributed to the data collection and experiment conduction. HH contributed to the data collection. JYa contributed to the data analysis.
Funding This study was funded by the National Natural Science Foundation of China (grant no. 31871103; 31671164).
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval This study was approved by the Ethics Committee of Southwest University in China.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.